











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkTo understand the effect that cancer has had on children (0-14 years old), it is necessary to study both the incidence and the mortality from these causes. 1
The difficulty in estimating the incidence of cancer lies in the necessity of having a population-based registry of cancer cases, which means recording all cases that occur in a given population and, most importantly, collecting data with quality criteria (indicating that the data should be 1) complete, 2) valid, 3) timely, and 4) following international standards for the coding and comparison of information). 2 These criteria are necessary so that the data will be reliable. Moreover, a registry of a few well-recorded cases is preferred to a registry of many poorly-recorded cases. 3 Accordingly, the incidence of cancer in children in developed countries is well-known. 1
In reference to the study of cancer mortality in both developed and developing countries, there are well-established policies for building an adequate registry of cancer deaths. Therefore, cancer mortality in children is well-known in most countries worldwide. 4,5
The interpretation of the mentioned indicators is important because the incidence is related to the risk that a population has of developing a disease. 1,3 For its part, mortality is a fairly accurate reflection of the overall treatment being provided to children with cancer, particularly when the disease incidence is stable. 6,7
Globally, the overall incidence of cancer in children ranges between 100 and 180 cases per 1 000 000 children / year. Incidences below this range reflect a possible underestimation, and incidences above represent a possible overestimation. 8
In countries where the survival of patients has increased, the mortality has subsequently decreased; this situation has occurred in developed countries. Furthermore, the mortality rate ranges between 22 and 30 cases per 1 000 000 children / year in these countries. 4,7
At the Instituto Mexicano del Seguro Social (IMSS) [Mexican Social Security Institute (MSSI)], which is located in the Distrito Federal (DF) [Federal District, coterminous with Mexico City], a population-based Registry of Cancer in Children (RCC) was initiated in 1996 and has attempted to comply with the aforementioned quality criteria. The Registry contains information regarding the cancer epidemiology of MSSI beneficiary (MSSI-B) children, but only children in some states of the Mexican Republic have been included. 9
The objective of this study was to analyze the data for both cancer incidence and mortality in MSSI-B children who were residents of the DF, Estado de México (EM), Morelos (Mor), Guerrero (Gro), and Chiapas (Chis) for the period of 1996-2013 and to discern the tendency that each variable presented.
Materials and methods
An observational, prospective, descriptive study was conducted. Data from two population registries were analyzed for the period from January 1st, 1996 to December 31st, 2013.
Data were obtained from two different sources of information.
a Incidence data. The information for the study of incidence was obtained from the RCC, which is managed at the Clinical Epidemiology Medical Research Unit of the Pediatric Hospital in the National Medical Center XXI Century. It is a population-based registry of cancer cases. The information is collected actively and prospectively by two registrars (nurses) who were trained for the collection, coding (morphology, topography, and staging of cases), and data capture of the different study variables. The coding and staging of the cases are performed in conjunction with the head of the registry (AFG), with a good consistency in the coding of these variables (unweighted Kappa of 0.85).
To code the different cancer cases, topographic and morphologic codes are used. For cases collected from 1996-1999, the second edition of the International Classification of Diseases for Oncology (ICD-O-2) was used, and for cases collected between 2000 and 2013, the third edition (ICD-O-3) was used. The cases were grouped according to the International Classification for Childhood Cancer (ICCC). 10
This study used data on children with cancer who were treated in the DF at the two hospitals that the MSSI uses for the care of its beneficiaries [the Pediatric Hospital (PH) in the National Medical Center XXI Century and the General Hospital in the National Medical Center La Raza (LR)]. These hospitals contain the necessary infrastructure to establish the precise diagnosis of cancer in patients. These are the reference centers for children with cancer from other states in the Mexican republic. Only the data regarding cancer in children coming from the DF, EM, Mor, Gro, and Chis were included in the analysis because data on cancer cases in children from the mentioned states are sent to the DF for their treatment, and they have been registered there since 1996, the year the RCC was initiated. 11
The analyzed cases were carefully selected only once to avoid duplicate cases. In 97.5% of the lymphoma and solid tumor cases, the diagnosis was confirmed by means of histopathological study, and in 100% of the leukemia cases, the diagnosis was confirmed through bone marrow aspiration.
b Mortality Data. Mortality data were obtained from the Instituto Nacional de Estadística y Geografía (INEGI) [National Institute of Statistics and Geography]. 12 For the study period, two International Classifications of Diseases (ICD) were used for coding the causes of death (ICD-9 for 1990-1997 and ICD-10 for the period 1998-2013); therefore, the table of equivalences for the study of mortality data, in which the equivalence of the ICD-9 to ICD-10 codes is established, was used. The ICD-9 codes 140-240 and the ICD-10 codes C00-97 were used. 13
The selection criteria for the analysis of the incidence and mortality were as follows: a) children who were diagnosed with cancer of any ICCC group; 10 b) MSSI beneficiaries under the age of 15; and c) residents of the DF, EM, Mor, Gro, and Chis.
The denominators for calculating the incidence and mortality rates corresponded to the population under 15 years of age who were MSSI-B Ascribed to Family Medicine and residents of the selected states; the denominators were obtained from the Coordination of Medical Care of the MSSI. 14
The absolute frequencies of the different groups and subgroups of cancer were obtained, and the overall and specific incidence was estimated by group and subgroup of neoplasia cases according to the ICCC10 and was stratified by age, sex, and state of residence. Age was grouped into the following categories: less than 1 year, 1-4, 5-9, and 10-14 years (rates given for 1 000 000 children/year, unless otherwise specified). A rate adjustment was performed by the direct method for the total incidence and the incidence by subgroup. The reference population was the population worldwide. 15
Furthermore, the annual mortality rates were obtained overall and were stratified by state. To evaluate the trend in both incidence and mortality, the annual percentage of change and the average annual percentage of change during the study period were obtained (APC and AAPC, respectively). These indicators are a weighted average of the annual percentage of increase or decrease that occurs in a population within a short period (APC) or during the entire study period (AAPC). For this analysis, the Joinpoint Regression Analysis program (version 4.0) that provides the Surveillance, Epidemiology, and End Results Program of the United States of America was used, and a p≤0.05 was accepted as the limit of statistical significance.* The research protocol was approved by the Committee on Research and Ethics of the Helsinki Protocol.
Results
The overall incidence decreased for the period of 1996-2001 and then stabilized for the period of 2002-2013 [APC = -6.6% (95%CI -11.0, -1.9) and 0.6% (95%CI -0.6, 1.9), respectively]. The same trend occurred in EM and Chis. Both Mor and Gro displayed a decreasing trend for the entire period [AAPC = -2.3% (95%CI -4.1, -0.6) and -2.6% (95%CI -4.9, -0.2), respectively]. The DF displayed a stable trend throughout the period (table I, figure 1).
Table I Incidence* and mortality* trends according to the state of residence in the Mexican republic of beneficiary children of the MSSI. 1996-2013

* Rates adjusted by age for 1 000 000 children/year; ICCC: International Classification for Childhood Cancer (reference 10); APC: Annual percentage of change; AAPC: Average annual percentage change for the period
‡ The APC is significantly different from zero at an alpha of 0.05; CI95% = 95% confidence interval
§ Period 1996-2010
# Period 2010-2013
MSSI: Mexican Social Security Institute
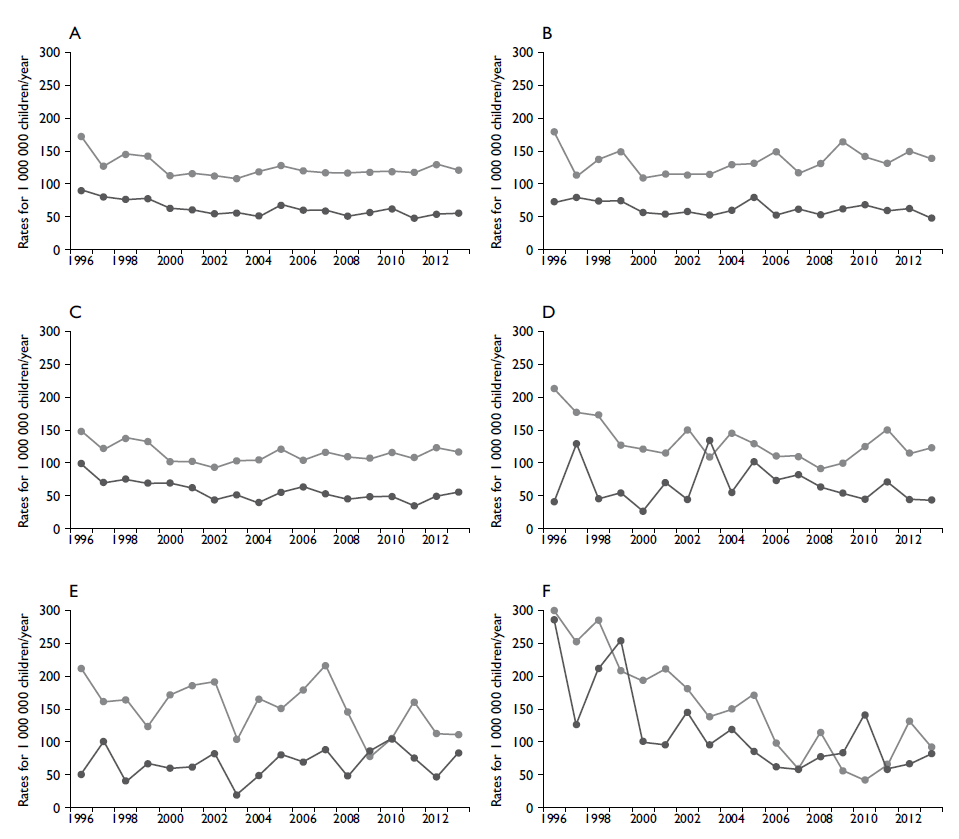
A. Overall, B. Distrito Federal, C. Estado de México, D. Morelos; E. Guerrero; F. Chiapas
Figure I Trend of cancer incidence and mortality in beneficiary children of the Mexican Social Security Institute who were residents of five states of the Mexican republic (1993-2013)
The same aforementioned phenomenon was found in the overall trend in mortality. There was a decreasing trend for the period of 1996-2002 (APC = -7.0% (95%CI -11.4, -2.4), but mortality remained stable for the following period (2003-2013). EM and Chis displayed a decreasing trend for the entire period [AAPC = -3.3% (95%CI -5.0, -1.5) and -6.2% (95%CI -9.3, -3.1), respectively]. The trends for the DF, Mor, and Gro were stable (table I, figure 1).
Because the trend in overall mortality was stable over the final 11 years (2003-2013), the average exact rate for that period, overall and for each state, was obtained. Overall, the mortality rate was 56.7, and for the DF, EM, Mor, Gro, and Chis, the mortality rate was 61.3, 49.1, 68.9, 68.4, and 85.0, respectively.
For incidence, the same phenomenon was observed in the neoplasia, general leukemia, and acute lymphoid groups. During the period of 1996-2001, there was a decreasing trend, and for the period of 2002-2013, the trend was stable [APC = -7.3% (-17.3, -2.7) and -6.1% (-11.1, -0.5), respectively]. With respect to other groups of neoplasias, myeloid leukemias, lymphomas in general, Hodgkin's lymphoma and non-Hodgkin's lymphoma (NHL) displayed a decreasing trend for the entire study period (table II).
Table II Incidence* trends according to groups and subgroups of the ICCC in beneficiary children of the MSSI who were residents of five states of the Mexican republic. 1996-2013
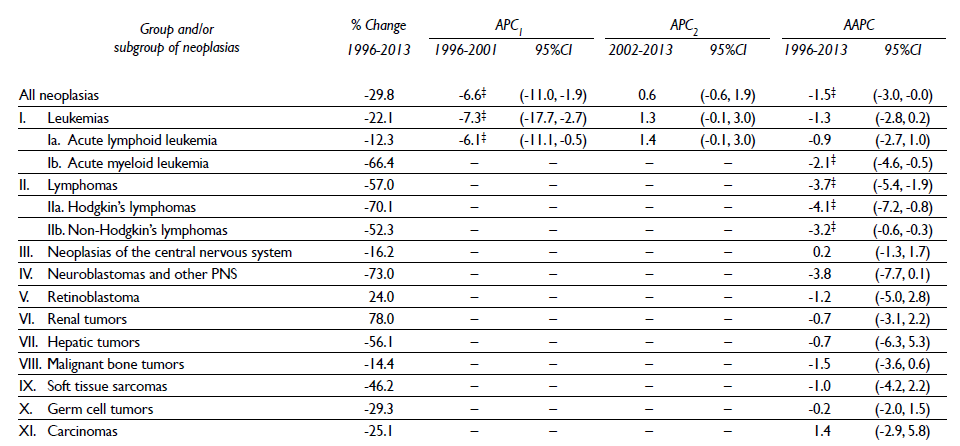
* Rates adjusted by age for 1 000 000 children/year; ICCC: International Classification for Childhood Cancer (reference 10); APC: Annual percentage of change; AAPC: Average annual percentage change for the period
‡ The APC is significantly different from zero at an alpha of 0.05; 95%CI= 95% confidence interval
MSSI: Mexican Social Security Institute
Moreover, the overall incidence was 128.0 cases per 1 000 000 children for all of the different groups of cancer. Leukemias, central nervous system tumors (CNST), and lymphomas were the main groups of neoplasias that were presented, and they displayed incidences of 58.8, 15.3, and 13.0, respectively (table III).
Table III Incidence* of malignant neoplasias in beneficiary children of the MSSI who were residents of five states of the Mexican republic ‡ , 1996-2013
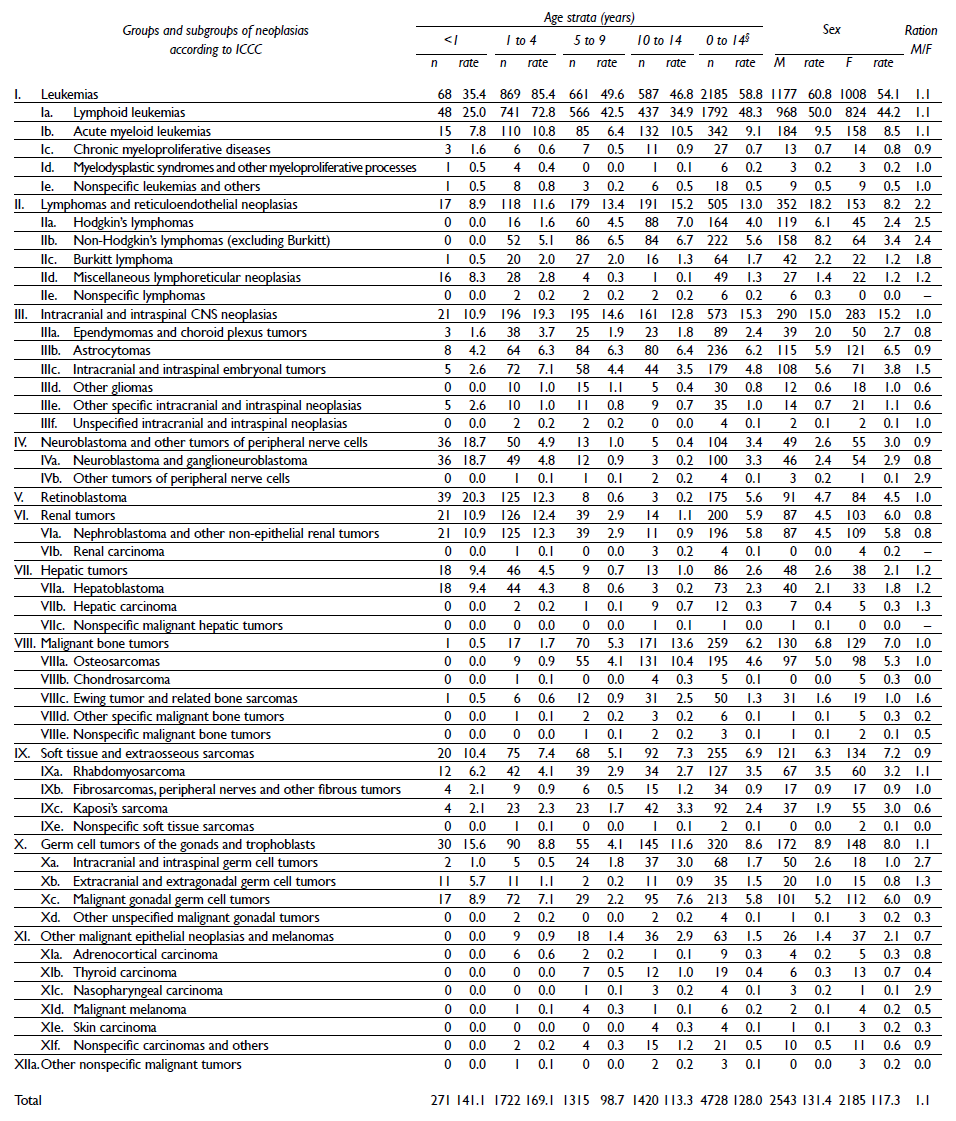
* Rates per 1 000 000 children/year
‡ Distrito Federal, Estado de México, Morelos, Guerrero, and Chiapas; MSSI = Mexican Social Security Institute; ICCC: International Classification for Childhood Cancer (reference 10)
§ Rates adjusted for age; n: number of cases; M: male; F: female; CNS: central nervous system
The highest incidence within the subgroups of leukemias occurred for acute lymphoid leukemia (48.3); of the CNSTs, astrocytomas occurred at the highest incidence (6.2), and NHL displayed the highest incidence in the lymphoma group (5.6) (table III).
In relation to other neoplasias, germ cell tumors (GCTs) were the 4th most common type, with an incidence of 8.6. The remainder of the neoplasias had lower incidences than those noted (table III).
The highest incidence according to age occurred in the 1-4-year-old age group, followed by infants less than 1 year old, children 10-14 years old, and finally children 5-9 years old, with rates of 169.1, 141.1, 113.3, and 98.7, respectively. The incidence according to sex was slightly higher in males (ratio M/F=1.1) (table III).
The highest incidence with respect to the state of residence occurred in Gro, followed by Chis, DF, Mor, and EM (rates of 155.1, 152.7, 137.8, 133.8, and 116.2, respectively). In general, the pattern of the main neoplasias was as follows: leukemias, CNST, and lymphomas, except in EM, wherein both lymphomas and CNSTs had a similar incidence (table IV).
Table IV Incidence* of malignant neoplasias in beneficiary children of the MSSI who were residents of five states of the Mexican republic. ‡ 1996-2013

* Rates are age adjusted per 1 000 000 children/year
‡ Distrito Federal, Estado de México, Morelos, Guerrero, and Chiapas; MSSI: Mexican Social Security Institute; ICCC: International Classification for Childhood Cancer (reference 10); n: number of cases; CNS: central nervous system
Discussion
One of the most important aspects identified in the present study is related to the data on the trends of both incidence and mortality. Having already reported the phenomenon, incidence displayed a decrease during the period of 1996-2001, 9 which was spontaneous and subsequently stabilized through 2013. We consider this trend to be a real effect and not the result of poor records in the RCC. The mortality data encountered also lends support to this phenomenon because the observed trend in incidence was also encountered in mortality, which was even presented with a year of delay because the decline occurred during 1996-2002 (table I, figure 1).
We do not know the causes of this phenomenon, but as noted when we first reported the decline, we believe that there was a period effect in the study population. That is, prior to 1996, the population of children may have been exposed to a harmful exposure, during which the incidence increased; subsequently, it was eliminated or the exposure was terminated; therefore, (spontaneously) the incidence and mortality decreased, as shown by the data from this study.
In support of this hypothesis, in a study conducted in Mexico, an increase in the mortality rate from 46.8 to 56.3 during the period of 1980-1995 was identified. 16 Moreover, in the evaluation of cancer mortality during 1970-2007 that was performed by L. Chatenoud and colleagues, in countries in America, Asia, and Oceania, an abrupt increase in the trend of mortality was observed in Mexico during the period of 1985-1990, which supports our comments. 7
Due to the absence of incidence data for periods preceding that recorded (1996-2013) and with the objective of identifying specific points and attempting to explain the phenomenon found, further exploration of the data on cancer mortality in Mexican children in greater detail should be considered.
Furthermore, relating exclusively to the incidence trend for the period of 2001-2013, the overall trend for all of the states and for the group of leukemias and the acute lymphoid subgroup was stable (tables I and II), which contrasts with that reported in developed countries (the United States of America and European countries), where it has been noted that cancer in children and, above all acute lymphoblastic leukemia, has increased. 13,17 There is controversy in relation to myeloid leukemias. North American children displayed an increasing trend during the period of 1975-1993 and stability during the period of 1994-2012; 13 in contrast, for European children, the trend has remained stable. 18 Our data showed a decreasing trend for myeloid leukemias throughout the study period (table II).
The trend of lymphomas occurred similarly in North American children compared to the previously discussed phenomenon. The trend decreased for the period of 1975-1993, but the period of 1994-2012 displayed an increasing trend. 13 In European children, there was an increasing trend in general, but this only occurred in the southern and western regions of Europe. 19 Data from our study showed a decreasing trend, and in a more detailed study of lymphomas that was performed by our group, the mixed cellularity subtype decreased in Hodgkin's lymphomas; non-Hodgkin's lymphomas also displayed a decreasing trend, particularly in the unspecified types, which was identified as an improvement in the histopathological diagnosis in recent years. 20
In relation to mortality exclusively, which, as mentioned, is related to the overall efficacy of treatment that is being administered to the population, 6,21 only the data from the period of 2003-2013 should be considered because during this period, the incidence was stable and it could be verified that the incidence differed from what occurred in developed countries, where the cancer mortality in children decreased. 4,7,13,22 This did not occur for the children in our study and in general for Mexican children because similar results were found when cancer mortality for children throughout the country was studied. 7,23
Furthermore, the exact mortality rate for some developed countries is between 22 and 30 deaths per 1 000 000 children, 7,13 whereas in our data, it corresponded to 49.3 and 85 (mortality rates for EM and Chiapas, respectively). This situation has been mentioned even by foreign authors. 7,24 Thus, the treatment of children with cancer in our country requires a better organization of the health system in charge of offering medical care for Mexican children with cancer, and we believe that research is the key through comprehensive studies and through research in conjunction with international organizations. 1
With regard to the incidence of the different groups and subgroups of cancer, the data obtained in the present study are consistent with what has previously been reported in MSSI-B children. 25
In relation to GCT only, it is noteworthy that the incidence found (8.6) is one of the highest worldwide; only children of Gro had a lower incidence (5.6), which was similar to that of North American and German children (5.5 and 4.9, respectively). 13,26 Therefore, we believe that the epidemiology of this group of cancers should be studied in detail worldwide to establish possible etiological hypotheses.
Nationally, some data on the epidemiology of children with cancer who were treated using the strategy of the Seguro Popular [People's Insurance] have been published. We could not compare our data with the data of that group because the populations were different. Seguro Popular reported on children 0 to 18 years of age, whereas the present study reported on children 0 to 14 years of age. Notably, the ICCC was used to group the different cancer groups, but the groups of neoplasias that were presented are different from that classification, and the data on the incidence according to age were not calculated according to traditional methods. 27
Conclusions
The incidence and mortality rates from cancer in the study population displayed spontaneous declines for the period of 1996-2001 and 1996-2002, respectively. For the additional period (2002-2013; 2003-2013), the trend for both indicators remained stable. According to the mortality data, the efficacy of the treatment that was offered to the children studied was not as effective as that attained by children in developed countries, indicating the need to conduct research, interinstitutional and/or international, to identify the causes of the treatment efficacy and to improve the treatment. The incidence data according to the neoplasm group, age, sex, and place of residence are consistent with those reported previously.

