










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkSalud Pública de México
Print version ISSN 0036-3634
Salud pública Méx vol.55 suppl.3 Cuernavaca 2013
Artículo original
Effect of exercise dosages on adiposity indices in overweight girls
Efecto de programas de ejercicio en los índices de adiposidad en niñas con sobrepeso
Stephanie Kellam, MS,(1) Norma Olvera, PhD,(1) Patrick Leung, PhD,(2) Jian Liu, PhD,(3) Dennis Smith, PhD.(1)
(1) Health Program, College of Education, University of Houston. Houston, TX, USA.
(2) Graduate College of Social Work, University of Houston. Houston, TX, USA.
(3) Health and Human Performance, University of Houston. Houston, TX, USA.
Abstract
Objective. The primary purpose of this study was to determine the impact of two exercise dosages on reducing adiposity in minority girls.
Materials and methods. Sixty-two overweight Hispanic and African-American girls participated in one of two intense summer interventions in Houston, TX: Intervention A (exposure to about 40 hours physical activities) or Intervention B (exposure to 60 hours of physical activities). Adiposity indices (percent body fat, waist circumference, body mass index) were taken pre- and post-intervention.
Results. Intervention B had a significantly greater decrease in adiposity indicators (p= 0.006) when compared to Intervention A. Waist circumference displayed the most significant decrease (p = 0.001). Both interventions significantly increased daily minutes of moderate-to-vigorous physical activity (p= 0.020).
Conclusions. Intense physical activity interventions may effectively reduce abdominal fat in minority girls.
Key words: physical activity; body mass index; adipose tissue; abdominal fat.
Resumen
Objetivo. Determinar el impacto de dos programas de ejercicio en la reducción de los índices de adiposidad en niñas de grupos minoritarios.
Material y métodos. Sesenta y dos niñas latinas y africano-americanas participaron en una de dos intervenciones intensivas durante el verano: la intervención A (exposición a aproximadamente 40 horas de actividad física) o la intervención B (exposición a 60 horas de actividad física) en Houston, TX. Los indicadores de adiposidad (índice de masa corporal, porcentaje de grasa corporal y grasa abdominal) se midieron antes y después de cada intervención.
Resultados. La intervención B tuvo una disminución más significativa en el nivel de adiposidad (p=0.006) comparado con la intervención A. La circunferencia abdominal fue la que más disminuyó (p=0.001). Ambas intervenciones aumentaron significativamente la actividad física moderada a intensa (p=0.020).
Conclusiones. Las intervenciones cortas e intensas pueden ser efectivas en la reducción de la grasa abdominal en niñas de grupos minoritarios.
Palabras clave: actividad física; índice de masa corporal; tejido adiposo; grasa abdominal.
Between 1980 and 2002, the number of overweight children tripled in the US.1,2 Although obesity affects all children in the United States, minority children experience an increased risk of being overweight. Over the last 30 years, African-American (AA) and Hispanic children have experienced a much larger increase in overweight rate than Caucasian children.3 Estimates suggest that in 2007-2008, 39% of Hispanic and 36% of AA youth were overweight as compared to 29% of Caucasian children.1 Even after controlling for socioeconomic status and demographic factors, AA and Hispanic children had 80% odds of becoming obese compared to 34% odds for Caucasian children.4
Physical inactivity is often considered a major contributor to the current obesity epidemic among US children and adolescents.5,6 The US Health and Human Services recommends that children and adolescents engage in 60 minutes of moderate-to-vigorous physical activity (MVPA) daily to obtain health benefits and develop healthy lifestyle habits.7 Despite the prescribed dosage of physical activity, only a small percentage of American children meet this recommendation. Troiano et al.,8 reported that only 42% of children ages 6-11 years engaged in at least 60 minutes of daily MVPA when measured objectively. However, by ages 12-15, the percentage of adolescents meeting MVPA recommendation decreased severely to only 12% of boys and 3% of girls. Hispanic and AA children reported lower levels of physical activity4,5 and were less likely than the Caucasian children to have participated in any type of organized physical activity in the past seven days.9 Furthermore, Butte et al.10 reported that among Hispanic children, overweight girls had the lowest rates of MVPA compared to non-overweight girls and boys. The risk for inactivity combined with the risk for being overweight in Hispanic and AA children, particularly girls, highlights the need to develop interventions to promote MVPA and healthy weight in such populations.
Several literature reviews conducted by van Sluijs, McMinn, and Griffin11 indicated that few physical activity interventions have involved Hispanic and AA children, none of which included minority adolescents. Physical activity interventions have ranged from once per week for 12 weeks to three times per week for 12 months and the health outcomes (e.g., adiposity reduction) have been mixed. One explanation for the differing outcomes is the suggestion that the recommended physical activity dosage may have been insufficient to achieve weight loss.12 Thus, research is needed to investigate the different types of exercise dosages required to reduce adiposity in youth, particularly, minority children. The purpose of this study was to assess the efficacy of two exercise dosage intervention (Intervention A: 40 hours, 25 minutes vs. Intervention B: 60 hours) on reducing adiposity indices in minority girls. It is hypothesized that the Hispanic and AA girls who engage in intervention B will exhibit a greater decrease in percent body fat, waist circumference, and body mass index (BMI) when compared to those girls who complete intervention A.
Materials and methods
Participants
The baseline sample consisted of 75 overweight [body mass index (BMI) ≥85th percentile for age-sex specific] Hispanic and AA girls, ages 9-14 years. The target girls participated in one of two BOUNCE (Behavior Opportunities Uniting in Nutrition, Counseling, and Exercise) summer interventions conducted in 2007 and 2008, intervention A and B, respectively in Houston, TX. Study inclusion criteria required girls to be: 1) between ages 9-14 years; 2) of Hispanic or African American descent; 3) overweight (BMI equal to or greater than 85th percentile) status; 4) of low socioeconomic status as demonstrated by receiving free-lunch at school or government financial assistance, including WIC, Medicaid, or CHIP; 5) without physical activity restrictions that limit their active participation in the BOUNCE interventions as certified by a medical professional; and 6) willing to participate for the entire length of the intervention. Participants were recruited through referrals by school counselors, nurses, and teachers. Girls and their mothers signed an assent and informed consent respectively before administration of measurements. The University of Houston Committee for the Protection of Human Subjects reviewed and approved the research protocols and assent and consent forms.
Description of BOUNCE Interventions A and B
Both of the interventions were delivered from 9:00 AM to 5:00 PM, Monday through Friday during the month of July. A typical day at the BOUNCE intervention contained three-to four exercise sessions, one nutrition education session, and one behavioral counseling session as well as two healthy snacks and a healthy lunch. For the proposed study, we will focus on the description of the exercise component of the interventions.
Intervention A spanned a three-week period for a total of 15 days and offered 2 415 minutes (40 hours and 25 minutes) of exposure to a variety of physical activities (see Appendix A for a complete list); whereas Intervention B lasted four weeks and offered 3 600 minutes (60 hours) of physical activity exposure (see Appendix A for a complete list). In both interventions A and B, participating girls engaged in physical activity group sessions of varied intensity based on Ridley's compendium13 for energy expenditure in youth (light = 2 METS, moderate = 3-5 METS, vigorous = ≥ 6 METS). The BOUNCE exercise program consisted of 21 group physical activity sessions, categorized into flexibility, sports skills, games, traditional fitness, and dancing categories. Participants were exposed to traditional (e.g., sport skills, step aerobics, spinning) and nontraditional physical activities (e.g., yoga, pilates, ballet, cheerleading, rumba fitness, and salsa) with an aim to engage participants in diverse and fun ways to be active.
The BOUNCE exercise program was standardized with a typical day beginning with a flexibility session followed by a sports skills or games session. Lunch and a nutrition lesson were then followed by a traditional fitness session. Following a counseling session, the day would end with a dancing session. Schedule format and layout was similar across the two interventions. Each BOUNCE exercise session included a 5-minute warm-up, light to vigorous physical activity, and 5-minute cool-down phase. Instructors certified by the Cooper Institute led exercise sessions at a gymnasium and dance studio located on a university campus.
Several strategies to encourage active participation were employed. First, participants were asked to sign a contract at the beginning of the exercise program in which they agreed to engage in all physical activities. Second, beginning after the first week, participants received weekly reports of their levels of physical activity achieved in the previous week. Third, small prizes (e.g., notebooks, pencils, bracelets, etc.) were awarded to participants who reached their own weekly goals. Fourth, participants received handouts on exercise benefits, components of a healthy lifestyle, and strategies for overcoming barriers to being physically active. The Social Cognitive Theory14 guided the design of both BOUNCE interventions, with an emphasis on knowledge, skill building, social support, positive outcome expectations, and reinforcement.
Measures
Trained data collectors conducted the study assessments at the baseline and end of interventions A and B, with the exception of physical activity data that was collected during the entire duration of interventions to determine physical activity compliance.
Demographic data were obtained through questions about age, date and place of birth, and self-described ethnicity. Anthropometric measures of body height and weight were measured to the nearest 0.1 cm and 0.1 kg respectively, using a stadiometer and a scale. BMI [body weight (kilograms)/height2 (meters)] was calculated using body height and body weight. BMI values were then used to identify the age and gender specific weight percentile for each child.15
Percent body fat (%BF) was obtained from a foot-to-foot bioelectrical impedance assessment using a scale. Waist circumference (WC) measurements to the nearest 0.5 cm were taken with a spring-gauge loaded, non-elastic flexible measuring tape at a point midway between the participant's last rib of the rib cage to the top of the iliac crest at the end of a normal expiration. Two WC measurements were taken and the average of both measurements was entered into the final analysis.
To assess changes in frequency, duration, and intensity of physical activity during the BOUNCE intervention, accelerometers were used. For the proposed study, protocols developed by Puyau et al., 200416 were followed. The accelerometer was programmed to collect data in 60-second epochs Monday thru Fridays from 9:00 AM until 5:00 PM each week of Interventions A and B. Participants did not wear accelerometers after 5:00 PM. Upon completion of each five-day intervention week, accelerometer data (activity counts per minute) were downloaded into the program and exported to a spreadsheet for initial analysis. In the initial examination, data completeness was verified against an exercise log and attendance roster. After initial data screening, activity counts were summed for each day and activity. Activity counts per minute were partitioned as moderate-vigorous (MVPA: ≥ 1500 counts⋅min-1), light (LPA: >100 – <1500 c⋅m-1), and sedentary activity (SA: ≤100 c⋅m-1) intensities using cutoff points developed by Puyau et al.16
Statistical analysis
Descriptive statistics, including means and standard deviations, were performed to identify basic characteristics of the data and sample population. Assumptions of normality, homogeneity, linearity, and multi-collinearity were checked and met. A repeated measures analysis of variance was used to determine changes in the average daily minutes of MVPA for each successive week followed by a paired samples t-test to determine statistically significant differences across weeks. Differences between Intervention A and Intervention B with regards to each of the adiposity indicators (BMI, %BF, and WC) at pre- and post- intervention time points were tested using a repeated measures multivariate analysis of variance (RMANOVA). Alpha levels were set at 0.05. A power analysis was conducted to determine if the sample size was adequate to detect differences in the impact of interventions on physical activity levels and adiposity indicators. The results of the power analysis indicated that a minimum of 50 and 52 subjects were required in the RMANOVA to achieve a statistical power of 0.80.
Results
Characteristics of the study sample
The baseline sample consisted of 75 (45 Latina and 30 AA) girls. Of those initial 75, 13 participants were excluded from the final sample due to missing pre- and post-physical activity or adiposity data. Thus, the final sample was reduced to 62 participants (39 Hispanic and 23 AA). As shown in table I, the mean age of 62 girls was 11.2 years + 1.5 years. Most of the participants were classified as obese (BMI ≥ 95th percentile). No significant difference in obesity status was observed between participants in Interventions A and B (p= 0.152). Thirty girls participated in Intervention A and 32 participated in Intervention B. The average attendance of the girls in Intervention A was 92% and 87% in Intervention B. Reasons for the participants' absences during intervention included family vacation, sickness, or transportation problems. The majority of the participants (90%) were low-income.
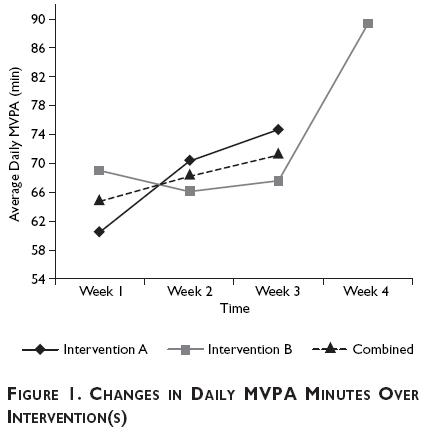
Physical activity compliance
As shown in figure 1, the average daily minutes of MVPA for Intervention A and B was similar (68.5 min and 67.5 minutes respectively). The combined MVPA improved each week. The repeated measures ANOVA indicated a significant time effect in daily MVPA (p= 0.020). The polynomial contrasts indicated that there was a significant linear effect (p= 0.005). A paired samples t-test indicated that there was only one significant daily minutes change between week 1 and week 3. These findings indicate that longer intervention duration results in a greater increase in daily MVPA.
Effects of exercise dosages on adiposity indices
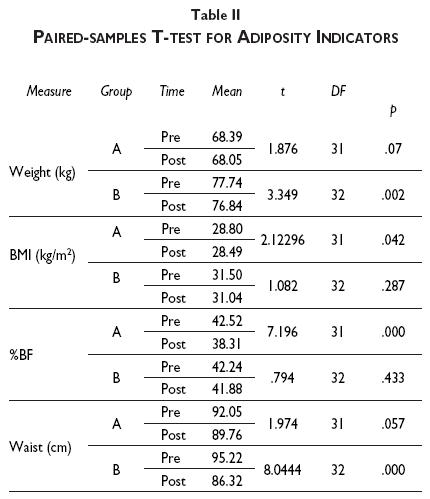
A repeated measures ANOVA was conducted to assess the differences in adiposity indicators between Intervention A and B from pre- to post-intervention periods. There was no significant effect of groups (Intervention A and B) on adiposity indicators (p= 0.069). However, there was a significant interaction effect of groups (Intervention A and B) over time (p= 0.006) on adiposity indicators. When looking more specifically at the interaction effect between time and group on the adiposity indicators, Intervention B group exhibited a significantly greater decrease in weight (p= 0.002) and WC (p = 0.001) as compared to Intervention A group. However, Group A exhibited a significantly greater decrease in BMI and %BF as compared to Group B. Table II depicts results of the paired-samples t-test of all adiposity indicators at pre- and post-intervention. The mean WC for Intervention B was also significantly lower at post-intervention (86.32 cm) than at pre-intervention (95.22 cm). However, Intervention A was more effective in reducing BMI (p <.05) and %BF (p<.001) at post-intervention.
Discussion
The purpose of this study was to assess the effects of two dosages of exercise interventions on reducing adiposity indicators in minority overweight/obese girls. Our findings indicated there was a significant effect of the interventions on WC over time and there were trends in the right direction on the reduction of %BF and BMI. Girls in Intervention B had a greater decrease of WC than girls in Intervention A. A decrease in WC is important given that recent research has shown that WC is a better determinant of cardiovascular disease than BMI17,18 and is associated with metabolic syndrome,19 type 2 diabetes, hypertension, lower HDL, and high cholesterol.20 Furthermore, WC has also been associated with abdominal fat. Kim and Lee21 identified the need for examining the impact of physical activity in decreasing abdominal obesity. Studies have demonstrated the positive effects physical activity has on abdominal obesity.22-24 Research has also reported that engaging in aerobic exercise attenuates age-related increases in visceral fat in children and adolescents.25-27 However, to our knowledge, there is no study that has examined the relationship between physical activity and abdominal obesity in Hispanic and AA girls. Thus, results from this study begin to fill the gap in our knowledge regarding the role of physical activity in reducing abdominal obesity in overweight minority girls.
A unique feature of the BOUNCE interventions is its implementation during the summer time. Research suggests that the summer time may be a period of increased weight gain and inactivity for children as compared to the school year. This weight gain can be as much as 2.8% of ideal body weight28 and African-American and Hispanics children are at an increased risk for weight gain during the summer season.29 The average BMI escalation is more than twice as fast during the summer months as it is for the school year.30 Thus, despite limited changes in BMI in Intervention B in this study, the stabilization and/or positive trends in BMI reduction that were observed helped combat the expected summer weight gain. Therefore, weight stability as well as the increased MVPA achieved during the BOUNCE summer interventions should be viewed as encouraging. Results from this study also suggest the need for greater exposure to opportunities promoting engagement in physical activity during the academic school year to achieve recommended MVPA. Furthermore, while the BOUNCE interventions may be optimal alternatives to improve daily MVPA levels in minority girls, these types of interventions might not be feasible during the academic year, but they may have an impact the level of engagement in more physical activities after the interventions. Future studies should follow up with the girls participating in the BOUNCE program to address this issue.
Several limitations of this study are noteworthy, including a lack of a control or comparison group, which may present some potential problems in controlling for extraneous variables that can reduce the internal validity. While the inclusion of a control condition is commonly a preferable research design, we employed a one-group pretest post-test design due to the exploratory nature of this study and constrained resources. Another limitation is the lack of control for sexual-maturity and developmental stages, dietary intake, and physical activity levels outside of the BOUNCE intervention, which may play a key role in adiposity levels. Use of a 1-minute epoch is another limitation of this study. When the study was initiated, this was the recommended methodology; however, more recent studies suggest using 30-second epochs for children and adolescents due to their short activity bouts. Measurement errors are always of concern and should be taken into consideration particularly with the measurement of the adiposity indicators, such as WC. To address potential measurement issues in this study, special attention was given to train our research assistants in collecting adiposity indicators data, including WC. For instance, two measurements were taken and the average of both measurements was entered into the final analysis.
Although changes in adiposity indicators over time were observed during the BOUNCE summer program, future research is needed to assess the effect of physical activity interventions on health outcomes in minority populations using stronger research designs and a larger sample size. Despite the limitations, this is an exploratory study that provides valuable information regarding different exercise dosages and their effects on decreasing WC. Constant exposure to physical activity can lead to an increase in MVPA levels among overweight minority girls. By achieving the recommended 60 minutes of MVPA each day, overweight minority girls can reduce their WC despite not losing weight or reducing BMI. The reduction of WC has a major impact on decreasing risk factors, including high blood pressure, cardiovascular disease, and type II diabetes.
Acknowledgments
We are thankful to the mothers and girls for their participation and insightful feedback regarding the BOUNCE intervention. Additionally, we acknowledge the assistance of the school administrators and physical education teachers at the selected elementary schools in the recruitment of families. Finally, we would like to acknowledge Nathalie Folch, MD. MPH for consulting in the development and implementation of the BOUNCE program and for translation of the abstract for this manuscript.
References
1. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA 2010; 303(3):242-249. [ Links ]
2. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009–2010. NCHS data brief, no 82. Hyattsville, MD: National Center for Health Statistics, 2012. [ Links ]
3. Freedman DS, Khan LK, Serdula MK, Ogden CL, Dietz WH. Racial and ethnic differences in secular trends for childhood BMI, weight, and height. Obesity (Silver Spring) 2006; 14(2):301-308. [ Links ]
4. Singh GK, Kogan MD, Van Dyck PC, Siahpush M. Racial/ethnic, socioeconomic, and behavioral determinants of childhood and adolescent obesity in the United States: analyzing independent and joint associations. Ann Epidemiol 2008; 18(9):682-695. [ Links ]
5. Anderson SE, Economos CD, Must A. Active play and screen time in US children aged 4 to 11 years in relation to sociodemographic and weight status characteristics: a nationally representative cross-sectional analysis. BMC Public Health 2008; 8:366. [ Links ]
6. Bukara-Radujkovic G, Zdravkovic D. Physical activity as an important determinant in developing childhood obesity. Med Pregled 2009;62(3-4):107-113. [ Links ]
7. US Department of Health and Human Services. 2008 Physical activity guidelines for Americans. [Consulted 2009 February]. Available in: http://www.health.gov/paguidelines. [ Links ]
8. Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 2008;40(1):181-188. [ Links ]
9. Heitzler CD, Martin SL, Duke J, Huhman M. Correlates of physical activity in a national sample of children aged 9-13 years. Prev Med 2006; 42(4):254-260. [ Links ]
10. Butte NF, Puyau MR, Adolph AL, Vohra FA, Zakeri I. Physical activity in nonoverweight and overweight Hispanic children and adolescents. Med Sci Sports Exerc 2007; 39(8):1257-1266. [ Links ]
11. van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. Br J Sports Med 2008; 42(8):653-657. [ Links ]
12. Trost SG. Interventions to promote physical activity in young children. Encyclopedia on Early Childhood Development 2011; 1-6. [ Links ]
13. Ridley K, Ainsworth BE, Olds TS. Development of a compendium of energy expenditures for youth. Int J Behav Nutr Phys Act 2008; 5:45. [ Links ]
14. Bandura A. Social foundations of thought and action: A social cognitive theory. Prentice-Hall series in social learning theory. Englewood Cliffs, NJ, US: Prentice-Hall, 1986:617.
15. Centers for Disease Control and Prevention. About BMI for Children and Teens. [Consulted 2010 June]. Available in: http://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html. [ Links ]
16. Puyau MR, Adolph AL, Vohra FA, Zakeri, Butte NF. Prediction of activity energy expenditure using accelerometers in children. Med Sci Sports Med 2004; 36:1625-1631. [ Links ]
17. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364(9438):937-952. [ Links ]
18. Cruz ML, Weigensberg MJ, Huang TT, Ball G, Shaibi GQ, Goran MI. The metabolic syndrome in overweight Hispanic youth and the role of insulin sensitivity. J Clin Endocrinol Metab 2004; 89:108-113. [ Links ]
19. Weiss R, Dziura J, Burget TS, Tamborlane WV, Taksali SE, Yeckel CW, et al. Obesity and the metabolic syndrome in children and adolescents. N Engl J Med 2004; 350:2362-2374. [ Links ]
20. Janssen I, Katzmarzyk PT, Ross R. Body mass index, waist circumference and health risk. Arch Inter Med 2002; 162:2074-2079. [ Links ]
21. Kim Y, Lee S. Physical activity and abdominal obesity in youth. Appl Physiol Nutr Metab 2009; 34(4):571-581. [ Links ]
22. Dencker M, Thorsson O, Karlsson MK, Lindén C, Wollmer P, Andersen LB. Daily physical activity related to aerobic fitness and body fat in an urban sample of children. Scand J Med Sci Sports 2008; 18(6):728-735. [ Links ]
23. Saelens BE, Seeley RJ, van Schaick K, Donnelly LF, O'Brien KJ. Visceral abdominal fat is correlated with whole-body fat and physical activity among 8-y-old children at risk of obesity. Am J Clin Nutr 2007; 85(1):46-53. [ Links ]
24. Owens S, Gutin B, Allison J, Riggs S, Ferguson M, Litaker M, et al. Effect of physical training on total and visceral fat in obese children. Med Sci Sports Exerc 1999; 31(1):143-148. [ Links ]
25. Eliakim A, Makowski GS, Brasel JA, Cooper DM. Adiposity, lipid levels, and brief endurance training in nonobese adolescent males. Int J Sports Med 2000; 21(5):332-337. [ Links ]
26. Gutin B, Barbeau P, Owens S, Lemmon C, Bauman M, Allison J, et al. Effects of exercise intensity on cardiovascular fitness, total body composition, and visceral adiposity of obese adolescents. Am Clin Nutr 2002; 75(5):818-826. [ Links ]
27. Barbeau P, Johnson MH, Howe CA, Allison J, Davis CL, Gutin B. Ten months of exercise improves general and visceral adiposity, bone, and fitness in black girls. Obesity (Silver Spring) 2007; 15(8):2077-2085. [ Links ]
28. Gillis L, McDowell M, Bar-Or O. Relationship between summer vacation weight gain and lack of success in a pediatric weight control program. Eat Behav 2005; 6:137-143. [ Links ]
29. Downey DB, Boughton HR. Childhood body mass index gain during the summer versus during the school year. New Dir Youth Dev 2007; 114:33-43. [ Links ]
30. von Hippel PT, Powell B, Downey DB, Rowland NJ. The effect of school on overweight in childhood: gain in body mass index during the school year and during summer vacation. Am J Public Health 2007; 97(4):696-702. [ Links ]
Received on: March 14, 2012
Accepted on: April 15, 2013
 Corresponding author:
Corresponding author:
Stephanie Kellam.
Health Program, College of Education, University of Houston. 4800 Calhoun Rd, Houston Tx, 77204, USA.
E-mail: stkellam@gmail.com
Declaración de conflicto de intereses: Los autores declararon no tener conflicto de intereses.
