











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkAt the beginning of the 21st century, the comprehensive management of chronic non-communicable diseases (CNCDs) became a priority for governments worldwide, given its effects both on the sustainability of national health systems and the productivity and wellbeing of humanity.1-4
Among CNCDs, cancer plays a significant role because of its connections to both the aging population and urban lifestyles.5 Cancer presents three challenges to the financial sustainability approach. First, estimates are needed of the funding necessary to treat the increasing number of patients who require medical care in the medium term.2,4 Second, the indirect costs generated by disability, pensions, non-medical patient care, and premature deaths among the working-age population (WAP) with cancer must be determined.6,7 Finally, the funding needed to implement prevention and timely detection actions must be assessed, and the potential savings that these actions would generate in the medium and long terms must be estimated.4
Although the economics of providing medical services to patients with specific cancers has been addressed internationally, few studies have analyzed the indirect cost associated with these diseases.8-10 Specific studies have been published in Mexico to determine the medical care costs associated with breast cancer, lung cancer, and cervical-uterine cancer.11-14 In addition, institutions such as the Popular Health Insurance (Seguro Popular de Salud; SPS) and the Mexican Social Security Institute (Instituto Mexicano del Seguro Social; IMSS) have developed cost systems to quantify various cancers funded with public resources by stage.15,16 Likewise, publications including cost-effectiveness analyses of preventative actions exist for cervical-uterine cancer and breast cancer cases in Mexico.17,18 However, no published studies have estimated the indirect costs associated with cancer in Mexico.
Because of the importance of economic analyses regarding cancer in Mexico, this study aimed to provide an estimate of the indirect costs derived from this set of diseases among Mexican adults between 2002 and 2020.
Materials and methods
The indirect costs associated with patients with cancer are estimated as the sum of the costs generated by income lost due to premature death (ILPD), short-term benefits (STBs), invalidity/disability pensions (DPs), and the opportunity costs of the non-medical carer (OCCs). The method for calculating the indirect cost components has been used to quantify the indirect costs of cancer in other countries and the indirect costs of other conditions in Mexico.8,19 All calculations were performed with regard to gender in the WAP, defined as individuals aged between 15 and 64 years according to the Federal Labor Law (Ley Federal del Trabajo; LFT) and the Social Security Law (Ley del Seguro Social; LSS), which was in forced in 2013.6-7 A description of the sources of data and calculation method for each of the indirect cost components is presented in Table 1. A detailed description of the calculation can be found in an upcoming work.20 The analysis was performed using R version 3.1 from July 2014 to June 2015.
Table I Description of the indirect cost components generated by patients with cancer
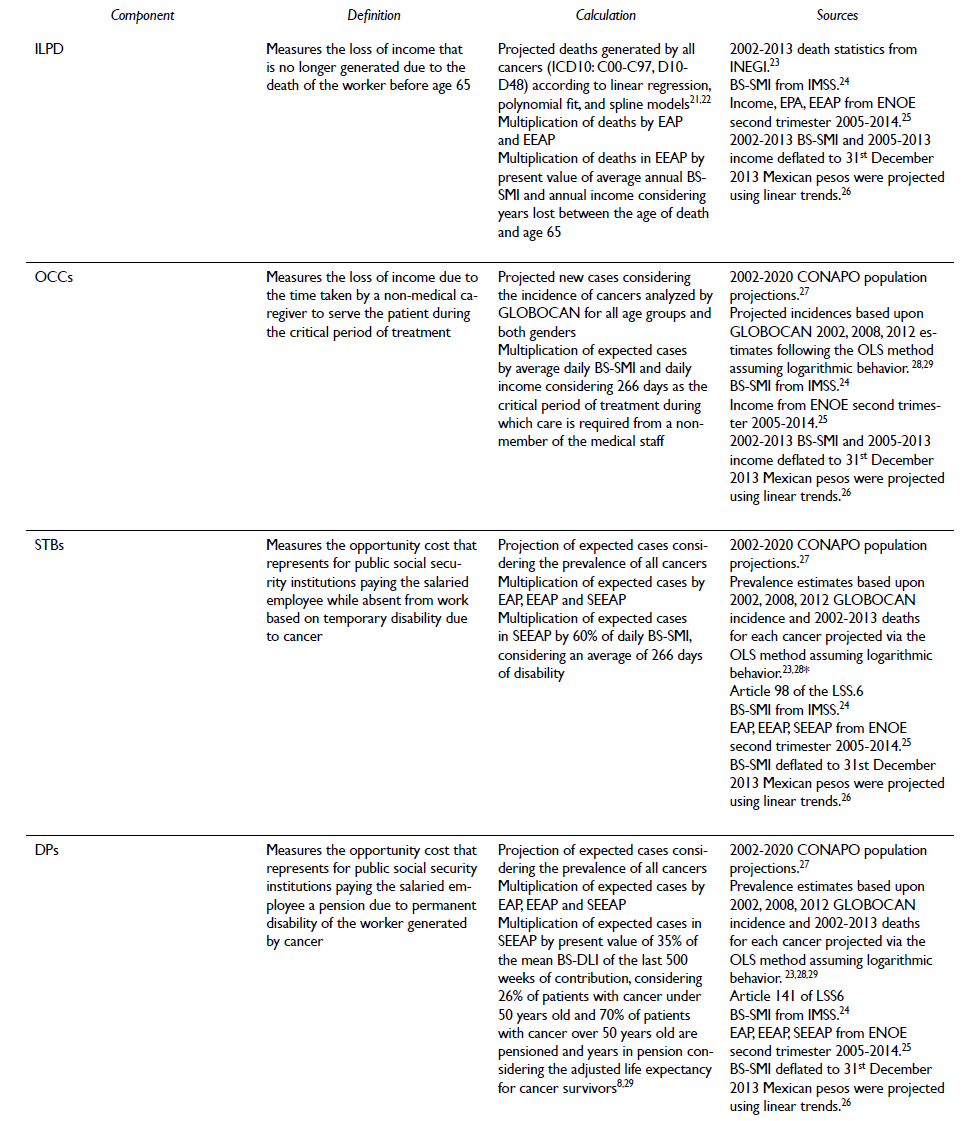
ILPD: income lost for premature death; OCC: opportunity cost for the carer; STB: short-term benefit; DP: disability pension; BS: base salary; SMI: sickness and maternity insurance; DLI: disability and life insurance; EAP: proportion of economically active population; EEAP: proportion of employed economically active population; SEEAP: proportion of salaried employed economically active population; LSS: social security law (acronym in Spanish).
* Reynoso-Noverón N, Armas-Texta D, Gutiérrez-Delgado C, Lasa-Gonsebatt F, Mohar-Betancourt A. Cancer Epidemiology: The challenge of the epidemiological surveillance system in Mexico. Unpublished paper.
Results
Population projections indicate that, on annual average, 72.7 million WAP individuals will live in Mexico from 2002 to 2020. Approximately 77% of the men and 42% of the women in the WAP comprised the economically active population (EAP) between 2005 and 2013. In addition, 95% of the EAP was employed (EEAP), and 61% was salaried (SEEAP) on average. The SEEAP represents approximately 40% of the men and just over 23% of the women in the WAP. The proportions of SEEAP, which under the framework of the LSS (in forced in 2013) are entitled to financial benefits, indicate that the effects that STBs and DPs will have on the indirect cost will be modest compared with those of ILPD and OCCs. Figure 1 shows the mean percentage distribution of the EAP, EEAP and SEEAP by age and gender. These distributions allow speculation with regard to the contribution of the patients whose demographic structure will affect ILPD, STBs and DPs; specifically, the contribution of females will be, on average, half the contribution of males for all age groups.
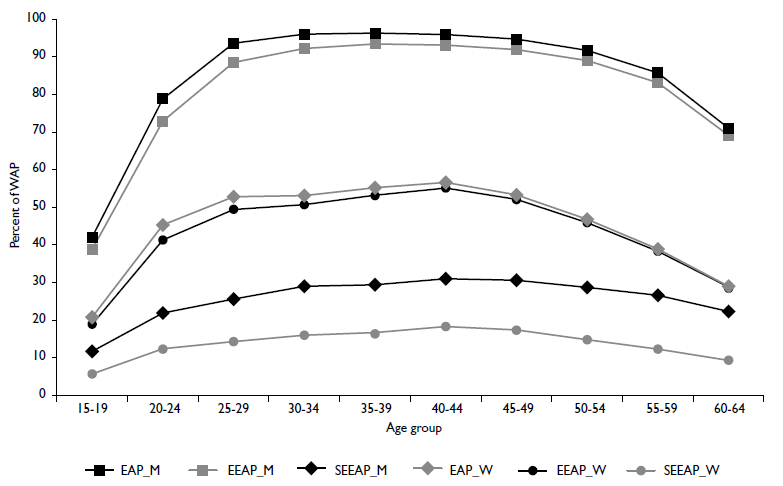
EAP: economically active population; EEAP: employed economically active population; SEEAP: salaried employed economically active population; M: men; W: women; WAP: Working age population.
Source: Authors' calculations using ENOE data, second trimester 2005-2013 INEGI.25 For the calculations, the 2014-2020 behavior was assumed to be similar to the 2005-2013 behavior, and the 2002-2004 behavior was assumed to be similar to the 2010-2013 behavior.
Figure I Average EAP, EEAP and SEEPA percentages by age and gender in Mexico, 2002-2020
Figure 2 shows both the number of expected deaths that generate ILPD and the expected cases that will generate STBs, DPs, and OCCs over the analysis period. A growing trend was observed for all cases, which primarily reflects the aging Mexican population. Importantly, the number of non-medical caregivers is especially high given that one caregiver was considered in the calculation for each new case of cancer without a patient age restriction.
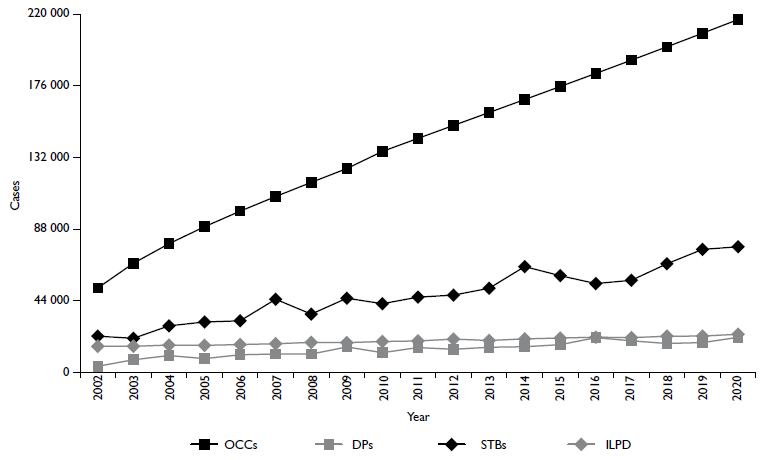
STBs: short term benefit; DPs: invalidity/disability pension; OCCs: opportunity cost for the carer; ILPD: income lost due to premature death
Source: The authors' calculations were based on the Conapo and ENOE data, second trimester 2005-2013 INEGI. 25 For the calculations, the 2014-2020 behavior was assumed to be similar to the 2005-2013 behavior, and the 2002-2004 behavior was assumed to be similar to the 2010-2013 behavior.
Figure 2 Deaths and expected Cancer cases generating ILPD, STBs, DPs, and OCCs in Mexico from 2002-2020
We estimated that 20 526 deaths by cancer would occur in the EEAP in 2014 (95% CIs=20 053-20 999), and 605 758 cases of cancer would exist in the total population (95% CIs=540 665-670 852), of which 167 534 would be new cases (95% CIs=165 205-169 864). Based on these figures, 60.96% (95% CIs=60.20%-61.73%) of the deaths and 41.46% (95% CIs=41.91-48.01) of prevalent cases will be men. If the trend observed up to 2013 continues, deaths by cancer in the WAP could rise to 23 359 by 2020 (95% CIs=22 775-23 943), and the number of prevalent cancer cases in the entire population could double to 1 262 861 (95% CIs=(1 079 419-1 446 303), of which 216 679 (95% CIs=213 145-220 214) would be new cases. Once again, men will comprise the highest percentage of deaths 58.30% (95%CIs=57.54%-59.07%), and women will comprise 57.33% of the prevalent cases (95% CIs=(51.62%-62.92%) in the entire population.
In terms of the income considered in the indirect cost calculation, the base salary for the Sickness and Maternity Insurance (BS-SMI) and Disability and Life Insurance (BS-DLI) of the IMSS were greater than the income reported by the non-salaried EEAP (NSEEAP). Figure 3 shows the mean BS-SMI and BS-DLI amounts and income as well as the mean income distribution by age and gender. We estimated that the mean difference between BS and income was 59%, although it is projected that this difference will significantly decrease over time. Moreover, average differences of 3% and 25% were observed among the age groups and between genders, respectively. An average difference of 45% was observed between the income of the 15- to 19-year-old age group and that of all age groups. These differences help explain the monetary contribution that the demographic structure of the WAP contributes to the different indirect cost components.
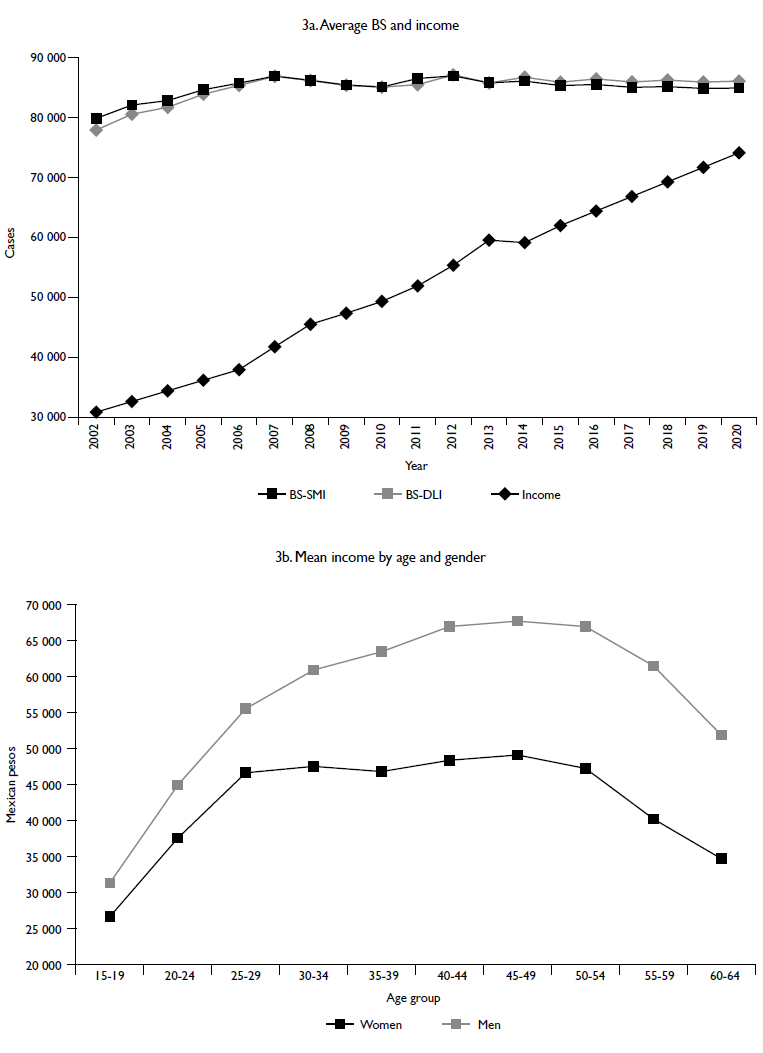
BS: base salary; SMI: sickness and maternity insurance; DLI: disability and life insurance; IMSS: Mexican Social Security Institute (Instituto Mexicano del Seguro Social)
Source: The authors' calculations were based on the ENOE data, second trimester 2005-2013 INEGI and data from the IMSS statistical report. For the calculations, the 2014-2020 behavior was assumed to be similar to the 2005-2013 behavior, and the 2002-2004 behavior was assumed to be similar to the 2010-2013 behavior.
Figure 3 Average incomes used to calculate the indirect costs by age and gender in Mexico from 2002-2020
Figure 4 shows the annual amounts of the indirect cost components for the analysis period considering all of the available information and applying the methodology presented in table I. The estimated ILPD for 2014 was 9.985 billion Mexican pesos (bMXN; 95% CIs=9.628-10.343), whereas it will be 12.121 bMXN in 2020 (95% CIs=10.399-13.843). Men comprised the largest group (66.78%) in the total population (95% CIs=63.57-70). These results are consistent with the fact that the population projections are higher for women, although their participation in the EAP has been lower historically. The results are also consistent with the gender difference in income (Figure 4a).
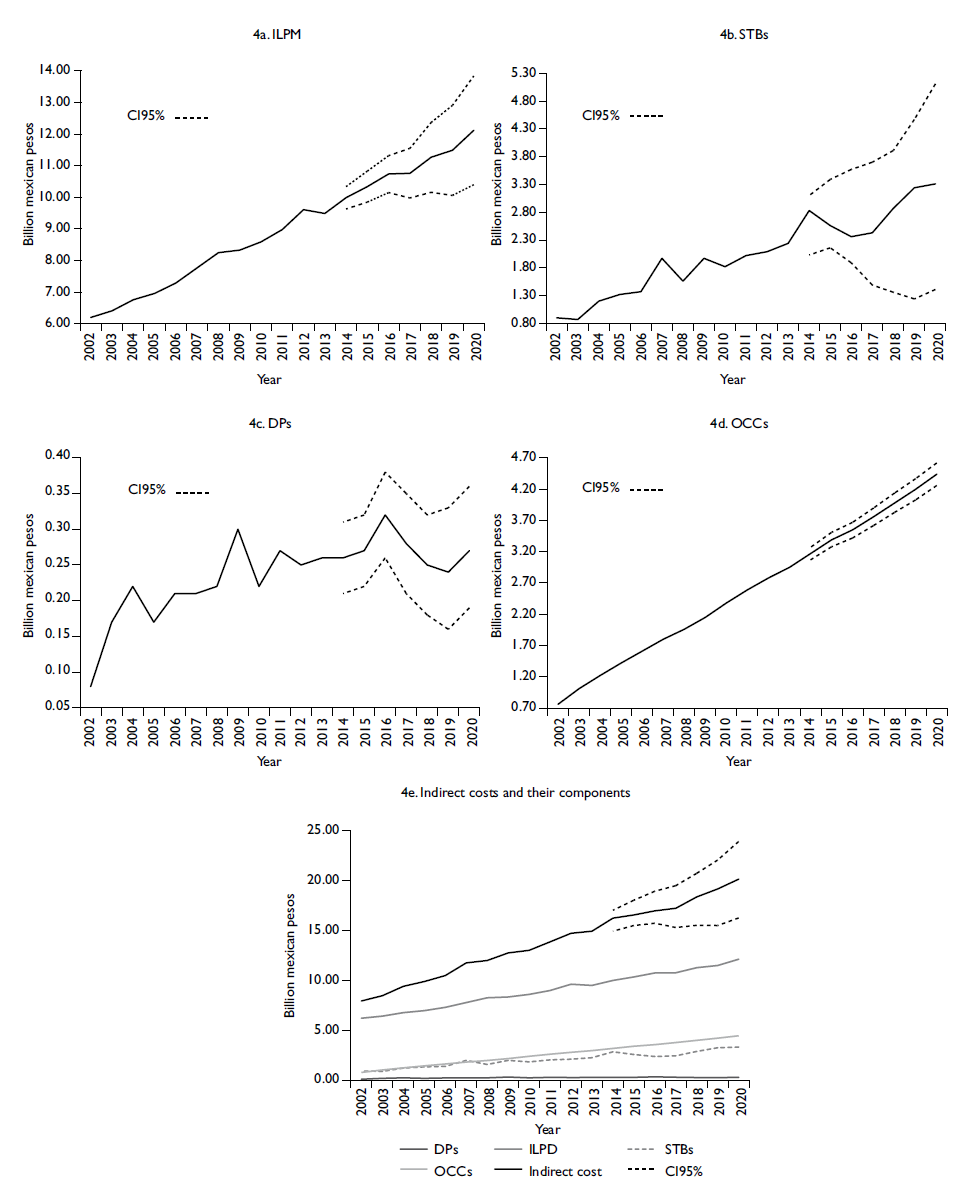
ILPD: income lost due to premature death; STBs: short term benefits; DPs: invalidity/disability pensions; OCCs: opportunity costs for the carer
Note: Figures in Mexican pesos must be multiplied by 1 000 and be read as "miles de millones de pesos" in the Spanish translation
Source: The authors' calculations were based on the INEGI, Conapo, and IMSS datasets.
Figure 4 Indirect costs due to cancer cases in Mexico from 2002-2020
The estimated STBs will be 2.828 bMXN (95% CIs=2.030-3.104) in 2014, and the respective projection for 2020 is 3.315 bMXN (95% CIs=(1.410-5.106). In this case, women comprised the largest group with an estimated percentage of 54.56% of the total population (95% CIs=51.22-57.90; Figure 4b).
The cost estimated for DPs in 2014 was 258 million MXN (mMXN; 95% CIs=208-308), and that estimated for 2020 was 275 mMXN (95% CIs=191-358). Once again, women comprised the largest group with an estimated percentage of 62.30% of the total population (95% CIs=59.00-65.60; Figure 4c).
Finally, the estimated OCCs in 2014 were 3.171 bMXN (95% CIs=3.068-3.274), and the 2020 estimate was 4.437 bMXN (95% CIs=4.256-4.619). Women would generate the highest percentage of patients requiring non-medical care and thus the highest OCC with 53.5% of the total cases (95% CIs=50.22-57.17; Figure 4d).
Therefore, the indirect costs estimated using the available data were 16.242 bMXN (95% CIs=14.933-17.028) in 2014. Based on this projection, the indirect costs will reach 20.148 bMXN (95% CIs=16.256-23.926) by 2020, of which 54.9% corresponds to men (Figure 4e).
Discussion
This study is the first to estimate the indirect cost associated with cancer in the Mexican WAP from 2002-2020. This estimate included ILPD, STBs, and DPs payments as well as the OCCs generated by patients with cancer. The estimate was made mainly using data from Mexican public sources and the legal social security framework in forced in 2013. The estimate reflects the conditions of the Mexican labor market for the EEAP with respect to ILPD and for the SEEAP with respect to STBs and DPs. Furthermore, it shows the economic effect that Mexican society is absorbing in the case of OCCs. Our estimates show that ILPD and OCCs contribute more than 80% of the total indirect costs, followed by STBs and DPs. The observed and projected trends indicate that the indirect costs due to cancer will fluctuate around 20.148 bMXN in 2020.
The method used to calculate the indirect cost components followed international standards applicable to this type of study. A major limiting factor for this study was the source of information used to estimate the prevalence and incidence of cancer. This limitation is because of the lack of a national population-based registry for patients with cancer in Mexico when the analysis was performed. This limitation was resolved using the International Agency for Research on Cancer (GLOBOCAN) incidence estimates, which are based on standard methodologies that consider the recorded national population data from other countries in Latin America. Although the epidemiological structure of cancer in Latin America is likely similar to that of Mexico, the effects of Mexican programs concerning prevention, detection, diagnosis, and treatment for some of the most common cancers in the country might not be reflected in the Latin America data potentially overestimating the GLOBOCAN incidence for the Mexican case.
The variation in the amounts between the BS and income might be partially because income was self-reported in the National Occupancy and Employment Survey (Encuesta Nacional de Ocupación y Empleo; ENOE), whereas the BS values came from data reported to the IMSS by employers for social security tax payments. This variation causes the indirect costs to be underestimated and therefore represents the floor of the actual value they might reach.
Our projections reflect the aging population and show a modest upward trend in the BS, assuming that the incidence, prevalence, and mortality rates of cancer, as well as the salary growth rate, maintain the projected trend. With a greater change in these concepts, the study results would represent the floor of the indirect costs of cancers.
The estimate of the OCC assumes that patients' caregivers lose the opportunity to generate income from work during the critical period of cancer treatment. This assumption might generate controversy because in Mexican society, patient care often falls on a family member who belongs to the WAP but is not part of the EEAP. Moreover, no subsidy exists to support the non-medical caregiver under the social security framework in force since 2013; thus, it is important to consider the possibility of a subsidy scheme being established based on best practices reported by the Organization for Economic Cooperation and Development under the scheme of long term care in the near future.30 In this context, the OCC estimates presented represent a possible scenario for the number of caregivers and the amount that they might receive for their labor.
Considering the results of the current study, the following public policies to control and eventually decrease the indirect costs of cancer in Mexico are suggested.
Create and maintain a national population-based registry of patients with cancer. This registry will allow researchers to obtain more precise incidence and prevalence rates to help improve indirect and direct cost estimates. In addition, this registry will have valuable information to plan resources within the National Health System regarding cancer.
Strengthen the link between the prevention and early detection programs of different cancers, including early treatment and follow-up assessments as well as palliative care and rehabilitation until medical discharge. This strengthening will generate significant savings in the medium term and long term by treating patients with earlier stages of cancer and therefore shortening disability times and reducing mortality.
Analyze the feasibility of extending social security economic benefits coverage by adjusting the legislation in force since 2013 to consider affiliation and sustainable funding schemes to enable the NSEEAP to access STBs and DPs in case of illness or permanent disability from cancer.
Consider the eventual establishment of a subsidy for long-term care under a sustainable financial scheme. This subsidy will be required more urgently as Mexican family structures decrease and do not count on any one member to face long periods without income. In addition, this subsidy might help bridge the current financial inequity gap with regard to accessing existing long-term care.
Finally, it is important to emphasize that indirect costs should be one of the key components in any analysis of the total economic effect of diseases and risk factors at the population level. This cost must be complemented by an analysis of the direct costs associated with the necessary medical care of all cancers in the general population. This analysis will be addressed in a future study.

