










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.56 no.4 Cuernavaca jul./ago. 2014
Cartas al editor
Malignant mesothelioma trends in Chihuahua, Mexico
Dear Editor: Malignant mesothelioma is an aggressive neoplasm originated primarily in the mesothelial cells of the pleura, and largely attributed to asbestos exposure and with a five–year survival rate estimated at less than 10%.1 Because of the transfer to our country of manufacturing industries of asbestos products banned in Europe, US and Canada, some authors have speculated that it could be reflected in an increase on the incidence of mesothelioma.2 Physicians from Chihuahua city have a perception that there is a high number of new mesothelioma cases each year, so we decided to conduct a survey addressed to the departments of Pathology, including those with immunohistochemistry facilities, in order to investigate how fast this neoplasia spreads in the municipality. Likewise, we wanted to analyze the epidemiological behavior of mesothelioma in relation to other diseases with a similar clinical pattern, and which are included in its differential diagnosis.
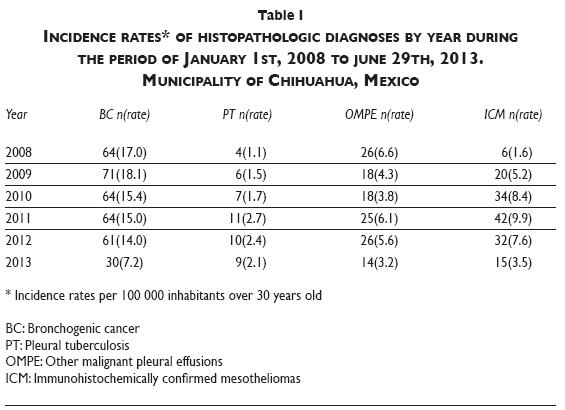
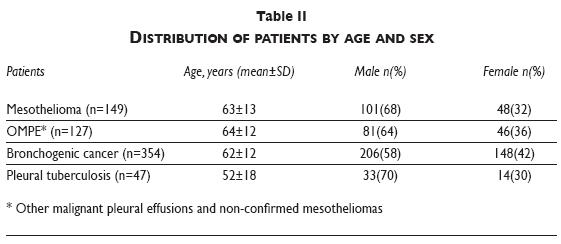
The survey gathered data from patients older than 30 years during the period of January 1st, 2008 to June 29th, 2013. Histopathologic diagnoses were included for immunohistochemically confirmed mesotheliomas (ICM), other malignant pleural effusions plus those unconfirmed mesotheliomas (OMPE), bronchogenic carcinoma (BC), and pleural tuberculosis (PT). The survey was applied in four departments of Pathology of public hospitals, plus the two largest private surgical hospitals, and the only two laboratories performing immunohistochemistry in the city. From a total of 276 pleural tumors diagnosed within the study period, 149 (54%) corresponded to ICM. The predominant histologic subtype was epithelioid mesothelioma, with 93%. By December 2012, new ICM cases per year averaged 27. This is of particular interest because our annual rates of mesothelioma reached or even surpassed those levels recognized as alarming in developed countries (2.9 cases per 100 000).3,4 The male–to–female ratio seen in our study population during the period was 2:1, which shows an important proportion of women and possibly represents a signal of a para–occupational exposure to asbestos.
At the beginning of the study period new OMPE cases were higher than ICM, but decreased over the following years as the incidence rate of ICM increased. This is possibly explained by more communication among local clinicians about the availability and usefulness of immunohistochemistry on pleural biopsies from suspected cases of mesothelioma. Furthermore, the observed OMPE/BC ratio exceeded that reported in the literature,5 suggesting the presence of other etiologies of effusions such as mesothelioma.
The incidence of lung cancer was higher than that of ICM and OMPE, averaging 16 cases per 100 000. The age and gender distribution of patients with BC and OMPE was similar from that shown by ICM and there was not a significant difference (p=0.28). The fact that our ICM cases shared the same age group with BC obviates this as a useful discriminatory variable. Patients with PT tended to be younger (p=0.00) and the incidence of the disease was far below the other studied groups despite the fact that in our country it is considered endemic. Based on the results of the survey, we conclude that Chihuahua city requires greater institutional resources for the confirmation of suspected cases of mesothelioma and that the possibility of performing an analysis of fiber concentrations for industrial and environmental asbestos should be seriously considered, in order to reinforce the implementation of pertinent regulatory measures.
René Agustín Flores–Franco, MD,(1)
Ernesto Ramos–Martínez, MD,(2,3)
Eduardo Luévano–Flores, MD,(3,4)
Ricardo Fierro–Murga, MD,(2)
Rocío Barriga–Acevedo, MD,(5)
María Elena Martínez–Tapia, MD,(6)
Arturo Luévano–González, MD,(4,7)
Antonio Gómez–Díaz, MD,(1)
Roberto Alfonso Perea–Sánchez, MD.(8)
(1) Hospital General Regional de Zona 1, Unidad Morelos, Instituto Mexicano del Seguro Social. Chihuahua, México. rflores99@prontomail.com
(2) Patología e Inmunohistoquímica de Chihuahua, S.C. Chihuahua, México.
(3) Hospital Centro Internacional de Medicina (CIMA). Chihuahua, México.
(4) Laboratorio de Patología Dr. Luévano. Chihuahua, México.
(5) Hospital Lázaro Cárdenas, Instituto de Seguridad y Servicios Sociales para los Trabajadores del Estado. Chihuahua, México.
(6) Hospital General Regional Dr. Salvador Zubirán Anchondo. Chihuahua, México.
(7) Hospital Christus Muguerza del Parque. Chihuahua, México.
(8) Hospital Central Universitario, Universidad Autónoma de Chihuahua. Chihuahua, México.
References
1. Samet JM, Alberg AJ, Ford JG. Epidemiology of lung cancer and mesothelioma. Eur Respir Mon 2009;44:349–391. [ Links ]
2. Aguilar–Madrid G, Juárez–Pérez CA, Markowitz S, Hernández–Ávila M, Sánchez–Román FR, Vázquez–Grameix JH. Globalization and the transfer of hazardous industry: asbestos in Mexico, 1979–2000. Int J Occup Environ Health 2003;9(3):272–279. [ Links ]
3. Weil H, Hughes JM, Churg AM. Changing trends in US mesothelioma incidence. Occup Environ Med 2004;61:438–441. [ Links ]
4. Bianchi C, Bianchi T. Malignant mesothelioma: global incidence and relationship with asbestos. Industrial Health 2007;45:379–387. [ Links ]
5. Scagliotti GV. Symptoms, signs and staging of lung cancer. In: Spiro SG. Lung cancer. Eur Respir Mon 2001;17:86–119. [ Links ]
