










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.54 supl.1 Cuernavaca ene. 2012
ANNEX
Sociodemographic characteristics of SMNG affiliates
Elaborado por: Mirna Hebrero-MartínezI; Rita Velázquez LermaII; Clara Mantilla TrolléIII; Ricardo Pérez-CuevasI, IV; Onofre MuñozV
ICentro de Estudios Económicos y Sociales en Salud, Hospital Infantil de México Federico Gómez. México, DF, México
IIDirección de Estandarización de Clasificaciones y Contenidos Sociodemográficos. Instituto Nacional de Estadística y Geografía. México, DF, México
IIIDirección de Encuestas Especiales. Instituto Nacional de Estadística y Geografía. Aguascalientes, México
IVUnidad de Investigación Epidemiológica y Servicios de Salud Siglo XXI, Instituto Mexicano del Seguro Social. México
VDirección de Investigación. Hospital Infantil de México Federico Gómez. México DF, México
Methodology
The survey of the Medical Insurance for a New Generation 2009 (Encuesta del Seguro Médico para una Nueva Generación, ESMNG 2009) was conducted from March 16th to April 10th 2009. The National Institute of Statistics and Geography (Instituto Nacional de Estadística y Geografía, INEGI) was in charge of the design and collection of the information. The survey was designed to have national representation; urban having 2500 or more inhabitants (>=2500) and rural having less than 2500 inhabitants (<2500). The sample had a design that was probabilistic, with three stages, and by clusters; the selection was proportionally distributed in each state of Mexico according to the size of the target population. The sampling units were municipalities, localities, and beneficiaries. The sampling frame was made up of 1545717 children affiliated between December 1st 2006 and September 30th 2008. The sample size was calculated with a 90% confidence interval, a 3.45 design effect, a 15% maximum relative expected error, a 30% maximum expected non-response rate, and a 4% proportion. The sample size was estimated on 12240 children. Also, a subsample of affiliates with anthropometric measurements of 6240 children, and another of hemoglobin measurements of 760 children was included.
The questionnaire includes 13 sections‡ and the information was collected through several direct interviews with an electronic questionnaire operated by a mobile device (mini laptop). The mother or primary caretaker of the child was the respondent of the interview. The detailed description of the interview is in the Methodological Synthesis of the ESMNG 20091 and in an article of this series.2
The measurements employed in this article are proportions and double entry contingency tables with Chi squared tests to identify possible significant differences by type of locality, with p<0.01 significance levels, and, in some cases, average values and correlation analysis were also calculated.
The results of the descriptive analysis were calculated using the expansion factor that allows for representation at the national level and by urban-rural locality type. The calculation of the expansion factors is found in the methodological synthesis of the ESMNG 2009. The analysis was carried out with SPSS 18 software.
Results
Information of 9085 live children, 6 to 29 months of age was analyzed; 24% were <1 year, 57.3% were 1, and 17.9% were 2; 49% were women and 28% lived in urban localities.
Information was also collected on 74 deceased affiliates, 33 in urban areas and 41 in rural areas. As much as 93% died before reaching one year of age, and 63% during the first month of life.
Mothers' characteristics
Mothers' mean age was 26.1 years; most were between 20 and 34 years of age. In urban localities, there was a greater proportion of adolescent mothers (<20 years) and in rural localities there was a greater proportion of mothers who were over 35. Mothers on average had 2.3 live births (rural localities 2.7 and urban localities 2.2). One out of four rural mothers was illiterate or had not finished primary school; the urban settings had a greater proportion of mothers with secondary and preparatory schooling levels (rural 48.9%, urban 68.8%). The majority (64.8%) were homemakers; one out of three reported having a job or economic activity with or without salary. Half of the women who worked were skilled workers and 38.4% were self-employed (table I).
Family structure and household characteristics
On average, there were 5.1 persons in the household* of the affiliates (rural 5.3 and urban 5). A male-headed household prevailed, although in urban areas there was a greater proportion of female-headed households (17%) when compared to the rural areas (10.1%). Among the persons that were reported as being the head of the household, 67.7% were a father and 6.7% a mother of an affiliated child; 81% of the female-headed households coincided with the father's absence in the home, which represented 20.4%. Most households were nuclear (mother, father, and children), and one out of three households was extensive, and in most of these only the mother was present.
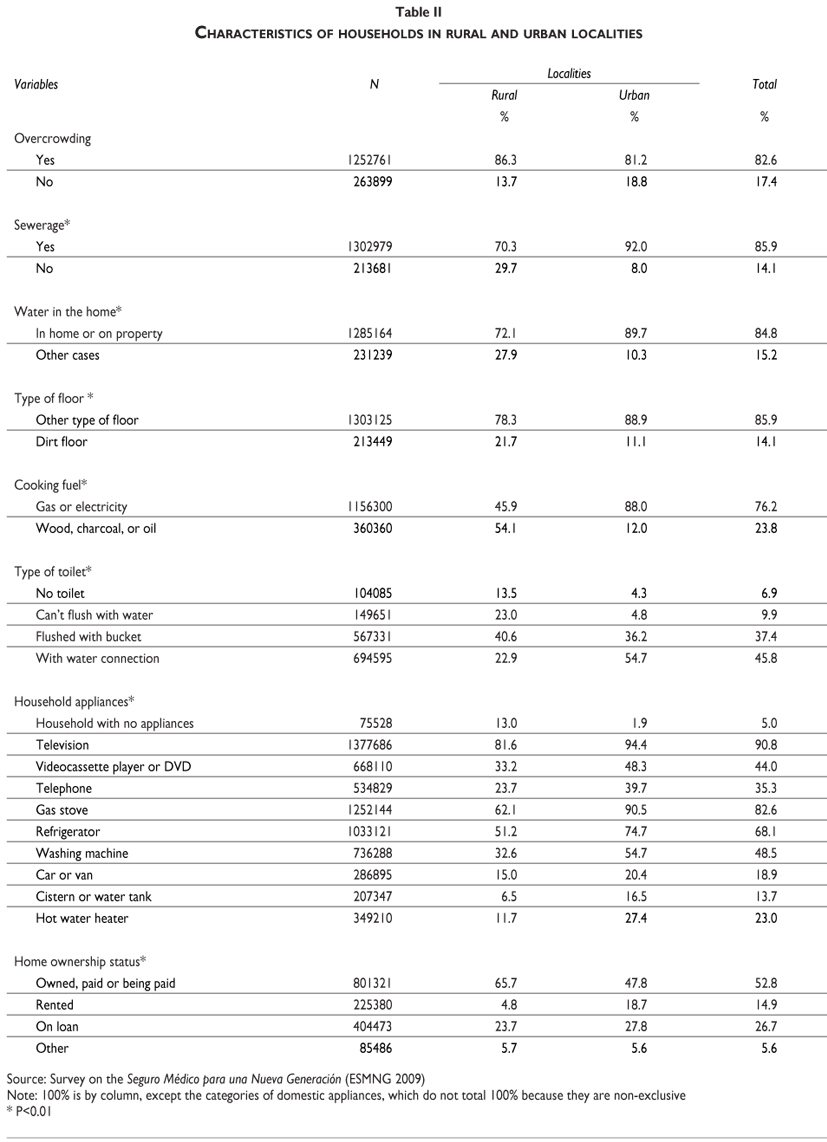
Considering the program's eligibility criteria, it is noticeable that at a national level, 9.7% of parents reported being affiliated to at least one social security institution. In urban localities was 11.8%, and in rural localities 4.1% (table II).
Dwelling characteristics
Overcrowding was widespread in this population (80%). Three out of ten dwellings did not have a toilet, and the majority of those that did have it couldn't flush it with water and had to do it with a bucket.
Rural areas had a lower availability of sewage or drainage system and of running water in the dwelling; half of these dwellings cooked with firewood, charcoal or oil, and one out of five had dirt floors.
About half of the dwellings of the affiliates were rented or loaned; the latter was more common in rural localities. The data on household appliances shows that 5% of the dwellings reported having no appliances; in urban localities it was 13% (table II).
SMNG affiliation, use and satisfaction of health services
The mother's knowledge of her child's affiliation to the System of Social Protection in Health (Sistema de Protección Social en Salud, SPSS) had two criteria: the exclusive affiliation to SMNG and/or to Seguro Popular, where one out of two mothers reported exclusive affiliation to SMNG, 13% inscription to both SMNG and Seguro Popular, one out of three were only aware of the inscription to the Seguro Popular, and 8% reported having no knowledge of the child's affiliation.
Of the people surveyed who declared having knowledge of the affiliation to SMNG (52%), one out of four reported not having used the services because: they hadn't needed to, they preferred to take their child to another service or they didn't know how it worked. The majority of those who reported they had used the services also reported that it took them at least an hour to arrive to the place where medical services were offered, 47% mentioned that they spent up to Mx$49, mostly in urban areas, and around 10% spent more than Mx$50 pesos in transportation to arrive to the place where they seeked medical attention.
The most commonly reported waiting time to receive care was 2 hours, and this occurred in a greater proportion in rural areas. The majority declared that in their last consultation the way they were treated by the physician was good, but two out of ten reported it was from so-so to very bad; around 18% mentioned that the physician did not inform them what the child's illness consisted in, and around three out of then reported the last consultation being so-so to completely unsatisfactory, the greater proportion of them being urban population. In this regard, a statistically significant positive correlation was found between general satisfaction and the way they were treated by the physician in their last consultation (table III).
Acknowledgements
We would like to thank the National Institute of Statistics and Geography, (Instituto Nacional de Estadística y Geografía, INEGI), for their contribution in the design and for conducting of the national survey to evaluate the impact on health state and family's finances of SMNG affiliated children. We would like to specially acknowledge Eduardo León Ríos Mingramm (Assistant Director General of Sociodemographic Surveys and Administrative Registries of INEGI). We would also like to thank Evelyne Rodríguez Ortega (Head of Department of Policy Research of HIMFG) who actively participated during the evaluation's preparation and design, for her comments and contributions.
Declaration of conflict of interests: The authors declare not to have conflict of interests.
References
1. Instituto Nacional de Geografía e Informática y Hospital Infantil de México Federico Gómez. Encuesta sobre el Seguro Médico de Nueva Generación: Síntesis Metodológica. México 2009. [Accessed 2011 June 5]. Available at: http://www.inegi.gob.mx/est/contenidos/espanol/metodologias/encuestas/hogares/sm_ESMNG.pdf. [ Links ]
2. Pérez-Cuevas R, Muñoz O, Rodríguez E, Jasso L, Flores S, Durán L, Pasillas M, Garduño J, Cortes-Gallo G. Design of the 2009 Evaluation of the Medical Insurance for a New Generation Program. Salud Publica Mex 2012:S11-S19. [ Links ]
‡ Sections: Characteristics of the dwelling and home identification, Sociodemographic characteristics, Reproductive and maternal and child health, Data on the birth of the child, Breastfeeding and nutrition, Enrollment in SMNG, Health service use and satisfaction, Use of preventative medical services and vaccination, Diseases and accidents, Attendance to workshops and talks about health self-care, Expenditure in child's health, Total home expenditure and income, and Information about deceased children.
* The concept of household is used as the group of people that live in the same dwelling and share the same eating expenses; hence, it does not necessarily correspond to the family affiliated to the System of Social Protection in Health (SPSS).


{kind=link}
{kind=link}
{kind=link}