










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.54 no.2 Cuernavaca mar./abr. 2012
ORIGINAL ARTICLES
Overview of the nutritional status of selected micronutrients in Mexican children in 2006
Estado nutricional de algunos micronutrientes en niños mexicanos en 2006
Teresa Shamah-Levy, MSc; Salvador Villalpando, MD PhD; Alejandra Jáuregui, MSc; Juan A Rivera, MS, PhD
Centro de Investigación en Nutrición y Salud, Instituto Nacional de Salud Pública. Cuernavaca, México
ABSTRACT
OBJETIVE: To present an overview of micronutrient status of Mexican children in 2006.
MATERIALS AND METHODS: Data on iron, zinc, folate and vitamin B12 deficiencies and low serum copper and magnesium were gathered and critically analyzed from the 2006 National Health and Nutrition Survey.
RESULTS: Iron deficiency is still the main nutritional deficiency in children (13%-26%). Zinc deficiency was high in all age groups (≈25%) but reduced 5.6 PP in children <5 y from 1999 to 2006. Folate deficiency was 3.2% and vitamin B12 deficiency 7.7% in children. Low serum magnesium and copper were high (22.6% and 30.6%, respectively).
CONCLUSIONS: The prevalence of iron deficiency seems to be lowering, and zinc deficiency has reduced in Mexican children. A high prevalence of copper and magnesium deficiencies warrants further research on their public health implications.
Keywords: iron; folate; zinc; copper; magnesium; micronutrient status; Mexico
RESUMEN
OBJETIVO: Presentar un panorama del estado de micronutrimentos de niños mexicanos en 2006.
MATERIAL Y MÉTODOS: Los datos sobre deficiencias de hierro, zinc, folatos, vitamina B12 y concentraciones bajas de cobre y magnesio se analizaron a partir de la Encuesta Nacional de Salud y Nutrición 2006.
RESULTADOS: La deficiencia de hierro fue la más importante en niños (13-26%). La deficiencia de zinc fue alta en todos los grupos de edad (≈25%) y disminuyó entre 1999 y 2006 5.6 pp en niños. La deficiencia de folatos fue de 3.2% y la de vitamina B12 de 7.7%. Las concentraciones bajas de magnesio y cobre fueron altas (22.6 y 30.6%, respectivamente).
CONCLUSIONES: La deficiencia de hierro pareció disminuir y la de zinc se redujo en niños mexicanos. La alta prevalencia de deficiencias de cobre y magnesio merecen más investigación para entender sus implicaciones en salud pública.
Palabras clave: hierro; folatos; zinc; cobre; magnesio; estado de micronutrimentos; México
Micronutrient deficiencies are still an important public health problem globally.1 In Mexico, the first comprehensive picture of the frequency and distribution of micronutrient deficiencies was presented by the Mexican National Nutrition Survey of 1999 (Encuesta Nacional de Nutrición 1999, ENN99).2 In ENN 99 anemia and iron deficiency were the most frequent nutritional deficiencies, particularly in infants 12 to 24 months of age (59 and 67%, respectively). Zinc deficiency was the second most common micronutrient deficiency: 34% in infants <2 years of age, and 19-24% in school-age children. Iodine deficiency was negligible in children.3 The ENN 99 also showed that vitamin A subclinical deficiency (<20 ug/dl) was present in 25% of children. About 30% of children <2 y had low (<0.3 mg/dl) ascorbic acid serum concentrations. The prevalence of folate deficiency varied in children from 2.3 to 11.2%.4
In 2006 a new national nutrition survey was carried out: the National Health and Nutrition Survey (Encuesta Nacional de Salud y Nutrición 2006, ENSANUT 2006).5 Blood samples were obtained for analysis of micronutrient status and stored while funds were obtained for laboratory analyses.
This paper presents an overview of the micronutrient status of Mexican children and adolescents in 2006, addresses the determinant factors of the different micronutrient deficiencies presented in related articles in this issue of Salud Pública de México (SPM) and highlights the most relevant findings. It also discusses differences in the micronutrient status indicators measured in 1999 and 2006 which were comparable. The results and conclusion of the paper can be used as input for designing public policies and as a reliable source of information for the health and academic community.
Materials and methods
Data sources
The source of information for this analysis is the National Health and Nutrition Survey (ENSANUT 2006).5 Conducted by the Mexican National Institute of Public Health in 2006 the survey and the subsample in which micronutrient status was determined was representative at the national level and at the following geographical regions: North, Center, Mexico City and South as well as by rural (<2500 inhabitants) and urban localities (≥ 2500 inhabitants). Detailed description of the design and sampling procedures for ENSANUT 2006 has been published elsewhere.5,6
Data collection and analysis
Data collection methods for assessing micronutrient status in children 1-11 y (n=5 060) and adolescents 12-19 y (n=2 418) are presented in detail in several articles in this issue for microminerals7,9 and vitamins.8 The present analysis is based on the information furnished by those articles.
The protocol of the survey was approved by the Research, Ethics and Biosecurity Committees of the National Institute of Public Health, Cuernavaca, Mexico.
Definition of micronutrient status
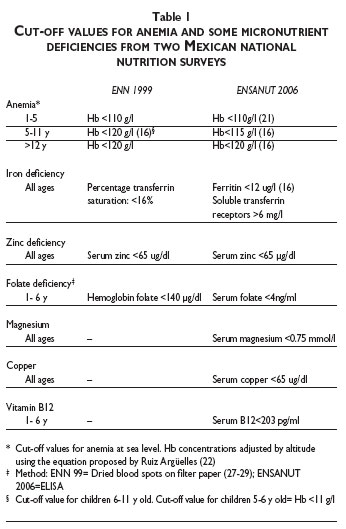
Table I presents the indicators of micronutrients status and the cut off values defining the deficiencies (or low serum concentrations) of individual micronutrients used in 2006. It also presents the methods used in 1999 to show that methods of assessment or cut-off points used to determine all micronutrients status differed between surveys, precluding comparisons. Only anemia and zinc were determined using the same method and cut-off values in both surveys.
Statistical analysis
Statistical analyses are described in detail in articles in this issue.7,8,9 Several of the analyses are presented and discussed in the context of geographic region and/or rural and urban areas (as previously described), age group, and SES classification. Data were analyzed with Stata 9.2 package.
Results
Results are presented for 5 060 children 1-11 y and 2 418 adolescents 12-19 y.
Iron deficiency
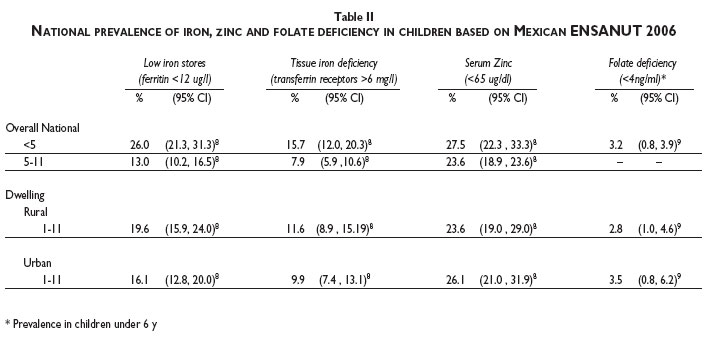
The prevalence of iron deficiency, as assessed by serum concentrations of soluble transferrin receptors (sTfR >6 mg/l), was 15.7% in children <5 y and 7.9% in children aged 5-11 y. No differences were noted between urban and rural areas. The prevalence, as assessed by serum ferritin <12 ug/l, was 26.0% in children <5 y and 13.0% in children 5-11 y. Prevalence in children 1-11 y was higher in rural areas (table II).
Zinc deficiency
The prevalence of zinc deficiency in 2006 as assessed by serum zinc <65 µg/dl10 was 27.5% in children under 5 y and 23.6% in 5-11 y old children (table II).
The prevalence of low serum zinc levels back in the 1999 National Nutrition Survey was 33.1% in children under 5 years of age.3 Reductions of 5.6 percentage points (PP) were observed from 1999 to 2006.
Folate deficiency
The prevalence of folate deficiency as assessed by serum folate<4 ng/ml was 3.2% in children 1-5 y. Determinations were not made in older children. The prevalence was slightly higher in urban than in rural areas (table II).
Nutritional status of other micronutrients
This issue of SPM reports for the first time the nutritional status of magnesium, copper, and vitamin B12 in a probabilistic, population based sample in Mexican children and adolescents.7,9 The prevalence of low magnesium serum concentrations (<0.75 mmol/l) was 22.6% in children 1-11 y and 37% in adolescents (12-19 y). Prevalence was higher in urban areas in children 1-11y (25.8%) compared to rural areas (18.6%) and were similar in adolescents.
Prevalence of low copper serum concentrations (<65 ug/dl) was 30.6% in children 1-11 y and 14.1% in adolescents. Prevalences in children and adolescents were similar in urban and rural areas (table III). One of the papers in this issue analyzed the prevalence of low copper serum concentrations by ethnic background (indigenous vs. non-indigenous) in adolescents,9 finding that the prevalence in non-indigenous population was about twice the prevalence in indigenous children (table III).
Prevalence of vitamin B12 deficiency (serum B12<203 pg/ml) was 7.7% in children 1-5 y. Prevalence was higher in rural compared to urban areas (table III).
Causes of anemia in children <5 y of age
The prevalence of anemia in children and adult population in 1999 and 2006 were thoroughly analyzed in two recent publications,11,12 thus this section will be limited to the analysis of the causes of anemia in children <5 years of age. In 2006, the proportion of cases of anemia documenting iron deficiency irrespectively of the presence or absence of other deficiencies was 42%. The proportion of cases of anemia associated with iron deficiency combined with deficiencies of folate and/or vitamin B12 was 10.3%. The proportion of cases of anemia associated with deficiencies of folate or vitamin B12 without iron deficiency was 2.0%. The proportion of cases of anemia of non-identified nutritional cause was 45% (table IV). It is important to underline that serum concentrations of vitamin A were not determined in the 2006 survey.

Discussion
Iron deficiency in children seems to have diminished from 1999 to 2006. However, it is necessary to underline the lack of comparability between the two prevalences, because in 1999 iron deficiency was measured using as indicator the percent transferrin saturation, which has a lower sensitivity and specificity than the serum ferritin concentrations used in 2006.13 Nevertheless the magnitude of the change is so large (≈ 30 PP), that the notion that a significant reduction occurred is plausible. Factors contributing to such an improvement in groups at higher risk for iron deficiency are, among others, the social programs distributing iron fortified foods or food supplements to young children and pregnant and lactating women (Oportunidades and Liconsa). In support to such a notion, Morales et al.7 and De la Cruz et al.9 found a significant protective association between the affiliation to both programs and the risk to suffer iron deficiency in children and adolescents. In the same line, there was a reduction in the prevalence of anemia from 1999 to 2006 of near 15 PP in children 12-24 months of age12 and 5% in non pregnant and pregnant women.11
A remarkable finding is the reduction (about 20%)in the prevalence of zinc deficiency in children <5 y from 1999 to 2006. Public programs supplying children and pregnant and lactating women with fortified food and supplements containing zinc, among other micronutrients, serve almost 5 million beneficiaries (Liconsa) and more than 5 million families (Oportunidades). Therefore, it is likely that these programs have contributed to improve the zinc status of those age segments. The efficacy of the supplement distributed by Oportunidades was tested in urban children younger than 3 years, finding that it was as effective as the powdered micronutrients preparation known as "sprinkles" to reduce the prevalence of zinc deficiency (from 10 to 30 PP) after 4 months of consumption.14 In spite of such a reduction, the prevalence of zinc deficiency persists at high level. This may be explained in part by the high dietary intake of inhibitors of intestinal absorption of dietary zinc, such as phytates, calcium, and fiber. The molar ratio phytate to zinc in the Mexican diet is about 6:1.15,16 Therefore, it is mandatory to carry out studies focused on the effectiveness of the micronutrient fortified foods or supplements provided by the public food assistance programs to reduce the prevalence of zinc deficiency.
The prevalence of folate deficiency in children under 5 y falls in the category of minimal public health problem as by the WHO criteria.17 The role of folate as a cause of anemia in the ENSANUT 2006, reported in a companion paper,9 was quite small; supporting the notion that folate deficiency is marginal as a public health problem in Mexico. This finding applies to children under 5 years and does not mean that folate supplementation or fortification around the time of conception to reduce the risk of congenital neural tube defects (NTDs) should be discontinued. NTDs risk factors include genetic as well as environmental factors, particularly folic acid deficiency at the time of conception. There is clear evidence of the effectiveness of folic acid supplementation or fortification in the prevention of NTDs across a large range of population folate intakes.18
Copper and magnesium deficiencies are new players in the nutritional scene of Mexico and its meaning is not quite understood. The high prevalence of copper deficiency was not associated with an insufficient intake7,8,9 allowing us to speculate that its absorption, as in the cases of iron and zinc, is interfered by a high intake of antagonists of its absorption, abundant in the Mexican diet.19 Copper deficiency in this study had a high level of association with the prevalence of iron deficiency anemia.9 As a constituent of ferroxidase, copper deficiency may interfere with the oxidation of Fe+2 to Fe+3, form in which iron is absorbed and captured by the ferritin molecule. Also, copper competes with zinc for the binding sites on metallothionein, which have more binding affinity for the former.20
Low serum magnesium might be very relevant for the epidemiological and health status of the Mexican population, because it has been associated with glucose intolerance and higher risks for atherosclerosis, hypertension and myocardial infarction.21-23 More research is needed in order to explore the consequences of magnesium deficiency in the health of Mexican population.
Anemia in Mexican children younger than 5 y was associated with iron deficiency in less than half of the cases analyzed in the two surveys, 199924 and 2006, highlighting the causal importance of other micronutrient deficiencies. In conclusion the prevalence of iron deficiency, although still high, seems to be progressively lowering in children. The prevalence of zinc deficiency in children < 5 y had some improvements that may be associated, in part, with public and focalized nutrition interventions aiming to curb it. The high prevalence of copper and magnesium deficiencies warrant further research to better understand their implications for public health. These results provide relevant information to reinforce some of the ongoing nutrition policies and to redesign others, particularly referring to zinc, copper and magnesium deficiencies.
References
1. Ramakrishnan U. Prevalence of micronutrient malnutrition worldwide. Nutr Rev 2002;60:S46-S52. [ Links ]
2. Rivera-Dommarco J, Shamah-Levy T, Villalpando-Hernández S, González-de Cossío T, Hernández-Prado B, Sepúlveda J. Encuesta Nacional de Nutrición 1999. Estado nutricio de niños y mujeres en México. Cuernavaca, Morelos, México: Instituto Nacional de Salud Pública, 2001. [ Links ]
3. Villalpando S, García-Guerra A, Ramírez-Silva CI, Mejía-Rodríguez F, Matute G, Shamah-Levy T, et al. Iron, zinc and iodide status in Mexican children under 12 years and women 12-49 years of age. A probabilistic national survey. Salud Publica Mex 2003;45:S520-S529. [ Links ]
4. Villalpando S, Montalvo-Velarde I, Zambrano N, García-Guerra A, Ramírez-Silva CI, Shamah-Levy T, et al. Vitamins A, and C and folate status in Mexican children under 12 years and women 12-49 years: A probabilistic national survey. Salud Publica Mex 2003;45:S508-S519. [ Links ]
5. Olaiz-Fernández G, Rivera-Dommarco J, Shamah-Levy T, Rojas R, Villalpando-Hernández S, Hernández-Avila M, et al. Encuesta Nacional de Salud y Nutrición 2006. Cuernavaca, México: Instituto Nacional de Salud Pública, 2006. [ Links ]
6. Resano-Perez E, Mendez-Ramirez I, Shamah-Levy T, Rivera JA, Sepulveda-Amor J. Methods of the National Nutrition Survey 1999. Salud Publica Mex 2003;45 Suppl 4:S558-S564. [ Links ]
7. Morales-Ruan MC, Villalpando S, Garcia-Guerra A, Robledo-Perez R, Avila-Arcos MA, Rivera JA, et al. Iron, zinc, copper, and magnesium nutritional status in Mexican children aged 1 to 11 years. Salud Publica Mex 2012;54:125-134. [ Links ]
8. Cuevas-Nasu L, Mundo-Rosas V, Shamah-Levy T, Méndez-Gómez Humarán I, Ávila-Arcos MA, Rebollar R, et al. Prevalence of folate and vitamin B12 deficiency in Mexican children aged 1 to 6 years in a population-based survey. Salud Publica Mex. 2012;54:116-124. [ Links ]
9. De la Cruz-Góngora V, Gaona-Pineda EB, Villalpando S, Shamah-Levy T. Anemia and Iron, Zinc, Copper and Magnesium Deficiency in Mexican adolescents. Results of the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2012;54:135-145. [ Links ]
10. International Zinc Nutrition Consultative Group (IZiNCG).Technical Document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull 2004;25:S94-S203. [ Links ]
11. Shamah-Levy T, Villalpando-Hernandez S, Garcia-Guerra A, Mundo-Rosas V, Mejia-Rodriguez F, Dominguez-Islas CP. Anemia in Mexican women: results of two national probabilistic surveys. Salud Publica Mex 2009;51 Suppl 4:S515-522. [ Links ]
12. Villalpando S, Shamah-Levy T, Garcia-Guerra A, Mundo-Rosas V, Dominguez C, Mejia-Rodriguez F. The prevalence of anemia decreased in Mexican preschool and school-age children from 1999 to 2006. Salud Publica Mex 2009;51 Suppl 4:S507-S514. [ Links ]
13. Beutler E, Felitti V, Ho NJ, Gelbart T. Relationship of body iron stores to levels of serum ferritin, serum iron, unsaturated iron binding capacity and transferrin saturation in patients with iron storage disease. Acta Haematol 2002;107:145-149. [ Links ]
14. García-Guerra A, Rivera-Dommarco JA, Neufeld L, Domínguez-Islas CP. Effect of three supplements with equal micronutrient content on serum zinc concentrations in Mexican children. FASEB Journal 2009:110-121. [ Links ]
15. Krebs NF. Overview of zinc absorption and excretion in the human gastrointestinal tract. J Nutr 2000;130:1374S-1377S. [ Links ]
16. World Health Organization. Zinc. In: Vitamin and mineral requirements in human nutrition: report of a joint FAO/WHO expert consultation. Bangkok, Thailand: WHO, 2005:230-245. [ Links ]
17. McLean E, de Benoist B, Allen LH. Review of the magnitude of folate and vitamin B12 deficiencies worldwide. Food Nutr Bull 2008;29:S38-S51. [ Links ]
18. Blencowe H, Cousens S, Modell B, Lawn J. Folic acid to reduce neonatal mortality from neural tube disorders. Int J Epidemiol 2010;39 Suppl 1:i110-121. [ Links ]
19. Barquera S, Hernandez-Barrera L, Campos-Nonato I, Espinosa J, Flores M, Barriguete-J A, et al. Energy and nutrient consumption in adults: analysis of the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2009;51 Suppl 4:S562-573. [ Links ]
20. Milne DB. Copper intake and assessment of copper status. Am J Clin Nutr 1998;67:1041S-1045S. [ Links ]
21. Swaminathan R. Magnesium metabolism and its disorders. Clin Biochem Rev 2003;24:47-66. [ Links ]
22. King DE. Inflammation and elevation of C-reactive protein: does magnesium play a key role? Magnes Res 2009;22:57-59. [ Links ]
23. Barbagallo M, Dominguez LJ. Magnesium metabolism in type 2 diabetes mellitus, metabolic syndrome and insulin resistance. Arch Biochem Biophys 2007;458:40-47. [ Links ]
24. Villalpando S, Perez-Exposito AB, Shamah-Levy T, Rivera JA. Distribution of anemia associated with micronutrient deficiencies other than iron in a probabilistic sample of Mexican children. Ann Nutr Metab 2006;50:506-511. [ Links ]
 Corresponding author:
Corresponding author:
Dr. Salvador Villalpando.
Instituto Nacional de Salud Pública,
Av. Universidad 655, col. Santa María Ahuacatitlán.
62100 Cuernavaca, Morelos, México
E-mail: svillalp@insp.mx
Received on: August 31, 2011
Accepted on: October 17, 2011
Declaration of conflict of interests: The authors declare that they have no conflict of interests.


{kind=link}
{kind=link}