










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.57 supl.1 Cuernavaca 2015
Artículo original
Prospective study of the link between overweight/obesity and diabetes incidence among Mexican older adults: 2001-2012
Estudio prospectivo de la asociación entre sobrepeso/obesidad e incidencia de diabetes en adultos mayores en México: 2001 -2012
Guido Pinto, PhD,(1) Hiram Beltrán-Sánchez, PhD.(1)
(1) Center for Demography & Ecology, University of Wisconsin-Madison. Wisconsin, USA.
Abstract
Objective. To prospectively assess the relationship between overweight/obesity and incidence of type 2 diabetes mellitus (T2DM) among Mexicans aged 50+, assessing effects of age, genetic predisposition, education, physical activity, and place of residence.
Materials and methods. The Mexican Health and Aging Study (MHAS) was used to prospectively follow respondents free of diabetes in 2001 who became diabetic by 2012. Multivariate random effects logistic regression was used to assess covariates effects on the incidence of T2DM.
Results. Obese or overweight individuals at baseline (2001) were about 3 and 2 times, respectively, significantly more likely to become diabetic by 2012. Genetic predisposition increases the risk of diabetes by about three times compared to those with no family history of diabetes.
Conclusion. Overweight/obesity and genetic predisposition are the primary drivers of diabetes incidence among Mexican older adults. Reducing body weight and having access to health care may amel iorate the disease burden of T2DM.
Key words: diabetes mellitus; obesity; overweight; health of the elderly; adult health, Mexico.
Resumen
Objetivo. Cuantificar prospectivamente la relación entre sobrepeso/obesidad e incidencia de diabetes entre mexicanos mayores de 50 años mediante la medición de los efectos de la edad, predisposición genética, educación, actividad física y lugar de residencia.
Material y métodos. Se utilizó el Estudio Nacional de Salud y Envejecimiento en México (Enasem) para seguir a adultos mayores sin diabetes en 2001 y que se convirtieron en diabéticos en 2012. Se utilizó el modelo de regresión logística de efectos aleatorios para cuantificar el efecto de covariables en la incidencia de diabetes.
Resultados. Quienes tenían obesidad y sobrepeso en 2001 fueron 3 y 2 veces más propensos a adquirir diabetes en 2012, respectivamente. La predisposición genética aumentó tres veces el riesgo de padecer diabetes en comparación con aquéllos sin historia familiar de diabetes.
Conclusiones. Sobrepeso, obesidad y predisposición genética son causantes de diabetes en adultos mayores mexicanos. Reducción de peso y acceso a atención de salud podrían reducir las consecuencias que tiene la diabetes.
Palabras clave: diabetes mellitus; obesidad; sobrepeso; salud de la persona mayor; salud del adulto; México.
Prevalence of adult obesity in Mexico has grown at an unprecedented pace during the last two decades, reaching the highest level (33%) in the Latin America region in 2012.1 The health consequences of overweight and obesity are beginning to emerge as exemplified by the increasing prevalence and disease toll from type 2 diabetes mellitus (T2DM), particularly among older adults.2'3
Epidemiologic evidence consistently shows that being overweight or obese is a major risk factor for developing T2DM. In Mexico, evidence indicates that overweight or obese individuals have a higher likelihood of having T2DM.4-6 In addition, prevalence of overweight and obesity differs significantly by sex, socioeconomic status (SES) and place of residence,7,8 suggesting that T2DM status also varies by these factors. Only a small number of epidemiologic studies have estimated this relationship in Mexico (e.g., in Mexico City9). Yet, these studies are not nationally representative of the older adult Mexican population and are usually based on cross-sectional data, which limit our understanding of the relationship between overweight/obesity and T2DM as the latter condition develops over the individual's life course.
In this paper we study the link between overweight/obesity and incidence of T2DM among older adults using nationally representative prospective data of Mexico. Our study adds to the existent literature in two main areas. First, we clarify how overweight/ obesity links with the incidence of T2DM among Mexicans aged 50 or older by exploiting the prospective (longitudinal) nature of the Mexican Health and Aging Study (MHAS in English or Enasem in Spanish) between 2001 and 2012. We improve the assessment of this relationship by using robust longitudinal methods that result in incidence estimates that control for unobserved con-founders present in cross-sectional data and account for time dependence in the variables of interest. As most studies document this link in high-income countries, we extend previous research by analyzing this association in a nationally representative sample of older Mexican adults. Second, as the association between overweight/ obesity and T2DM is likely to vary by place of residence, education and between younger and older adults, we examine this association by controlling for area of residence (urban/rural), educational level (no education/elementary/secondary or more), and age groups (50-64/ 65-79 / 80 or older). This allows us to get a better understanding of the incidence of T2DM across population subgroups.
Materials and methods
Data
Our analysis is conducted on individual-level data from a prospective three-wave panel study of a nationally representative cohort of Mexican adults ages 50 and older at the baseline (2001), the MHAS. MHAS is designed to have both urban and rural representation and provides data on demographic traits, self-perceived health status and chronic conditions, lifestyle choices (tobacco use, alcohol consumption, or physical activities), functional and cognitive performance, labor and economic status, income and assets, transfers, family arrangements, use of health services, health insurance and housing. The study was approved by the Institutional Review Boards or Ethics Committees of the University of Texas Medical Branch in the United States, as wellas the Instituto Nacional de Estadística y Geografía (INEGI) and the Instituto Nacional de Salud Pública (INSP) in Mexico. Detailed information on the MHAS survey design is presented elsewhere.10
The MHAS dataset includes information from three waves: 2001,2003 and 2012. The sample baseline consists of 15 402 interviews gathered during 2001. The second wave was conducted during 2003; questionnaires were administered to 14 386 surviving respondents and a new sample of 220 new spouses. Finally, a third survey was carried out during 2012 including 12 569 respondents and a new replacement sample of 5 896 new subjects and spouses. In this study, we use all respondents and their spouses aged 50 or more interviewed at baseline and in any of the two follow-up waves.
At baseline, 10 919 persons out of 15 402 were diabetes free, and during the follow-up period, 1 640 respondents became diabetic, either by 2003 (487) or by 2012 (1 153).
Measures
Diabetes was measured using self-reported information obtained from the following question: "Has a doctor or medical personnel ever told you that you have diabetes or high blood sugar levels?" The variable "diabetes" takes the value of 1 if the respondent says "yes" to the previous question in 2001,2003 and 2012. Body weight and height are also based on self-reports and body mass index (BMI) is computed as weight divided by the square of height. We used the WHO11 standard cut-off to define BMI categories as underweight (< 18.5), normal or healthy weight (18.5 to 25), overweight (25 to 30) and obese (> 30). In all statistical models, the control group corresponds to healthy weight individuals. Thus, coefficient estimates represent the effect of being obese, overweight, or underweight on diabetes relative to their normal-BMI counterparts.
We consider how the incidence of T2DM is associated with three main factors: a) genetic predisposition coded as 1 if either the respondent's parents or siblings were told by a physician or medical personnel they have diabetes and 0 otherwise; b) physical activity coded as 1 if the respondent reported having exercised, or done some hard physical activity three or more times a week, and 0 otherwise, and c) smoking status, coded as 1 if the respondent currently smokes (active smoker) and 0 otherwise. We additionally control for respondent's age using three categorical variables: 50-64,65-79, and 80 + years old, and two additional variables to account for socioeconomic differences: a) education coded as three categorical variables: no education (0 years of schooling), elementary (1 to 6 years of schooling), and secondary or more (7 + years of schooling); b) current place of residence coded as 1 if respondent lived in an urban area (locality size more than 15 000 inhabitants) and 0 if respondent lived in a rural site (locality size less than 15 000 inhabitants).
Methods
To model incidence of T2DM we used a random effects logistic regression model especially suited to handle longitudinal data. We begin our analysis with a sample of diabetes-free individuals in 2001 and modeled their transition into (incidence of) T2DM by the follow-up in either 2003 or 2012. This model takes into account differences across and between individuals that could have an influence on T2DM.
The model assumes that diabetes is not directly observable but instead it is reported by the respondents themselves and represented by a binary variable. The propensity-to-diabetes equation is specified over individuals (i) and time (t) as follows:

where Educ=education, PA=physical activity, GP=genetic predisposition, Smk=current smoker, μi=between-individual error, and εit= within-individual error.
"Diabetes" is the chronic condition reported by the respondent. This model specification monitors the effects of respondent's individual traits such as BMI category, age, education, smoking, physical activities, genetic predisposition, and place of residence on T2DM incidence. We additionally included a time variable that accounts for changes over time in the incidence rate of self-reported diabetes. We estimated three models: for the total population (i.e., pooled sample with a sex indicator), and separately for males and females.
Results
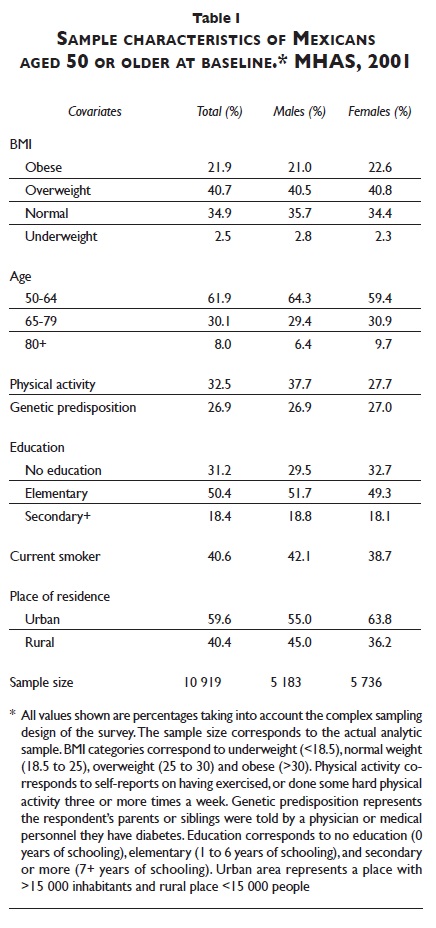
Descriptive characteristics of the studied sample in 2001 are displayed in table I. Results indicate that almost two-thirds (63%) of the older adult Mexican population is either overweight (41%) or obese (22%), with slightly higher obesity and overweight prevalence among females. Physical activity shows that about one-third (33%) reported having exercised or done some physical activity three or more times a week with higher prevalence among males. Similarly, about one-fourth of the sampled population self-reports having parents or siblings with diabetes (genetic predisposition to diabetes), according to a physician or medical personnel. About half of the older Mexican population reported having some elementary education, with another one-third having no schooling and the remaining one-fifth with secondary or more. Males tend to show slightly higher proportions of schooling (either elementary or secondary or plus) than females.
Changes in diabetes status by age and BMI categories are shown in figure 1. Results clearly show that obese or overweight individuals at baseline were more likely to become diabetic by 2012; while the opposite is true for underweight people. These patterns are similar for males and females, although obese or overweight males become diabetic in larger numbers than females. For instance, about one-third of obese males aged 50-59 in 2001 became diabetic by 2012, while the corresponding fraction among females is only one-fifth Differences in diabetes incidence by BMI categories reduce at older ages reaching levels of about 10%.
The net effect of obesity on diabetes incidence
Results from multivariate logistic random effect models assessing the incidence of diabetes with overweight / obesity are shown in table II. These results show net effects of overweight/obesity and genetic predisposition on diabetes; that is, the effects that are not "confounded" by all other factors included in the model. Results show positive and statistically significant effects of overweight and obesity as well as hereditary factors on the incidence of diabetes, after controlling for other individual traits.
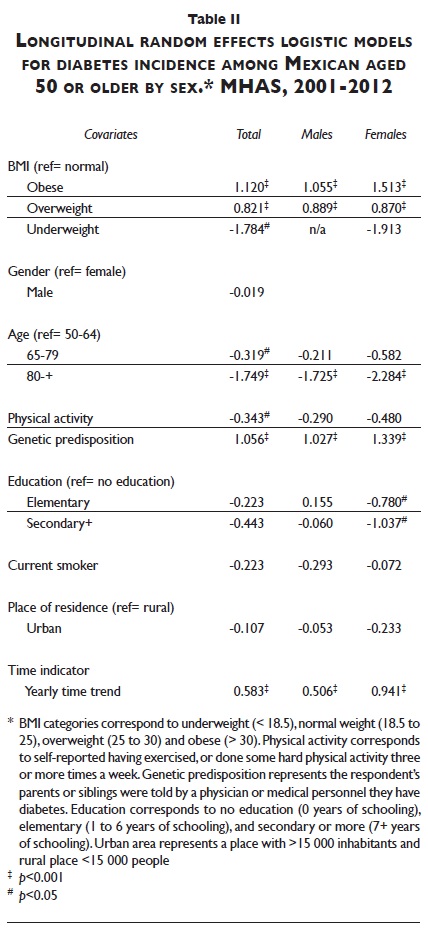
In fact, obese or overweight individuals were more likely to develop diabetes over the follow-up period relative to normal BMI individuals; while underweight respondents show a negative association, suggesting that they were less likely to develop this chronic condition during the period of study. For example, being obese or overweight at baseline increases the likelihood of developing T2DM by about 3 and 2 times, respectively, over an 11-year follow-up period relative to their normal-BMI counterparts.
Genetic predisposition to diabetes also has a strong positive effect in this population. Having parents or siblings diagnosed with T2DM increases the risk of developing the disease by almost three times compared to those with no-family history of diabetes.
The remaining variables also show significant effects on diabetes in the expected direction. For example, being active reduces the chances of being diabetic by almost 1.5 times when compared to no-active respondents. Importantly, younger older adults (aged 50-64) are more likely to become diabetic than their older counterparts (aged 65-79 and 80 or older). Finally, individuals with low levels of education (no schooling) are more likely to become diabetic than to those with secondary or higher education Results also show no significant difference in the incidence of diabetes by smoking status and place of residence (urban vs. rural).
Overall, there is a similar association between each factor and the incidence of T2DM for both males and females, but there are some noticeable differences. For instance, relative to normal BMI respondents, obese females are about 4.5 times more likely to become diabetic over the follow-up period, compared to an about 2.9 times higher likelihood among obese males. Similarly, hereditary factors increase more strongly the predisposition of becoming diabetic among women (3.8 times) than men (2.7 times), holding constant all other factors in the respective models. Additionally, there are no educational differences in the likelihood of developing T2DM among males but females with no schooling are significantly more likely to become diabetic relative to their counterparts with some schooling (either elementary or secondary or more education). Finally, physical activity does not seem to have a significant effect on T2DM incidence among males and females.
Discussion
Random-effects logit regression models using data from MHAS produces positive, strong, and significant estimates of the effect of overweight/ obesity on T2DM at the population-level, after adjusting for respondent's individual traits. Our results indicate that obesity and overweight are strongly and significantly associated with the incidence of T2DM among older Mexican adults: obese or overweight individuals are about 3 and 2 times, respectively, more likely to develop T2DM than their normal-BMI counterparts over an 11-year period. This result raises important concerns given the rapid increase in overweight and obesity prevalence among older adults (aged 50 or more) in the last decade.12 The rapid growth in body weight among Mexicans has been fueled by recent changes in both nutritional intake and the epidemiologic profile, which have led to improvements in health and survival status.13'14 However, these changes may have reached a point of diminishing returns as Mexico switched from a state of under-nutrition to over-nutrition in a short period of time.4
In addition, young older adults (aged 50-64) were significantly more likely to become diabetic over an 11-year period than their older counterparts (aged 65+). This result can have important implications for the health status of the upcoming aging population and the future mortality prospects of older Mexican adults. For instance, there is evidence indicating that diabetes is associated with large reductions in overall life expectancy15 and disability-free life expectancy among older Mexican adults.16
Our results also show a strong association between genetic predisposition and T2DM. Individuals with this trait have about three times higher likelihood of developing diabetes as they age, net of obesity/overweight and other inter-individual characteristics. In addition, about one-third (31%) of older adults (table I) self-reported a genetic predisposition to diabetes. These results underscore the significance of access to health care for older Mexican adults, particularly that of Seguro Popular.17'18 For instance, preventive care may allow these individuals to get an early diagnosis of the disease thereby reducing the disease associated comorbidities. Similarly, access to health care can also provide patients with adequate medical treatment to reduce the progression of the disease and its associated health consequences. This is particularly important since previous evidence indicates that a large portion of diabetic patients (85%) aged 20 or older in 2006 received poor medical treatment19 which have led to sizeable economic costs and disease burden due to diabetes.20
Thus, the findings gleaned in this paper provide additional evidence of the role of obesity/overweight and genetic predisposition as the main and independent drivers of diabetes. This means that reductions in obesity rates may lead to important declines in morbidity and mortality from diabetes, which consequently may lead to cost reductions for the health system. For instance, diabetes is the leading cause of death among women and the third among men in Mexico.21
This study has a limitation. We rely on self-reported data on diabetes, body weight and height which may be producing some bias in our estimates. On the one hand, self-reported diabetes may bias our estimates resulting from undiagnosed cases; however, if this is the case, our estimates will likely lead to lower than expected coefficient estimates which suggest that our results are indeed conservative (i.e., lower bounds). On the other hand, self-reported weight and height could bias effects of overweight/obesity if there is large discrepancy between objective measures and self-reports. However, evidence shows significant agreement between self-reported height and weight and objective measures in MHAS22 and lack of agreement between objective measures and self-reports has been shown to be mostly attributable to random noise.23 Thus, although consistency between self-reports and objective measures varies by age and gender, the overall concordance of measures in MHAS is surprisingly high and secures valid inferences.22
Diabetes as a major chronic disease places a high burden due to its associated comorbidities and increased medical costs as well as for being a risk factor for old-age disability and mortality. Diabetes prevalence in the adult Mexican population (aged 20 or older) has more than doubled between 1994 and 2006, from 6.7 to 14.4%,2 but it remained fairly constant between 2006 and 2012 at about 14%.12 However, the prevalence among older adults is much higher, reaching about 19 and 24% among those aged 50-59 and 60-79, respectively, in 2012.12 In addition, the majority of diabetic patients (85%) aged 20 or older in 2006 have been reported to receive poor medical treatment, regardless of their access to health care, type of institution, or type of health insurance.19 As a result of poor disease control, there are sizeable economic costs and disease burden associated with diabetes; some research suggests that diabetes accounts for about 7% of all health expenditures in Mexico.20
References
1. Food and Agriculture Organization of the United Nations.The state of food and agriculture 2013. Rome: FAQ 2013. [ Links ]
2. Barquera S, Campos-Nonato l, Aguilar-Salinas C, López-Ridaura R, Arredondo A Rivera-Dommarco J. Diabetes in Mexico: cost and management of diabetes and its complications and challenges for health policy. Global Health 2013;9:3. [ Links ]
3. Hernández-Ávila M, Gutiérrez JP, Reynoso-Noverón N. Diabetes mellitus en México. El estado de la epidemia. Salud Publica Mex 2013;55 suppl 2:129-136. [ Links ]
4. Beltrán-Sánchez H, Crimmins EM. Biological risk in the Mexican population at the turn of the 21 st Century.J Cross Cul Gerontol 20I3;28(3):299-3I6. [ Links ]
5. García-García E, Aguilar-Salinas CA, Tusié-Luna T, Rull-Rodrigo JA. Early-onset type 2 diabetes in Mexico. Isr Med Assoc J 2002;4(6):444-448. [ Links ]
6. Aguilar-Salinas CA, Vázquez-Chávez C, Gamboa-Marrufo R, García-Soto N, de Jesús Ríos-González J, Holguín R, et al. Obesity, diabetes, hypertension, and tobacco consumption in an urban adult Mexican population. Arch Med Res 200I;32(5):446-4S3. [ Links ]
7. Smith KY Goldman N. Socioeconomic differences in health among older adults in Mexico. Soc Sci Med 2007;6S(7): 1372-1385. [ Links ]
8. Wong R, Ofstedal M, Yount K, Agree E. Unhealthy lifestyles among older adults: exploring transitions in Mexico and the U.S. Eur J Ageing 2008;S(4):311-326. [ Links ]
9. González C, Stern MR González E, Rivera D, Simón J, Islas S, et al.The Mexico City Diabetes Study: a population-based approach to the study of genetic and environmental interactions in the pathogenesis of obesity and diabetes. Nutr Rev 1999;57(5):71-76. [ Links ]
10. Wong R, Peláez M, Palloni A Markides K. Survey data for the study of aging in Latin America and the Caribbean: selected studies.J Aging Health 2006;18:157-179. [ Links ]
11. WHO Expert Committee on Physical Status. Physical status: the use and interpretation of anthropometry: report of a WHO Expert Committee. Geneva: WHO, 1995. [ Links ]
12. Gutiérrez JR Rivera-Dommarco J, Shamah-Levy T, Villalpando-Hernández S, Franco A Cuevas-Nasu L, et al. Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales. Cuernavaca, México: INSR 2012. [ Links ]
13. Rivera JA Barquera S, Campirano F, Campos I, Safdie M, Tovar V. Epidemiological and nutritional transition in Mexico: rapid increase of non-communicable chronic diseases and obesity. Public Health Nutr 2002;5(IA):113-122. [ Links ]
14. Rivera J A Barquera S, González-CossíoT, Olaiz G, SepulvedaJ. Nutrition transition in Mexico and in other Latin American countries. Nutr Rev 2004;62(7 Pt 2):S 149-S157. [ Links ]
15. Palloni A Beltrán-Sánchez H, Novak B, Pinto G, Wong R.Adult obesity, disease and longevity in Mexico. Salud Publica Mex 2015;57 suppl I :S22-S30. [ Links ]
16. Andrade FCD Measuring the Impact of diabetes on life expectancy and disability-free life expectancy among older adults in Mexico. J Gerontol B Psychol Sci Soc Sci 2010 2010;65B(3):381 -389. [ Links ]
17. Knaul FM, González-Pier E, Gómez-Dantés O, García-Junco D, Arreola-Ornelas H, Barraza-Lloréns M, et al. The quest for universal health coverage: achieving social protection for all in Mexico. Lancet 2012;380(9849): 1259-1279. [ Links ]
18. Beltrán-Sánchez H, Drummond-Andrade FC, Riosmena F. Contributions of socioeconomic factors and health care access on the awareness and treatment of diabetes and hypertension among older Mexican adults. Salud Publica Mex 2015;57 suppl 1 :S6-S14. [ Links ]
19. González-Villalpando C, López-Ridaura R, Campuzano JC, González-Villalpando ME. The status of diabetes care in Mexican population: are we making a difference? Results of the National Health and Nutrition Survey 2006. Salud Publica Mex 2010;52:S36-S43. [ Links ]
20. Ávila-Burgos L, Cahuana-Hurtado L, González-Domínguez D, Centro de Investigación en Sistemas de Salud (Mexico). Cuentas en diabetes mellitus, enfermedades cardiovasculares y obesidad: México 2006.1. ed. Cuernavaca, Morelos, México: INSR 2009. [ Links ]
21. CONAPO.Principales causas de mortalidad en Mexico, 1980-2007 [documento en internet].2010. [consultado el I de noviembre de 2013]. Disponible en: http://www.conapo.gob.mx/en/CONAPO/Principales_causas_de_mortalidad_en_Mexico_l980_2007. [ Links ]
22. Ávila-Funes JA Gutiérrez-Robledo LM, Ponce-De León-Rosales S. Validity of height and weight self-report in Mexican adults: Results from the National Health and Aging Study. Journal Nutr Health Aging 2004;8(5):355-36l. [ Links ]
23. Palloni A Soldo B,Wong R.The accuracy of self-reported anthropometric: obesity and older Mexicans. Population Association of America Meetings; 2003; May 1-3; Minneapolis, USA. [ Links ]
Received on: December 9, 2013
Accepted on: December 9, 2014
 Corresponding author:
Corresponding author:
Dr. Guido Pinto.
Center for Demography & Ecology, University of Wisconsin-Madison.
1180 Observatory Drive, Madison. WI 53706-1393 Wisconsin, USA.
E-mail: pinto@ssc.wisc.edu.
Declaration of conflict of interests. The authors declare that they have no conflict of interests.
