











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkCancer is one of the leading causes of death worldwide; 8.2 million of the deaths that occurred during 2012 were attributed to cancer and included 4.66 million men and 3.54 million women. The main types of cancer are lung (1.59 million deaths), liver (740 373 deaths), stomach (733 499 deaths), colorectal (723 913 deaths), breast (536 521 deaths), and esophageal cancer (405 s803 deaths). More than 60% of all new cases that arise annually in the world occur in Africa, Asia, and Central and South America. These regions represent 70% of all cancer deaths in the world, and it is expected that the number of annual cases will increase from 14 million in 2012 to 22 million in the next two decades.1,2
In recent decades, there has been a historic change in the evolution of the health status of the population, with a decrease in mortality in older age groups.3 Several factors have contributed to this situation, such as the control of most communicable diseases, extension of preventive and therapeutic interventions to large population sectors, progressive increase in life expectancy (LE), and the consequent aging of the population.4,5
In Mexico, according to the Union for International Cancer Control (UICC), cancer is the third leading cause of death, and an estimated 128 000 new cases are detected each year (Health Secretariat, Sub-secretariat for Prevention and Health Promotion [Subsecretaría de Prevención y Promoción de la Salud, SPPS]).6
If the projections made by the National Institute of Statistics and Geography (Instituto Nacional de Estadística y Geografía, INEGI) are met, the life expectancy at birth of the Mexican population will be 75.7 and 77.0 by the years 2020 and 2030, respectively,7 which may increase the absolute number of people who develop a malignant tumor. Despite therapeutic advances, cancer survival does not guarantee that the patients who suffer from it will have good quality of life because various disabilities can occur depending on the type of cancer.8,9 The Disability-Adjusted Life Years (DALYs) is a summary measure that takes into account the frequency and age of death and the aftermath of the disease to determine a better estimate of the burden of disease.
This study describes the burden of cancers in the population of affiliates of the Mexican Social Security Institute (Instituto Mexicano del Seguro Social, IMSS).
Materials and methods
Calculation of the DALYs was performed following the methodological principles outlined in the National Burden of Disease Studies: A Practical Guide for each of the 35 delegations into which the institution divides the country.10
The DALYs is the sum of years of life lost (YLL) due to premature mortality and years lived with disability (YLD). In this calculation, the criteria established by the Global Burden of Disease Study (GBD Study), i.e., the social value of time lived to different ages and a discount rate of 3%, were applied.
The steps for calculating the DALYs can be summarized as follows: estimation of overall mortality by age, sex, and life expectancy; selection of the list of diseases; estimation of age-sex specific deaths and correction of misclassification of deaths; choice of the information source and the parameters that best describe the disability caused by the studied diseases; modeling the diseases using the DISMOD program; and calculation of the YLL, YLD, and DALYs.
Estimation of overall age-sex mortality and life expectancy
The life expectancy by delegation and overall mortality were calculated using information on deaths among affiliates registered in the INEGI database11 and the Population Assigned to Units,12 distributed by age and sex groups, according to the INEGI Population Census.13 The sources cited consider information from 2010. The IMSS divides the states of Mexico, Veracruz, and the Federal District into two delegations each; this geographical division is not included in the INEGI mortality database; therefore, it was necessary to consider the deaths per municipality classified according to the area covered by each delegation.
Selection of the disease list
Malignant neoplasms that correspond to the GBD IIA group were divided into subgroups including IIA1-IIA2, diseases corresponding to mouth, nasopharyngeal and oropharyngeal cancers (10th ICD revision, C00-C14); IIA3, cancer of the esophagus (C15); IIA4, stomach cancer (C16); IIA5, colorectal cancer (C18-C21); IIA6, liver cancer (C22); IIA7, cancer of the gallbladder and biliary tract (C23-C24); IIA8, pancreatic tumors (C25); IIA9, cancer of the larynx (C32); IIA10, cancer of the trachea, bronchia, and lungs (C33-C34); IIA11-IIA12, malignant melanoma and other skin tumors (C43-C44); IIA13, malignant breast tumors (C50); IIA14, cancer of the cervix (C53); IIA15, cancer of the uterus (C54); IIA16, cancer of the ovaries (C56); IIA17, cancer of the prostate (C61); IIA19, malignant tumors of the kidney and other urinary organs (C64-C66, C68); IIA20, malignant bladder tumors (C67); IIA21, cancer of the brain and nervous system (C70-C72); IIA24 and IIA23, Hodgkin and non-Hodgkin lymphomas (C81-C85, C96); IIA25, multiple myeloma (C88-C90); IIA26, leukemia (C91-C95); and IIA18, IIA27, and IIA22, consisting of other malignant neoplasms (C17, C30-C31, C37-C38, C40-C41, C45-C49, C51-C52, C57- C60, C62, except C63 C63.9, C69, C73, C74-C75, C77-C79, C97, C26, and C39).
Estimation of age and sex-specific deaths and correction for misclassification of deaths
The underreporting of deaths was corrected by delegation, age, and sex groups. Infant mortality was adjusted according to the estimations performed by Aguirre,14 who used the method of Brass, while in the group of subjects over four years old, the generalized method was used in combination with an analysis of the consistency of the deaths reported in the IMSS Mortality System (SISMOR) and by the INEGI. Both methods are validated, and their use is recommended in the GBD Study.10 The corrected death values were redistributed by delegation, cause, age, and sex to calculate the YLL and also used as one of the input parameters for DISMOD II* to model all subgroups of malignant neoplasms and estimate the incidence, age of onset, and duration of the disease, which combined with the weight of disability, are the basis for calculating the YLD.
Choosing the information source and parameters that best describe the disability caused by the diseases studied
In addition, mortality, incidence (first-time visits to IMSS specialty units), and prevalence (data from the National Cancer Registry for the Hispanic population in the United States) were selected as input parameters for the model. For malignant breast tumors (IIA13) and other malignant neoplasms (IIA18, IIA22, and IIA27) remission according to the criteria of a group of clinical experts from the Institute was used, and in the case of IIA13 only, new cases reported by the Unified Automated System for Epidemiological Surveillance (Sistema Único Automatizado para la Vigilancia Epidemiológica, SUAVE) were used to calculate the incidence. All parameters used for modeling in DISMOD were disaggregated by delegation, age, and sex.
Modeling the diseases using the DISMOD program
The disease duration and incidence in all subgroups were estimated; therefore, they were consistent with the natural history of the disease and the particularities of each delegation in terms of risk factors, lifestyles, and environmental and socioeconomic conditions.
A factor of 0.484 was used for weighting of disability15 for cancers of the mouth, nasopharynx, and oropharynx; esophagus; liver; gall bladder and biliary tract; pancreas; larynx; trachea, bronchia, and lung; ovary; kidney and other urinary organs; bladder; and brain and nervous system. This weighting assumes that disability caused by these cancers limits the patient's ability to perform activities in two or more of the following areas: recreation, education, procreation, and occupation.16
For malignant stomach, colon, rectal, breast, cervical, and uterine cancers; Hodgkin's and non-Hodgkin lymphoma; multiple myeloma; leukemia; and other malignant neoplasms, the weighting factor was 0.294. This value considers limitations in the ability to perform most activities in one of the following areas: recreation, education, procreation, and occupation.
Calculation of the YLL due to premature mortality, YLD, and DALYs
The YLL, YLD, and DALYs were calculated by age and sex for each delegation for each of the diseases studied using the previously described procedures and with the support of tools developed by the WHO. The YLL values were calculated from the table of standard Western life as recommended in the National Burden of Disease Studies: A Practical Guide.10
Results
In 2010, cancer was the fifth leading cause of disease burden in the IMSS affiliate population, with a total of 736 090 DALYs and a rate of 16 722 DALYs per 1000 affiliates (figure 1). Of these, two-thirds were due to the YLL resulting from premature death, and one-third of the YLL were associated with disability.

Figure I Fifteen major causes of disease burden measured via Disability-Adjusted Life Years (DALYs). Mexico, IMSS 2010
In figure 2, the distributions of the YLL and YLD are shown for each cancer. Breast cancer was the malignant neoplasia that showed the highest contribution to the disease burden, followed by prostate cancer. In both, the weight of disability was greater than 50%. In contrast, for cancers of the trachea, bronchia, lung, stomach, liver, and pancreas; leukemia; and melanoma, the contribution of premature mortality was higher than 90%.

The burden of disease for each type of cancer differs by sex. With the exception of gallbladder and biliary tract cancer, in which the DALY rate per 1000 affiliates in women is almost twice that in men, and pancreatic cancer, in which there is no difference according to sex, the DALY rate is higher in men. This is especially the case for cancers of the larynx; esophagus; bladder; trachea; bronchia and lung; and mouth, nasopharynx, and oropharynx (table I).
Cuadro 1 Years of life lost due to premature mortality (YLL), Years lived with disability (YLD), and Disability adjusted life years (DALY ), for different types of cancer in women, men and total. Mexico, IMSS 2010

* Per 1000 affiliates
The contribution to the cancer burden by delegation is shown in figures 3 to 5. On average, 75% of the cancer burden in each delegation is due to ten cancers, including breast, prostate, tracheal, bronchial, and lung cancers, leukemia, and colorectal cancer, which rank in the top positions in terms of importance, not considering the subgroups of other malignant neoplasms.

DALY's: Disability-Adjusted Life Years
Figure 3 Distribution of cancer measured by DALYs, according to Delegation. Mexico, IMSS 2010

Figure 4 Distribution of cancer burden measured by Years of Life Lost due to Premature Mortality (YLL), according to Delegation. Mexico, IMSS 2010
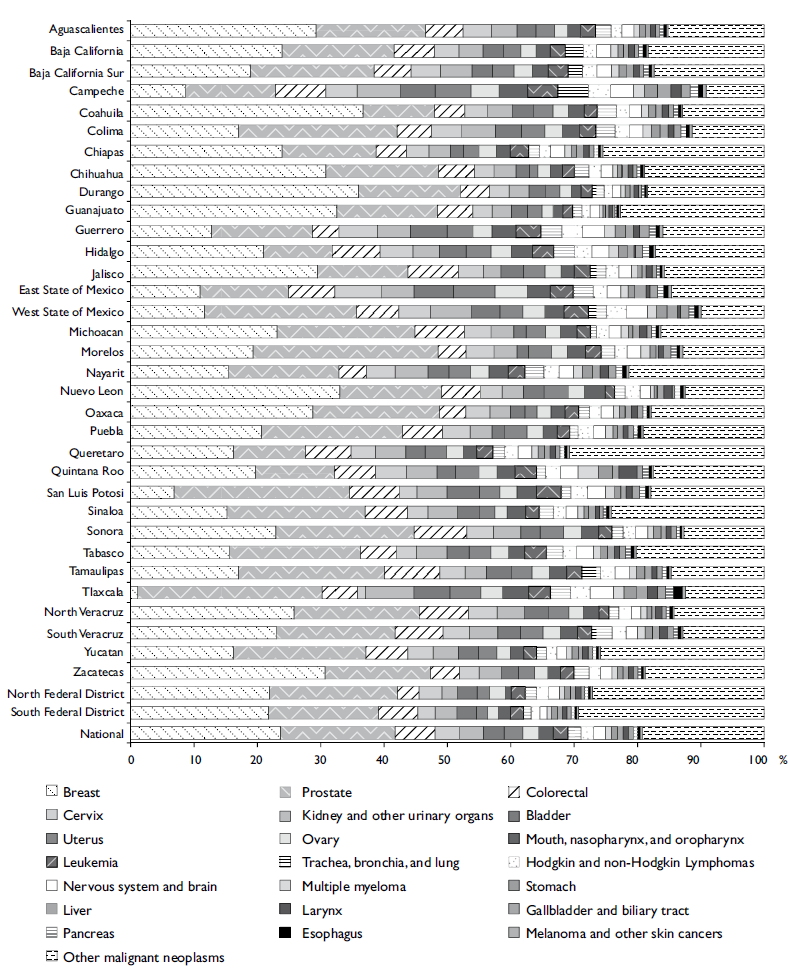
Figure 5 Distribution of cancer burden measured by Years Lived with Disability (YLD), according to Delegation. Mexico, IMSS 2010
It is worth noting that while breast cancer ranks first in importance nationally among IMSS affiliates, in some delegations, breast cancer occupies the second position in terms of incidence. In other delegations, it ranks in third (Tlaxcala), fourth (San Luis Potosi and Yucatan), or fifth (Campeche) place. In Chiapas, unlike the other delegations, cervical cancer ranks second, followed by leukemia. In eight delegations, cancer of the trachea, bronchia, and lung ranks second, while leukemia occupies the same position in six delegations.
Discussion
The total DALYs lost due to malignant neoplasms in the insured population corresponds to 6.8% of the total number of causes, which is below the value reported in the Global Burden of Disease Study 2010 (7.6%).17 In this latest study, the cancers that most contributed to the burden of disease were stomach cancer, other malignant neoplasms of the liver, and cancers of the trachea, bronchia, and lung; in the insured population of the IMSS, the diseases included breast cancer, other malignant neoplasms of the prostate, and cancers of the trachea, bronchia, and lung. This results can be explained by the use of different methodologies for calculating the DALYs.
Of the cancers, the diseases with the highest number of DALYs were breast and prostate cancers. In addition, these two diseases accounted for the largest proportion of years of disability, similar to that for noncommunicable diseases such as diabetes mellitus and cardiovascular and circulatory diseases. The order of the proportion of DALYs at the national level was very similar to the order within the IMSS delegations; for example, breast cancer ranked first in most IMSS delegations (82%).
In San Luis Potosí and Yucatán, prostate cancer ranks first, and leukemia ranks first in Campeche and Quintana Roo. Stomach cancer and cancer of the trachea, bronchia, and lung rank first in the delegations of Tlaxcala and Sinaloa, respectively. However, these conditions are in the second and fourth positions in other delegations. This uniformity in ranking likely occurs because IMSS affiliates are composed of individuals with a homogeneous socioeconomic status throughout the country.
Excluding breast and prostate cancer, in other conditions, the YLD proportion is very low, which indicates that these conditions are very lethal. The total YLL has no single explanation, as there are conditions such as leukemia in which the incidence rate does not occupy the first positions in the general population, but it occurs at younger ages. In contrast, tumors of the respiratory tract and stomach, which are among the leading causes of death in the general population and for which the lethality is very high, can be explained because most cases occur when individuals reach their 50s.18
Similar results were observed when comparing these results with those of other Latin American countries. In Peru, in 2008, cancers represented the fourth leading cause of disease burden (8% of the total DALYs) and a DALYs rate of 15.8 per thousand inhabitants, which was surpassed by mental and behavioral disorders, unintentional injuries, and cardiovascular diseases. Cancers of the stomach, blood system (leukemia), cervix, and breast, exhibited the greatest burden of disease.19
In Santander, Colombia, in 2005, the cancers with the highest burden of disease due to premature mortality were stomach cancer, leukemia, colorectal cancer, lung cancer, lymphoma and myeloma, and breast cancer.20 In both studies, the methodology used was similar to that used in our analysis, and although differences in the positions held by each cancer and in the percentage of burden attributable to premature death were observed, these differences could be due to the varying disability weightings used in each study.
The results of recent studies published on the disease burden of the country highlight the significance of some cancers21 ranked in the top 20 of all major causes analyzed (lung cancer in men and breast cancer in women, ranked in positions 19 and 10, respectively), specifically in terms of premature mortality. Taking into account these data, both cancers are the most significant contributors to the burden of disease attributable to premature mortality in the subgroup of malignant neoplasms, which is similar to the results of our study in which cancers of the breast and the trachea, bronchia, and lung were the first and second causes of YLL, respectively. Moreover, the significance of breast cancer, which has displaced cervical cancer in women,22 is highlighted.
One of the limitations of studies of disease burden is related to the availability and quality of information. Due to the lack of a cancer registry in institutions or in the country, information from various sources was used for our analysis including information from institutional (incidence), national (mortality), and international (prevalence) sources and a consensus of experts (remission), which allowed the calculation of accurate estimations that are comparable with the results of other studies.
The methodology used in this study corresponds to that published in 2001,10 which was made available to countries and institutions interested in using it, along with tools such as the DISMOD II. The evolution of the burden of disease during the study led to the development of newer applications that mainly employed computational and statistical methods to estimate parameters other than those estimated by the above methodology. These new tools inevitably produced different estimations.17
The results obtained in this study allow the identification of intervention priorities with regard to cancer at the institutional level and allow for the focus at the delegation level to be placed on cancers ranking higher in terms of disease burden. In this regard, the Institute has designed a cancer plan (OncoIMSS) that proposes including prostate and colorectal cancers in screening and early diagnosis programs. The OncoIMSS also considers the implementation of a population-based Institutional cancer registry, which will allow an assessment of the impact of these intervention programs.

