











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkWorldwide, breast cancer (BC) is the most common cancer among women. In 2012, more than 1.67 million new cases were diagnosed, representing one in four cancers among women (25.2%) and 12% of all cancers.1 Breast cancer is the fifth leading cause of cancer death worldwide. This disease causes approximately 522 000 deaths per year, and in the case of women, it represents the most common cause of cancer death.1 In Latin America and the Caribbean, 27% of new cancer cases and 15% of cancer deaths are due to BC.1,2
Although Mexico is one of the 10 countries with the lowest incidence and mortality rates in the Americas,1,2 standardized mortality rates per 100 000 women aged 25 years and older in 2009 ranged between 9.10 and 26.69 in the individual states.3 A trend of increasing standardized mortality rates, which rose from 11.7 to 17.0 deaths per 100 000 women aged 25 years and over between 1980 and 2009, was observed.3
There are no figures available on the incidence of BC because Mexico does not have a histopathological cancer registry. However, less than 10% of BC cases are estimated to be detected in a timely manner.4,5 and 50-80% of those cases are found in advanced stages.5,6 In Mexico5,7,8 and other countries,9-12 low screening coverage13 and diagnostic delay cause lower survival, lower quality of life, less efficient use of resources and, above all, increased mortality.
A policy that reformed the Mexican health system was established in 2003.14 The System of Social Protection in Health (Sistema de Protección Social en Salud, SPSS) was established. SPSS provisions entered into force in 2004. The main financial component of SPSS is voluntary public insurance, known as Popular Insurance (Seguro Popular).15 Another component of the SPSS is the Fund for Protection against Catastrophic Expenditures (Fondo de Protrección contra Gastos Catastróficos, FPGC), which aims to support the Mexican population that lacks any health insurance scheme in the care of high-cost diseases and those that cause catastrophic expenditures.14-16 In 2007, a comprehensive BC treatment was included in the FPGC and thereby guaranteed that Mexican women with BC have access to comprehensive and free medical care in units certified by the SPSS.14
A greater increase in the number of hospital discharges in hospitals affiliated with the SPSS than in the social security hospitals could be expected due to the decrease of financial barriers through the incorporation of BC into the FPGC; consequently, a decrease in BC mortality rates should be expected.17 In this context, the aim of this study was to examine the trends in hospital discharges and mortality by BC in Mexico from 2004 to 2012 according to insurance scheme to identify the medium-term changes that have been caused by the inclusion of the comprehensive BC treatment into the FPCE of the SPSS since 2007.
Materials and methods
Design
An ecological study was conducted to compare trends in hospital discharges and mortality from BC in Mexico from 2004 to 2012 among women aged 25 years and older, according to insurance scheme before and after the inclusion of the comprehensive BC treatment into the FPGC of the SPSS in 2007. This period was chosen because the SPSS entered into force in 2004 and based on the availability of hospital databases at the time the analysis was performed.
Information sources
Data on hospital discharge and mortality in the period 2004-2012 were disaggregated by age, federal state and insurance scheme. Databases in dynamic cube format, which are available on the website of the General Directorate of Health Information (Dirección General de Información en Salud, DGIS) of the National Health Information System, constituted the data source.18 The International Statistical Classification of Diseases and Related Health Problems (CIE-10) code C50 was used to identify the pathology of interest. Projections of the female population disaggregated by age, federal state and insurance scheme for the years 1998-2011 and 2010-2015, conducted by the College of Mexico and the National Population Council (Consejo Nacional de Población, Conapo), were also used.18 The marginalization index estimated by the Conapo19 was included in the analysis to include the heterogeneity of socioeconomic development between federative states. The study was authorized by the ethics and research committees of the National Institute of Public Health (Instituto Nacional de Salud Pública, INSP) record number 774.
Information analysis
Information tables about women with BC aged 25 years or older were built per year, federal state and insurance scheme with data from the databases, drawing from discharge and mortality information. Discharges and deaths with unspecified age (0.006 and 0.057%, respectively) were excluded. Specific mortality rates among age groups of women aged 25 years and older were calculated at the national and federative state levels. For comparison purposes, it was standardized for age* within each group. Subsequently, the rates were adjusted by the direct method to eliminate the effects of any age difference between the insurance scheme, the federative states and the analyzed years.20 The standard population corresponded to the combined populations of women aged 25 or older per analyzed year, nationally and by federative state. The annual percentage change was used to assess trends, and statistical significance was estimated using joinpoint** models.
Results
Hospital discharges for breast cancer
Nationally, joinpoint analysis allowed the two increase periods for uninsured women (UW), 2003-2007 and 2007-2012, to be distinguished, with mean annual increases of 0.9% (p=0.9) and 34.2% (p<0.05), respectively.
For insured women (IW), these percentages were 3.3% (p<0.05) and 4.2% (p<0.05), respectively (figure 1). The numbers of hospital discharges by federative state are shown in table I. During 2004-2009, the Federal District, Veracruz and Jalisco were highlighted as the states that concentrated the largest numbers of hospital discharges for BC. However, the increase was remarkable since 2009 for Jalisco and 2010 for Michoacan. As a result, from 2007 to 2012, the percentages of the mean annual increase of hospital discharge numbers nationwide and among UW were 14.8% (p<0.05) and 34.2% (p<0.05), respectively. By excluding the states of Michoacan and Jalisco, this trend continued, but at lower rates: 5.4% (p<0.05) and 9.8% (p<0.05), respectively.
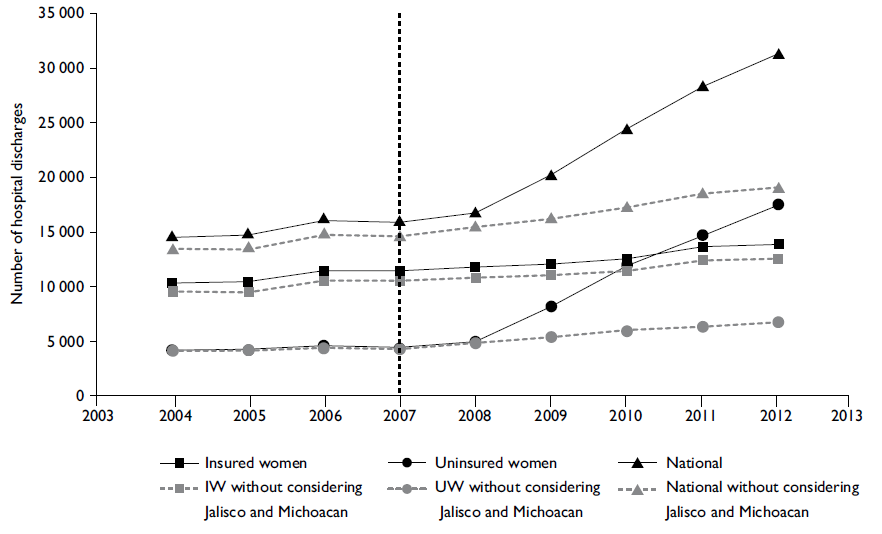
IW: Insured women (affiliated to the health services of the Mexican Social Security Institute, Institute for Social Security and Services for State Workers, Pemex, Navy Ministry or National Defense Ministry)
UW: Uninsured women (without any insurance scheme and affiliated with the System of Social Protection in Health)
Source: own calculations from the sectoral databases of hospital discharges, 2004-2012, General Direction of Health Information/Health Secretariat.
Figure I Hospital discharges in women with breast cancer aged 25 years or older, according to insurance scheme. Mexico, 2004-2012
Table I Hospital discharges in women with breast cancer aged 25 years or older, according to insurance scheme and Federative state. Mexico, 2004-2012
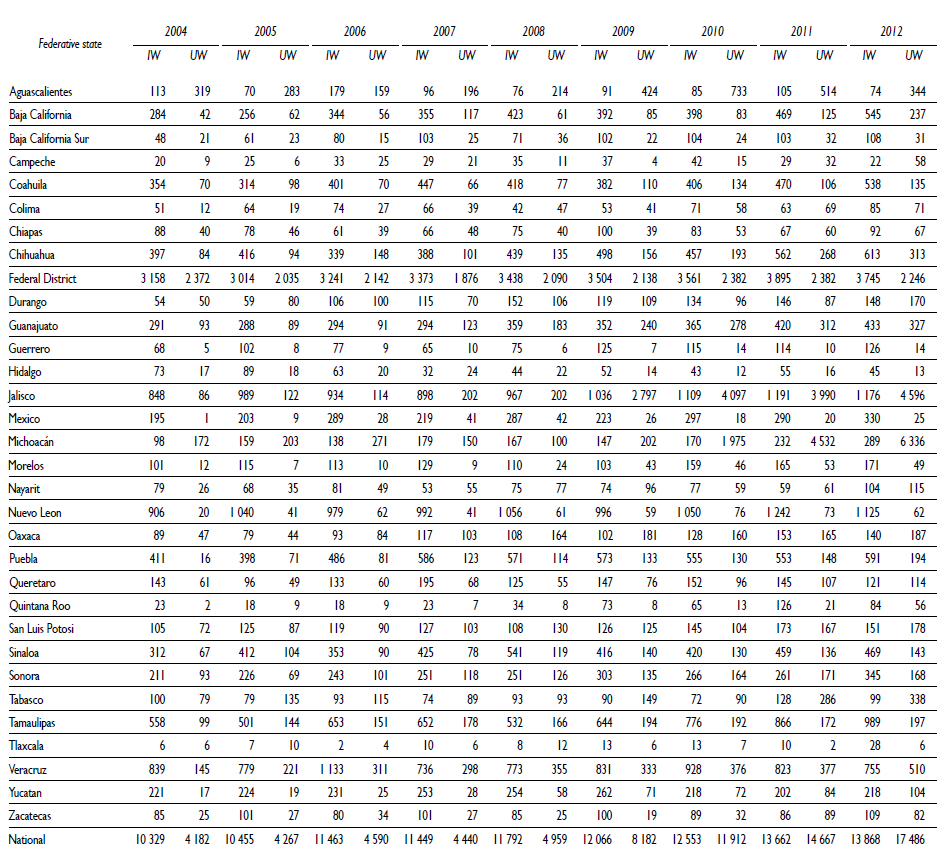
IW: Insured women (Mexican Social Security Institute, Institute for Social Security and Services for State Workers, Pemex, Navy Ministry or National Defense Ministry)
UW: Uninsured women (without any insurance scheme and affiliated with the System of Social Protection in Health)
Source: own calculations from the sectoral databases of hospital discharges, 2004-2012, General Direction of Health Information/Health Secretariat.
Breast cancer mortality
The number of breast cancer deaths at the national level also showed an upward trend during the periods 2004-2007 and 2007-2012 (figure 2a), with annual rates of 3.4% (p<0.05) and 3.9% (p<0.05). The analysis of mortality among women with and without social security showed that mortality was higher in IW; however, the annual growth rate during 2004-2007 was higher (4.2%, p=0.3) in the UW group than in the the IW group (2.4%, p<0.05). After 2007, deaths reached a higher rate in the UW group, with an annual growth rate of 7.1% (p<0.05), while the death rate was 2.9% (p<0.05) in the IW group.
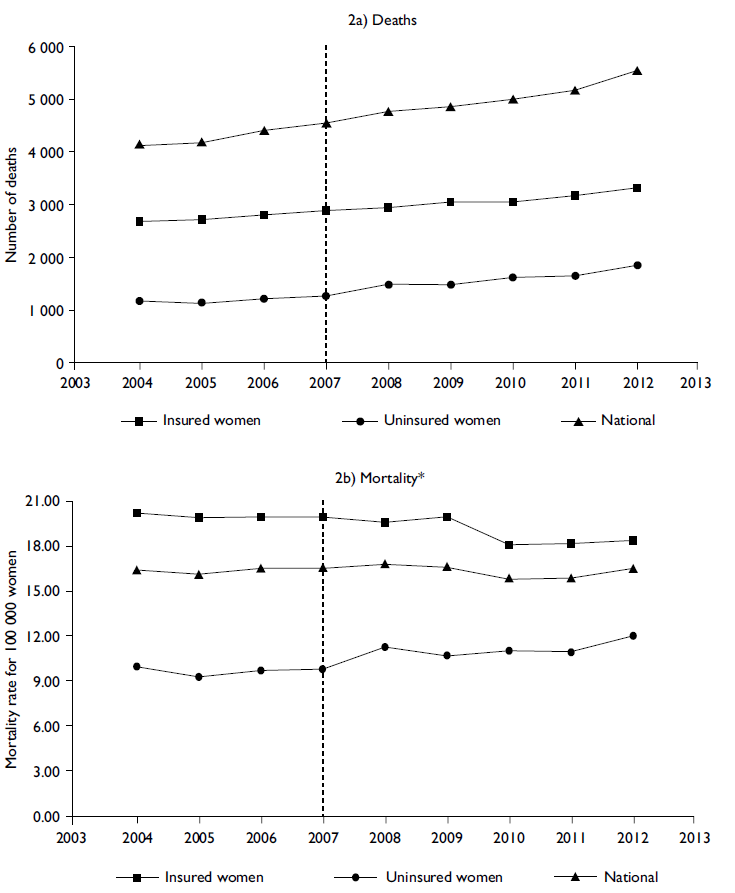
IW: Insured women (affiliated to the health services of the Mexican Social Security Institute, Institute for Social Security and Services for State Workers, Pemex, Navy Ministry or National Defense Ministry)
UW: Uninsured women (without any insurance scheme and affiliated with the System of Social Protection in Health)
*Age-standardized rates
Source: own calculations from the mortality databases, 2004-2012, General Direction of Health Information/Health Secretariat. Insured population projections for 1998-2011 and 2010-2015, National Population Council / General Directorate of Health Information.
Figure 2 Deaths and mortality* by breast cancer in women aged 25 years or older, by insurance scheme. Mexico, 2004-2012
The mortality rates standardized by age in 25-year-old women or older show that mortality remained constant over the 2004-2012 period nationally (figure 2b). However, when analyzed by insurance scheme, the mortality rates of the IW group were above the national rates, opposite to the situation seen with the rates in UW. For IW, joinpoint analysis allowed the observation that the annual mortality rate remained constant for the 2004-2007 period; however, an annual percentage change of -1.9% (p=0.1) was observed for the 2007-2012 period. In contrast, in UW, although the annual mortality rate was also constant from 2004 to 2007, for the second period, a percentage of annual growth of 3.3% (p<0.05) was observed. The adjusted mortality rates by federative state were higher in the IW group than in UW; this finding agrees with nationwide results (table II).
Table II Breast cancer* mortality in women aged 25 years or older, age-standardized, by insurance scheme and federative state. Mexico, 2004-2012

* Mortality rate per 100 000 women aged 25 years or older
IW: Insured women (affiliated to the health services of the Mexican Social Security Institute, Institute for Social Security and Services for State Workers, Pemex, Navy Ministry or National Defense Ministry)
UW: Uninsured women (without any insurance scheme and affiliated with the System of Social Protection in Health)
Source: Own calculations from mortality databases, 2004-2012, General Direction of Health Information/Health Secretariat. Insured population projections for 1998-2011 and 2010-2015, National Population Council / General Directorate of Health Information.
In general, the distribution of mortality rates by federative state indicates that BC remained constant until prior to 2007. From that year, the trends varied considerably, especially in those states with the highest marginalization rate (figure 3a). This finding is consistent with what is shown in figure 3b, which suggests a decreasing trend in BC mortality in women aged 25 years or older as the marginalization rate increases (2012).
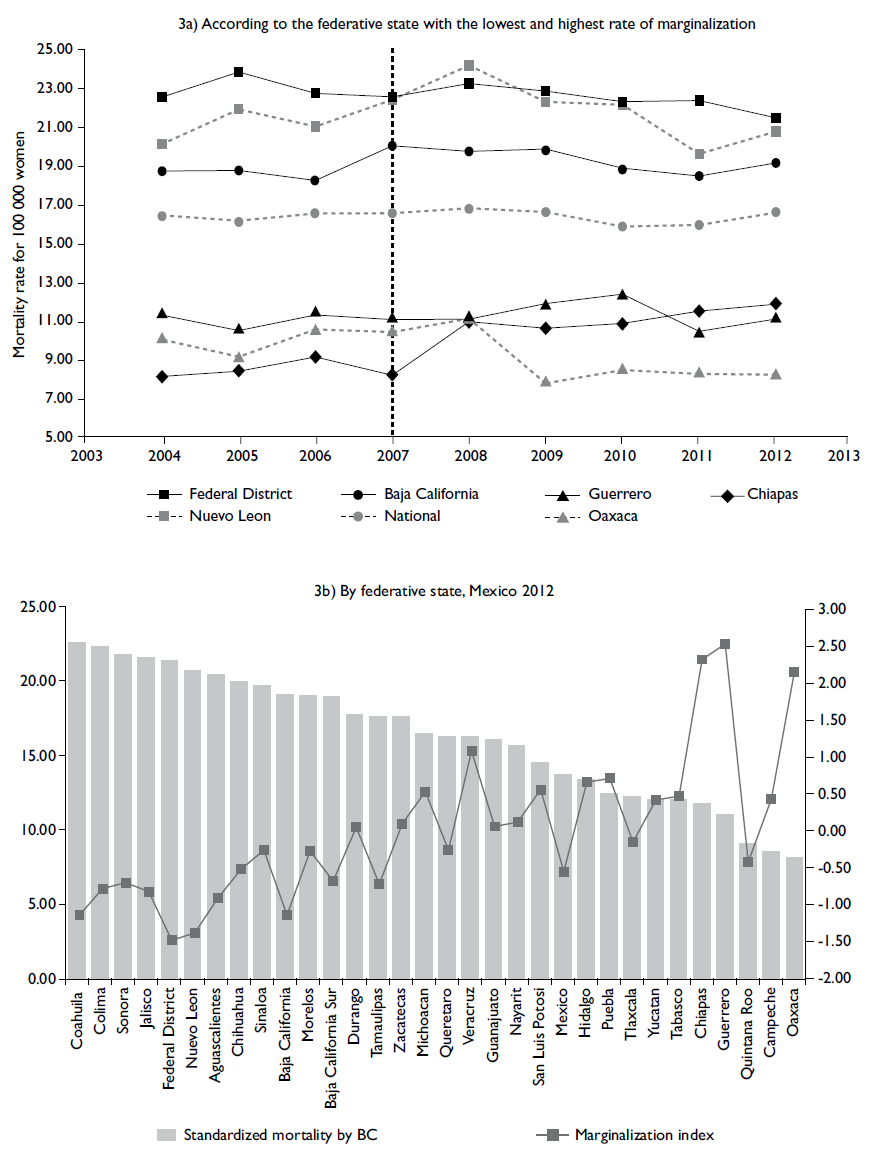
*Aged-standardized rate
Source: own calculations from mortality databases 2012, General Direction of Health Information/Health Secretariat. Insured population projections 2010-2015, Marginalization index data. National Population Council/General Directorate of Health Information, 2010
Figure 3 Breast cancer* and marginalization index in women aged 25 years or older, by federative state. Mexico, 2004-2012
Discussion
Nationally, a growing trend of hospital discharges was observed, particularly in UW, whereas mortality rates standardized by age in 25-year-old or older women remained constant. However, these rates decreased in IW from 2009, while in UW, rates increased from 2007. In addition, mortality rates were higher in federative states with low marginalization levels than in states with high marginalization levels.
The results of this study show an increase in the number of hospital discharges for BC from the inclusion of the comprehensive BC treatment into the FPGC. This result is consistent with the findings of an initial assessment of the SPSS impact conducted by Gakidou and colleagues.21 They reported that municipalities with high levels of SPSS affiliation had higher rates of hospitalization, and the impact was greater when it accounted for conditions included in the FPGC. However, higher increases in the states of Michoacan and Jalisco were noted, which could result from a difference from the other states in terms of the hospitalization criteria. Similarly, other studies have shown an increase in the use of public hospital services associated with an increased SPSS affiliation,22,23 which is more pronounced when the condition is included in the FPGC.24 This finding is consistent with studies stating that when removing financial barriers to access the health services, there is an increased utilization of hospital health services, particularly in populations that did not use these services previously.25,26
The number of deaths and the mortality rates experienced growing trends nationwide, which contrasts with expected results given the greater availability and access to health services.27,28 Studies in other countries have suggested, after a reform in the health system, that the health coverage improvement increases the use of services and decreases mortality.29-31 However, this reduction is hampered by inequalities in education30,32 and socioeconomic levels.29,32 Thus, in Mexico, Bautista-Arredondo et al.32 found that people with lower education levels and who are poorer are less likely to access outpatient medical services, even if the service is a beneficiary of SPSS. This finding suggests that the coverage of social health protection is a necessary but insufficient condition to reduce inequalities in access to primary outpatient care. This factor may be one reason why such a result in this study was not found, as most members of the SPSS are located in groups with social inequalities. Another possible explanation is that breast cancer in women is detected at an advanced clinical stage; thus, improvements should be incorporated in terms of access, screening by mammography, and the timeliness of diagnosis and treatment. Another explanation could correspond to the fact that FPGC covers only the costs of the disease; however, the infrastructure, equipment and the number of available spots may not be sufficient to provide the treatment with the required timeliness and quality.33 Subsequent studies could deepen these hypotheses, with the additional advantage that the period of inclusion of breast cancer in the FPGC would be higher.
In Mexico, there is a legal and regulatory framework for universal access to BC treatment; however, this framework needs to be translated into effective and timely access to a health services infrastructure and sufficient human resources to meet the demand of such services.14 However, increasing the available information about the benefits of using FPGC through awareness campaigns about the existing regulations to both health care providers and women would be advisable.
The nationwide breast cancer mortality rates in women aged 25 years or older presented here are similar to those reported in other studies.3,34,35) However, this study is one of the first that takes into account the insurance scheme, which gives an added value to generate an hypotheses about the differential impact of the inclusion of comprehensive BC treatment between FPGC populations with and without social security.
One limitation of this study is that it does not measure BC prevalence and incidence because the number of hospital discharges is different from the number of patients. Moreover, for some years (2005 and 2011), no reliable data at the national and federative state levels were available on the number of hospital discharges for BC per age group. To resolve this issue, some populations for which the number of hospital discharges for BC was not available were estimated; therefore, the results may not reflect actual trends for these years. This estimation is a limitation of this study because of the lack of population information disaggregated by age groups and the lack of access to original source data (i.e., medical records). Another limitation of the study is not upholding the correlations between mortality rates and some determinants of health inequalities because they were not part of the objectives of this study. However, this analysis attempts to establish the foundations to perform other studies in greater depth that could identify the factors that limit the effects of including comprehensive BC treatment in the FPGC.
In conclusion, the results of this study suggest that trends in mortality rates among women are heterogeneous according to insurance scheme and are higher for UW than for IW, who showed a decreasing trend. These findings could be a reflection of differences in socioeconomic status or could be because the coverage of mammography screening is higher among IW than among UW.7 This difference results in BC treatment beginning at an earlier stage for IW than for UW. Although the current FPGC operation has not yet shown the desired change in the health indicator, improvements in access, strengthening the mechanisms to recruit women to the SPSS, and ensuring the implementation of regulations and consolidating systems for training, evaluation, monitoring and compliance of operating regulations and treatment guides for BC systems is necessary. The adaptation of the established capacity to the demand for services is necessary, as is the development of a leadership capacity of health authorities to fulfill the roles of coordination and regulation. These changes would improve equity in access to BC treatment care and would inform on population-wide results.

