











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkLatin America and the Caribbean (LAC), representing 31 nations, 600 million inhabitants and towards 10% of the world's population, is a transitioning region with the highest overall Human Development Index (HDI) rating, yet marked inequalities persist between and within its constituent countries.1 In the last decades, the region has experienced significant reductions in fertility and infant mortality, with increases in life expectancy and subsequent aging of the population.2,3 Among developing regions, LAC has among the highest life expectancies, shaping the current epidemiological profiles. With the emergence of non-communicable diseases including cancer as the leading public health problem within the region, there remains great challenges to health care systems in LAC in forming a response to the increasing cancer burden and the care for patients, often with advanced cancer.4
This paper provides a situation analysis of the patterns and trends in cancer incidence and mortality by country in the sub-regions of South America, Central America and the Caribbean, and quantifies the future cancer incidence by 2030. We point to the data as an evidence basis for ongoing efforts to reduce the burden and suffering from cancer in LAC. Progress will require investment and reconfiguration of health systems, and in the tailoring of national strategies of cancer control to fit the cancer profiles within each country and the level of resources available.
Materials and methods
In this paper we provide a broad overview of the patterns and, where possible, trends in 31 countries within the LAC region, breaking down the situation analysis into three sub-regions of: South America (Argentina, Bolivia (Plurinational State of), Brazil, Chile, Colombia, Ecuador, French Guiana, Guyana, Paraguay, Peru, Suriname, Uruguay and Venezuela (Bolivarian Republic of)), Central America (Belize, Costa Rica, El Salvador, Honduras, Guatemala, Mexico, Nicaragua and Panama) and the Caribbean (Bahamas, Barbados, Cuba, Dominican Republic, Guadeloupe, Martinique, Haiti, Jamaica, Puerto Rico and Trinidad and Tobago). Data on cancer incidence and mortality rates for the year 2012 for each country were obtained from the GLOBOCAN database held at the International Agency for Research on Cancer (IARC) for the year 2012.5 These estimates were prepared using methods that are described in detail elsewhere,6 and they depend upon the availability and accuracy of the incidence and mortality data for each individual country. Observed incidence data from regional population-based cancer registries in three countries (Brazil, Colombia, Ecuador) together with national data for Costa Rica were obtained from the Cancer Incidence in Five Continents (CI5) series,* with data supplemented with more recently published data, where available. The WHO Mortality Database7 was used to provide corresponding mortality trend analyses for seven countries with long-term data series available from national civil registration systems: Argentina, Brazil, Chile, Colombia, Cuba, Ecuador and Mexico.
To adjust for the effects of age in comparative analyses of incidence and mortality rates by country and over time, we utilise two measures of direct standardisation, the age-standardised rate (ASR) using the world standard population, and the cumulative risk (up to the age of 74), defined as the lifetime risk of developing or dying from cancer in the absence of competing causes of death. In presenting the time trends of incidence and mortality ASR, random fluctuations were smoothed by country, sex and cancer site using loess regression. As well as all-sites combined excluding non-skin melanoma (ICD-10 C00-97, except C44), we focus on the six most frequent forms of cancer incidence and mortality within LAC: stomach (C16), colon and rectum (including anus C18-21) lung (including trachea, C33-34), female breast (C50), cervix uteri (C53) prostate (C61).
In assessing the cancer-specific trends we focussed on the temporal patterns of incidence and/or mortality from 1974-2012, where instructive in elucidating the needs and impact of cancer control: for breast and prostate, we examined both indicators; for stomach, colorectal and lung, we examined mortality trends. For cervical cancer, we assessed incidence, in part given the problems of misclassification of corpus uterus, part unspecified, in the mortality data. Finally, we predict the all-cancer incidence in both sexes by sub-region by the future incidence based on country, sex- and age-specific incidence rates in 2012 applying to UN population projections for the year 2030.
Results
Overall cancer burden in the LAC Region
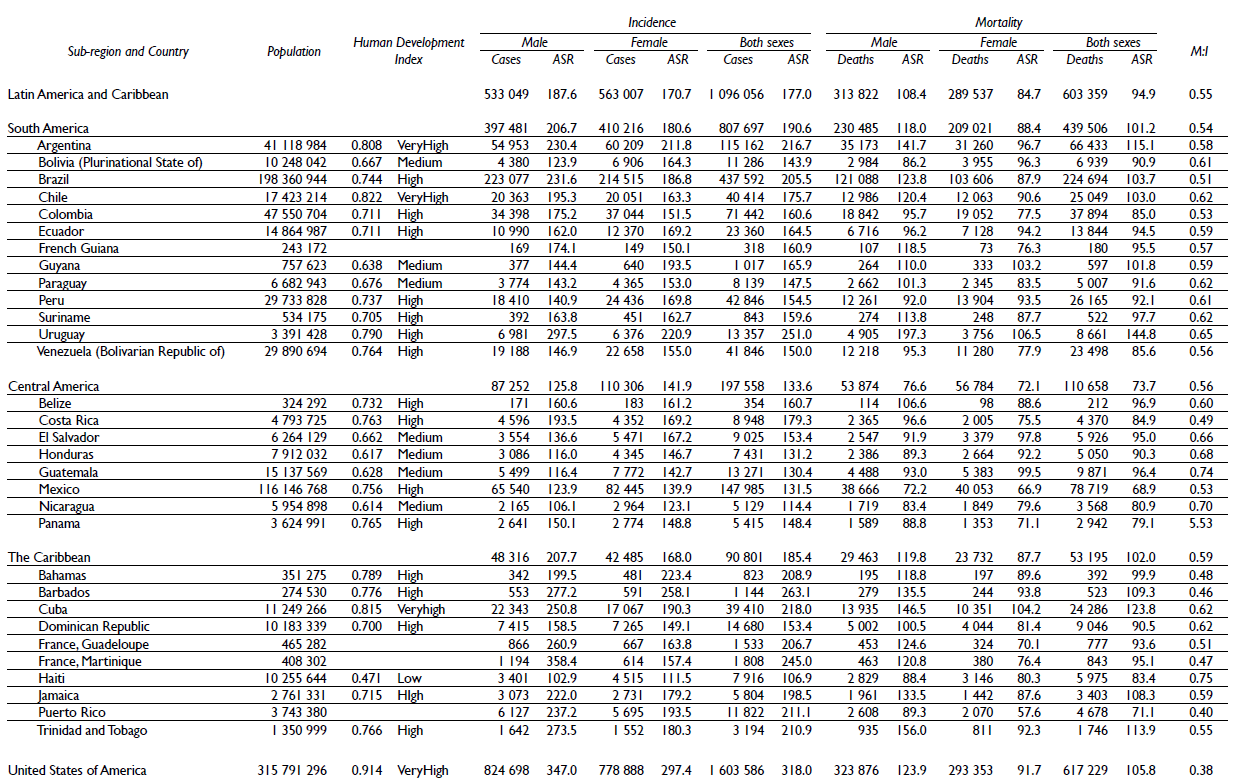
In 2012, almost 1.1 million new cancer cases were estimated to occur annually in the LAC region, accounting for 7.8% of cancer cases worldwide. Three-quarters of new cases in the region are seen in South America, the sub-region that also forms the majority population in the region (almost 67% of the total). Across countries, rates for both sexes vary 2.5 fold, with incidence highest in Uruguay, Barbados and Martinique and lowest in Haiti (table I). The total number of cancer deaths in 2012 was estimated at around 600000 in LAC. The highest mortality rates are seen in Uruguay, where cumulative risk of death (up to age 74) is 20% among men. Rates are lowest in Mexico and Puerto Rico, with, as a comparison, a corresponding cumulative mortality of cancer among women in the latter country of 6%. Overall cancer incidence and mortality rates are lower in Central America relative to South America and the Caribbean. Yet Nicaragua and Guatemala together with Haiti, have among the highest case fatalities in the region, as indicated through the elevated M:I ratios of 0.70, 0.74 and 0.75, respectively; these compare with a ratio of 0.38 in the U.S. (table I).
Sex-specific differences
In the region as a whole, sex-specific all-cancer incidence rates were similar (table I). Rates were consistently higher among males in all countries of the Caribbean (with the exception of Barbados and Haiti), while incidence rates among men in Martinique were more than double those of women. Conversely, incidence rates in Central America were consistently higher among females, other than for Belize and Panama. In terms of the mortality, rates tended to be greater in males in most countries, although there were exceptions in Bolivia, El Salvador and Guatemala, where female rates were greater (table I).
Patterns and trends in the most common cancers
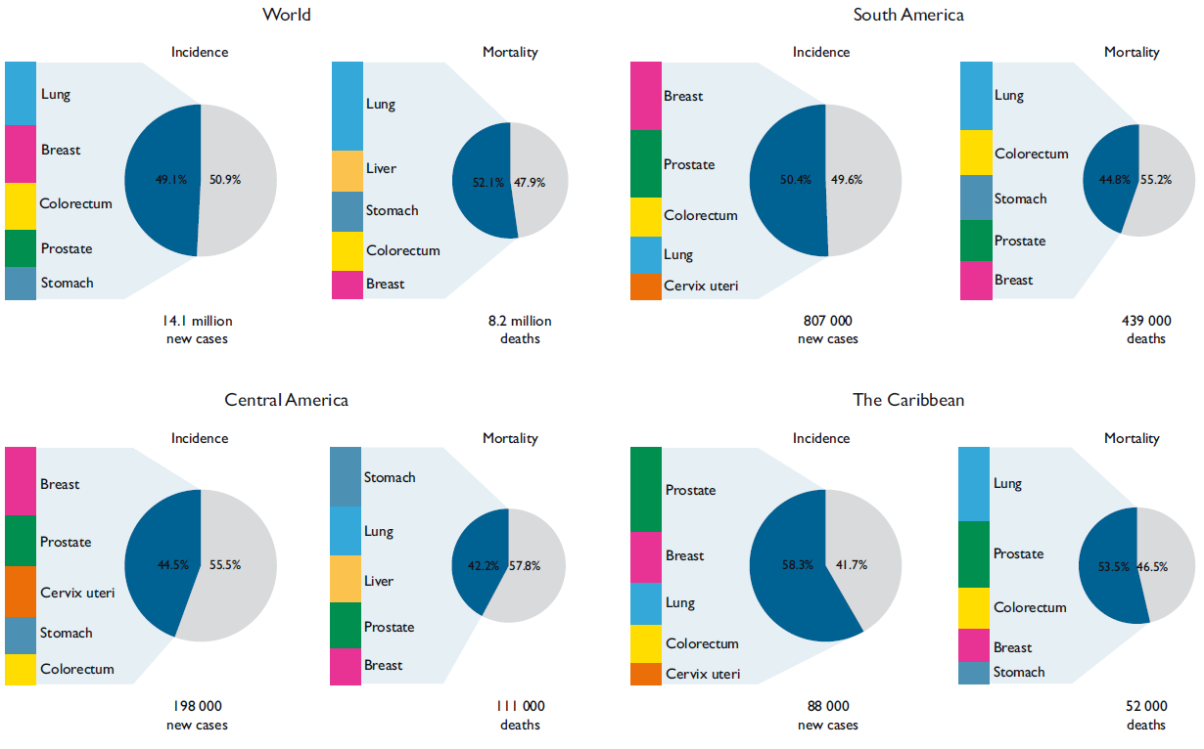
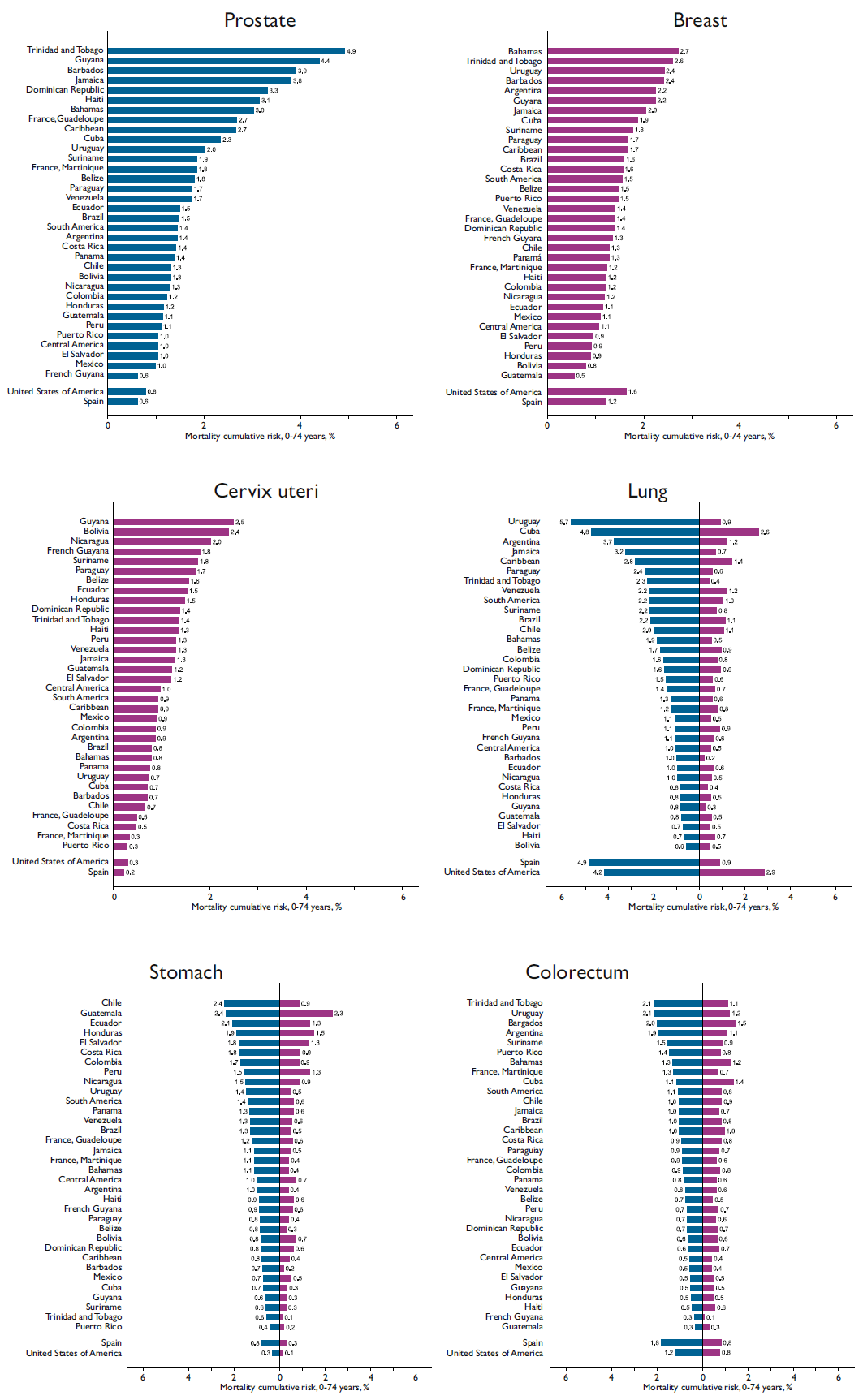
Figure 1 displays the five most frequent cancers (for incidence and mortality) in both sexes worldwide and in the three LAC sub-regions. These neoplasms account for 58, 50 and 45% all of incident cancers in the Caribbean, South America and Central America, respectively. In accordance with the global profile, the most common types in both South America and the Caribbean include cancers of the breast, prostate, colorectum and lung, with the latter neoplasm the leading cause of cancer death (figure 2). Males in Uruguay and Cuba had the highest risk of dying from lung cancer before the age of 75 in the region (5.7 and 4.8% respectively), higher or equivalent to the risk observed in Spanish and U.S. males (figure 3). In women, the cumulative risk of lung cancer only exceeds 1% in a handful of countries, but is by far highest in Cuba, where the risk of 2.6% is approaching risk among Spanish women.
Source: Global 2012
Figure I The five most frequent cancers in the world and the LAC sub-regions: incidence and mortality, both sexes
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement
Data source: GLOBOCAN 2012
Map production: IARC
World Health Organization
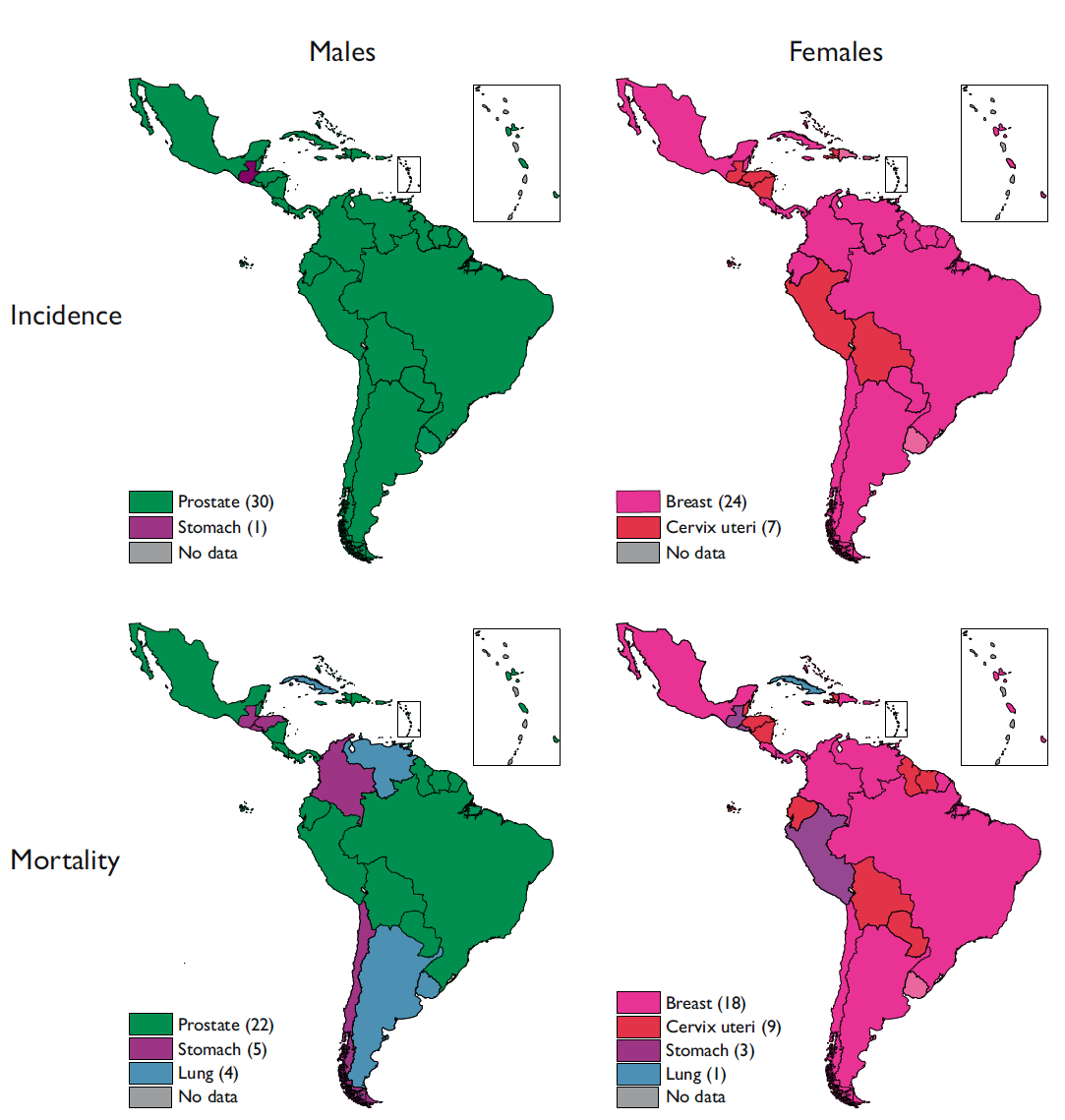
Figure 2 Leading causes of cancer incidence and mortality among males and females by country, LAC region
Source: reference 7
Figure 3 Cumulative risk of mortality for six common cancers by country and sex, LAC region
Trends in lung cancer convey very different temporal patterns in men and women (figures 4a and 4b). Mortality rates in men largely reveal decreasing trends, rates having peaked in most countries in the 1990s, with rapid declines in Argentina, Chile, Mexico and Costa Rica mirroring those in U.S. males, while rates in Cuban males are the one exception, where the rising rates have now surpassed rates among U.S men. In women, the lung cancer mortality rates are rising in most countries, excluding Mexico and Costa Rica, where declines are similar to those in men, or stable or recently declining in Colombia and Chile. The surge in rates among Cuban women mimic those in Spanish women, with the exception that rates in Cuba began to rise 10 years later and at level consistently three-fold higher relative to Spain.
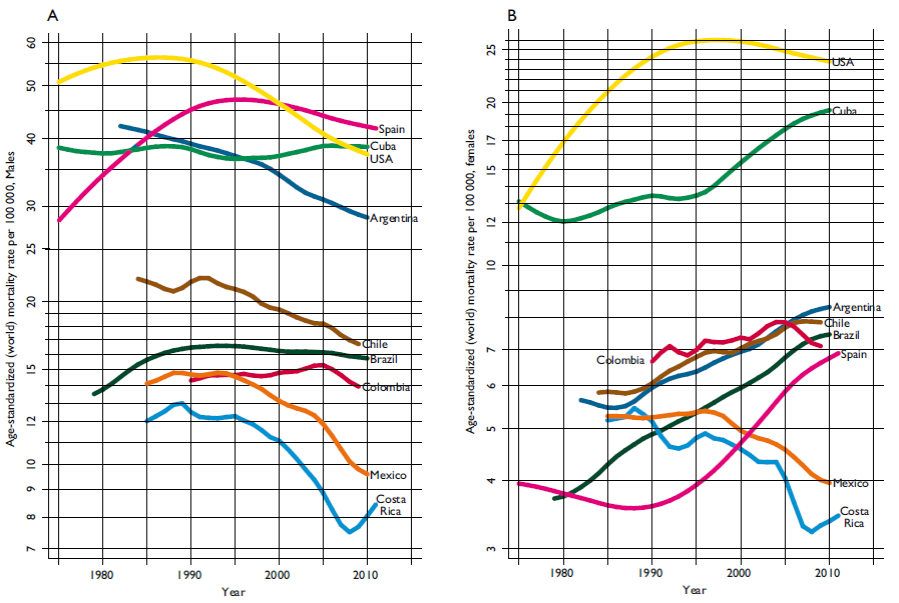
Source: reference 7
Figure 4 Trends in lung cancer mortality rates, males (4 A ) and females (4 B ) (ASR per 100 000)
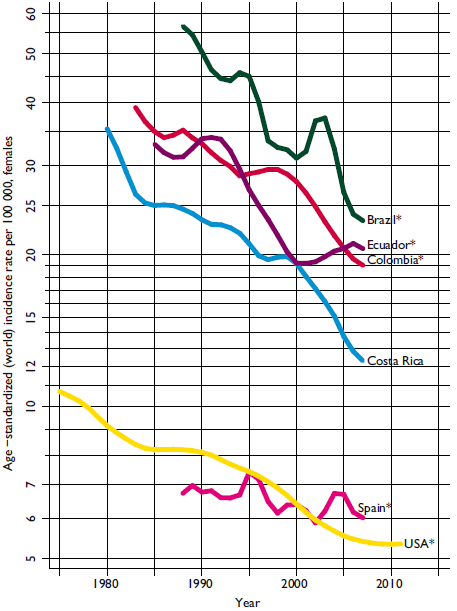
Breast cancer is the leading cause of cancer incidence and mortality in women in the majority of countries in the region, but cervical cancer is more common in a number of South and Central American countries including Bolivia and Nicaragua, the two countries with the highest mortality rates in the region. In terms of breast cancer, the highest risk of mortality from the disease is observed in several Caribbean countries as well as Uruguay and Argentina, where cumulative risk of death exceeds that seen among U.S. females (figure 3). Breast cancer incidence has risen 50% in two decades where there is national, or more commonly, regional registry data available (figure 5a). Incidence rates in Costa Rica and Ecuador are still half those observed among U.S. women however, despite rapidly increasing rates, while breast cancer incidence in Brazil appears to have peaked and recently declined. The magnitude and direction of breast cancer mortality trends are quite variable (figure 5b). In Argentina and Chile, declines are evident and similar, but less rapid than those observed in Spain and the U.S. Breast cancer mortality trends have become stable recently in Mexico and Colombia, but are rising in Brazil and Cuba, the latter country exceeding breast cancer mortality in the U.S.
* Regional registries
Source: IARC-CI5 Series; WHO Cancer Mortality Catabase
Figure 5 Trends in female breast cancer incidence (5 A ) and mortality rates (5 B ) (ASR per 100 000)
Among males, prostate cancer is the most frequently diagnosed cancer in all countries with the exception of Guatemala, where stomach is most common; prostate cancer is also the most common cause of death in the majority of countries (figure 2). Elevated cumulative risks of prostate cancer death were mainly observed in countries in the Caribbean, and in the countries of Trinidad and Tobago, Guyana and Barbados, risk of death is four times higher than seen in the U.S. (figure 3). Looking at the temporal patterns, incidence rates have rapidly risen to similar levels in Costa Rica, Ecuador and Colombia, similar to those in Spain, while a five-fold increase in incidence is observed in Brazil between the early-1990s and the mid-2000s (figure 6a). Mortality rates are much lower but convey considerable temporal heterogeneity: rates have been declining in the last one to two decades in Chile, Argentina, Costa Rica and Mexico, but are rapidly increasing in Brazil and Cuba, although rates in the latter country are double those of the former (figure 6b).
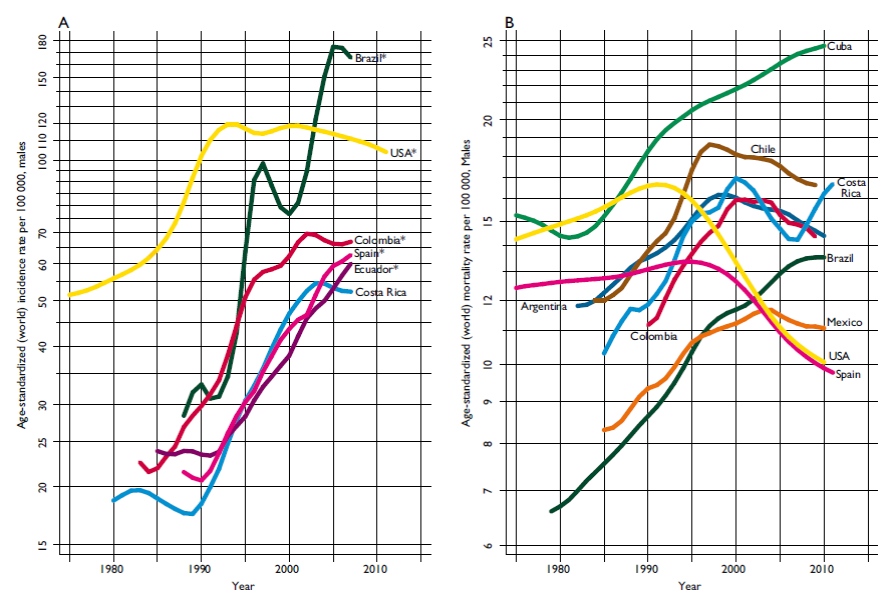
* Regional registries
Source: IARC-CI5 Series; WHO Cancer Mortality Catabase
Figure 6 Trends in prostate cancer incidence (6 A ) and mortality rates (6 B ) (ASR per 100 000)
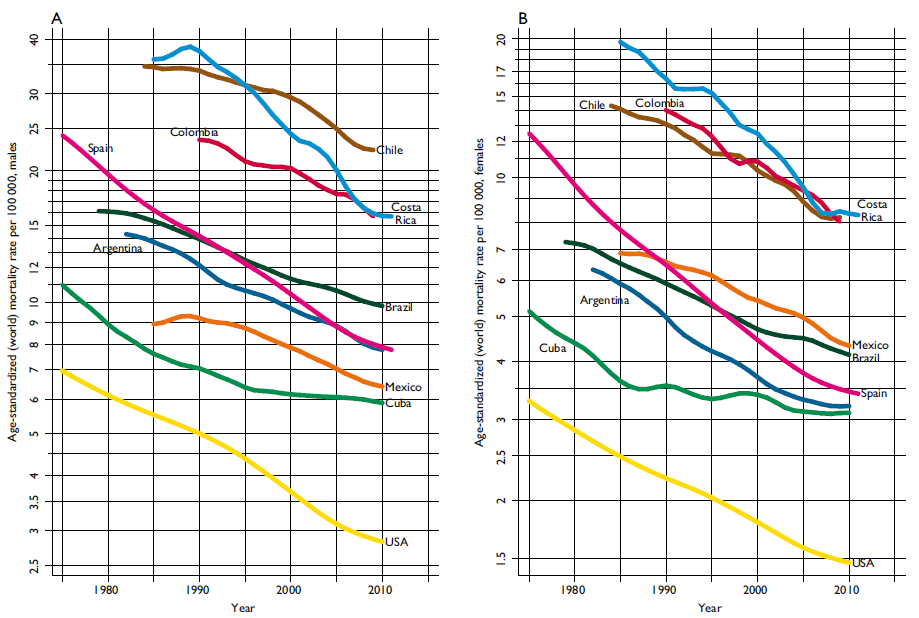
An illustrative marker of development and extent of westernization, colorectal cancer now ranks as a top five cancer in all three sub-regions, and is the second and third leading cause of cancer death in South America and the Caribbean, respectively (figure 1). Indeed, cumulative risk of death from colorectal cancer among males is around 2% in Uruguay and Argentina in the former region, and in Barbados and Trinidad and Tobago in the latter. A similar profile is seen in women, although it is Cuba along with Barbados that have the highest risks, around 1.5%. Trends in colorectal mortality (figure 7a and 7b) are similar to incidence (data not shown) where populations correspond: there are rapid increases in most LAC countries in both sexes, particularly in Brazil, Chile and Mexico, while rates are stable or increasing in high-risk Cuba (with rates surpassing the U.S. in the early-1990s). Rates are more stable among women in Argentina and possibly declining of recent in among Costa Rican males.
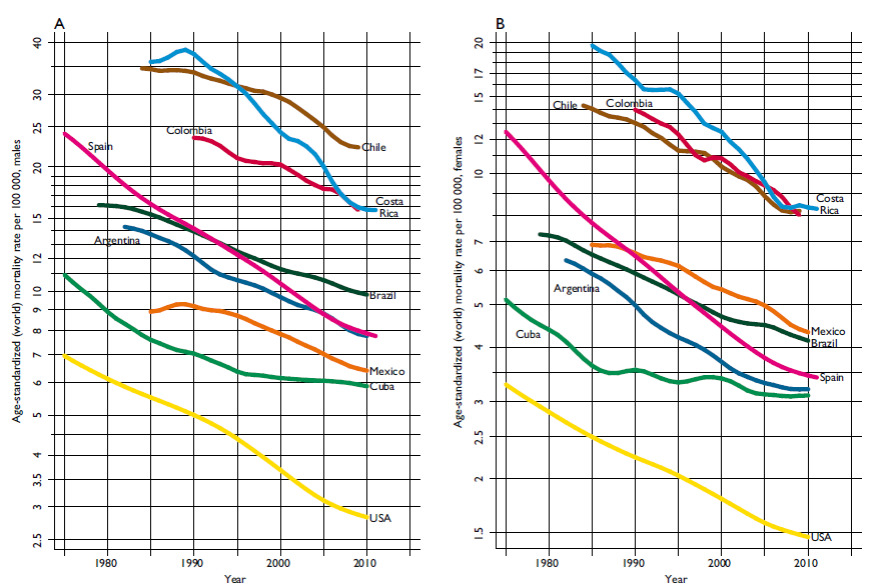
Source: reference 7
Figure 7 Trends in colorectal cancer mortality rates, males (7 A ) and females (7 B ) (ASR per 100 000)
Infection-related cancers are also frequent cancer forms in LAC: cervical and stomach cancer rank among the top five cancers in terms of incidence and mortality, respectively, in each of the three regions (figure 1). In Central America, stomach cancer is the leading cause of cancer death, while liver cancer ranks third. The highest risks for stomach cancer among males can be observed in Chile and Guatemala, where rates are 2.5-fold those in U.S. males. In females, the cumulative risk of stomach cancer in Guatemala is by far the highest in LAC, and unlike the vast majority of countries, rates are equivalent to those in men. As with incidence, mortality rates in both males and females have been uniformly declining in the last decades, with the sharpest decrease observed in Costa Rica, where historically rates have been among the highest in the regio (figures 8a and 8b).
Source: reference 7
Figure 8 Trends in stomach cancer mortality rates, males (8 A ) and females (8 B ) (ASR per 100 000)
For cervical cancer, the highest cumulative risks of mortality in Guyana, Bolivia and Nicaragua of 2.5, 2.4, and 2.0% respectively are seven to eight times greater than the corresponding estimates for Spain and the U.S. (figure 3). Incidence rates have been rapidly falling in the last decades in most countries where data is available, with the most prominent declines seen in women in Costa Rica (figure 9).
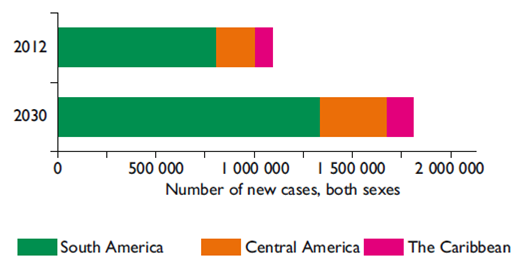
Burden projections to 2030
Figure 10 portrays the increasing cancer burden expected in the LAC region over the next decades. Incidence will rise from the 1.1 million new cases, as estimated in 2012, to over 1.6 million by 2030 (a 66% increase), assuming rates remain unchanged and allowing for the joint demographic effects of population ageing and population growth in the region. Based on these assumptions, the increase will be 50.2, 66.3 and 73.6% for The Caribbean, South America and Central America, respectively.
Discussion
The burden, patterns and trends of cancer in the LAC region reflect the major and ongoing sociodemographic transitions in the region: while prostate cancer and breast cancer are the leading causes of cancer in the majority of countries, stomach cancer and cervical cancer continue to be the most important cancers in lesser developed countries within the region. Overall, cancer incidence rates in LAC are relatively low compared with western countries, but cancer mortality rates are relatively high, as are M/I ratios, a proxy of case-fatality, as has been reported previously.4,8 Contributing factors include the case-mix linked to the extent of epidemiological transition in different countries, but also inferior outcomes, including advanced stage at diagnosis and limited access to and uptake of, effective treatment,4,9,10 linked to the capacity of health systems to implement effective early detection and cancer management strategies. Population-based cancer survival information is essential to elucidate the quality, host, tumour and health care-related factors that operate and influence survival proportions. Unfortunately there is at present only limited comparable statistics on cancer survival being generated within the region. Longer-standing population based cancer registries like Costa Rica have participated in several global studies,11,12 and more recently five LAC countries were able to participate in the latest available global comparison showing, as an example, moderate improvements in breast cancer survival between 1995-99 and 2005-09.13
In term of cancer incidence and mortality, the estimated burden was rather similar in most countries in both sexes, although the Caribbean has a distinct pattern of higher rates, particularly among males. For mortality this may be due in part to the elevated breast and prostate cancer rates among black populations in the sub-region, combined with outcome disparities and an increased risk of death for both cancers, as reported in other settings.14-19
Lung cancer was the first cause of death in two of the sub-regions but warrants cautious interpretation on considering the relatively low rates of lung cancer incidence and the fact that mortality should closely follow incidence given the consistently poor prognosis from this cancer. The underlying inferior quality of death certificates cannot be excluded as a possible explanatory artefact. A recent study has shown that general accuracy of vital statistics has worsened in Argentina, Colombia and México during the period 2000-2011,20 but is countered by one Colombian study that reported the reasonable quality of death certification for cancer deaths.21 The declining lung cancer mortality rates observed among males in the seven countries with mortality data, accompanied by rising rates among females, probably reflects the historical and gender-specific smoking profiles, with smoking prevalence among men earlier and falling versus a later and rising smoking uptake among women. Unfortunately, there is no comparable long-term information for smoking trends in most countries, though presently all countries in the region have signed the WHO Framework Convention on Tobacco Control (WHO FCTC) and have advanced recommended measures.22,23
Two infection-related cancers -stomach and cervical cancer- still represent a major part of the cancer burden in the region. The observed decreasing stomach cancer mortality rates both among males and females are consistent with worldwide findings,24 but rates remain double those observed in the U.S., ranking highest in Central America. Stomach cancer incidence rates in the region are also among the highest in the world, with elevated risks particularly associated to high mountainous regions,25 the only distinct feature in the region compared to the other established risk factors.26 Although stomach cancer survival is reported as below 30%,13 timely access to effective early diagnosis and treatment have proven effective in some Asian countries, and efforts to introduce such approaches while reducing disparities in the quality of care are needed to improve survival in some countries.9
Marked declines in cervical cancer incidence in selected regional cancer registries in LAC were evident yet rates are still elevated relative to the U.S. or Spain, lending support to the proposal to integrate HPV vaccination and organized screening programmes.27 There has been political support to the HPV vaccine in the region and by 2014, with 18 countries in Central America and South America already offered HPV vaccine through public immunization programs.28 Impact is expected to be seen only in the long term - mathematical models indicate that a 50% reduction in invasive cervical cancer will take four decades based on vaccination of 70% of 12-year-old girls based on current vaccines. Short-term reductions can however be gained by a focus on timely diagnosis and curative treatment via cost-effective organised screening programmes.
Cancers of the female breast, prostate and colorectum are major causes of cancer in the LAC region: breast and prostate cancer represent the leading cancers, in terms of both incidence and mortality in men and women respectively, in the majority of countries. The upwards trends in each cancer type are partly markers of a transitioning social and economic development in most countries, and from a broad epidemiological perspective, a changing prevalence and distribution of reproductive, dietary, and hormonal risk factors, as societies become more prosperous and industrialized, possibly enforced or reinforced by concomitant changes in the built environment. Enhanced levels of diagnostic testing and screening in some LAC countries are probably also drivers of the respective increment in prostate and breast cancer incidence, given precursor lesions are not the target of the intervention.29
Of greatest concern are the rising mortality trends of these cancers in selected LAC countries, in stark contrast to the U.S., for example, where increased early detection, and multiple modest improvements in treatment of each of these three cancers have led to substantial progress in reducing all-cancer mortality rates.30 The increasing trends in colorectal mortality (mirroring incidence), most markedly in Brazil, Chile and Mexico may pertain to changes in diet (e.g. intake of fruit and vegetables, fibre, red and processed meat, alcohol consumption), physical activity and overweight and obesity. Obesity is an increasing problem in Latin America and is the leading overall risk factor for disease in South America.4 The lack of recent mortality declines indicates a limited availability of programmes of earlier diagnosis (detection and removal of precancerous polyps via screening) as well as curative treatment, when one contrasts the country-specific trends in LAC with the downwards trends in the U.S.30
For breast cancer, the rapid declines in mortality observed in Spain and the U.S. are partially matched only in Argentina and Chile, while rates are stable in Mexico and Colombia, and rising in Brazil and Cuba. Chile, on the other hand, has demonstrated advances in early breast cancer diagnosis, with early stage breast cancer cases increasing from 43% in 1999 to 70% of all diagnosed cases by 2003,31 while mammography screening was initiated into the primary care programme in 2001. In other South American countries including Peru, Colombia, and Mexico about half of all breast cancer cases have been reported as detected in advanced stages.10
Recent declines in prostate cancer mortality rates in Chile, Argentina, Costa Rica and Mexico would suggest improvements in the management of the disease including the introduction of curative therapy as early as the late-1990s, while the rapid increases in incidence in the registry catchment areas are indicative of an increased use of PSA testing, although largely unknown risk factor changes may also contribute. Others have reported, given the relatively high mortality rates, limited early detection in the region, with many patients diagnosed with advanced disease.32 Most alarming then are the upwards trends in Brazil and Cuba, with rates rising similarly to those of incidence in the former country. Changes in the diagnosis and certification of prostate cancer have also been postulated as an explanation for the mortality inclines, particularly among the elderly.33
The present article provides a comprehensive overview of the descriptive epidemiology of cancer in 31 countries of the region presented by sub regions and compared to the world, the U.S and Spain to provide a global perspective. Attention must be drawn to the fact that given the lack of availability of incidence data, the major source of information were the GLOBOCAN estimates. High quality cancer registration in the LAC region for the period 2003-2007 covers less than 10% of the population while in North America the equivalent coverage is 83% and in Europe 32%.34 Though important advances in cancer registration have been achieved in Latin America, much is still to be done to fill the cancer surveillance gaps and significant improvements in quality, coverage and use of data are needed. A complete situation analysis of cancer registration, alongside considerations for improving cancer surveillance in the region are presented elsewhere (Piñeros M et al., submitted 2015). Sustained cancer registration will provide the basis for robust survival data, of limited availability from cancer registries at present, and essential to monitor health system policies and equity in cancer diagnosis and treatment at the population level. The Global Initiative on Cancer Registry Development (GICR), coordinated by the International Agency for Research on Cancer (IARC) represents an international effort to reduce disparities in cancer information in low and middle income-countries. The IARC Regional Hub in Latin America and the GICR partners look forward to provide the needed technical support, training, advocacy and networking supported by national and regional experts in cancer surveillance.
Conclusions
Cancer patterns and trends in the LAC region reflect the significant sociodemographic changes that the countries in Latin America and the Caribbean are undergoing. The continuing coexistence of infection-related cancers and the emergence of "westernized" cancers in the cancer profile together with the projected increase in burden impose great challenges to national health care systems to respond accordingly, particularly in the lesser developed countries in the region. Major efforts are also required to improve cancer surveillance in the region as the evidence base for planning and evaluating cancer control interventions.

