










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.54 no.2 Cuernavaca mar./abr. 2012
ORIGINAL ARTICLES
Anemia and iron, zinc, copper and magnesium deficiency in Mexican adolescents: National Health and Nutrition Survey 2006
Anemia y deficiencia de hierro, zinc, cobre y magnesio en adolescentes mexicanos: resultados de la ENSANUT 2006
Vanessa De la Cruz-Góngora, MsC; Berenice Gaona, MsC; Salvador Villalpando, MD, PhD; Teresa Shamah-Levy, MsC; Ricardo Robledo, PhD
Instituto Nacional de Salud Pública. Cuernavaca, Morelos, México
ABSTRACT
OBJETIVE: To describe the frequency of anemia and iron, zinc, copper and magnesium deficiencies among Mexican adolescents in the probabilistic survey ENSANUT 2006.
MATERIALS AND METHODS: The sample included 2447 adolescents aged 12 to 19 y. Capillary hemoglobin and venous blood samples were collected to measure the concentrations of ferritin, sTFR, CRP, zinc, iron, copper and magnesium. Logistic regression models were constructed to assess the risk for mineral deficiencies.
RESULTS: The overall prevalence of anemia was 11.8 and 4.6%, body iron deficiency 18.2 and 7.9% for females and males, respectively. Overall prevalence of tissue iron deficiency was 6.9%, low serum copper were14.4 and 12.25%; zinc 28.4 and 24.5%, magnesium 40 and 35.3%; for females and males, respectively.
CONCLUSIONS: There is a high prevalence of mineral deficiency in Mexican adolescents; females were more prone to have more mineral deficiencies. Nutritional interventions are necessaries in order to reduce and control them.
Keywords: iron; zinc; copper; magnesium; Mexican adolescents
RESUMEN
OBJETIVO: Describir la prevalencia de anemia y deficiencia de hierro, zinc, cobre y magnesio en adolescentes mexicanos en la encuesta probabilística ENSANUT 2006.
MATERIAL Y MÉTODOS: La muestra incluyó 2447 adolescentes de 12 a 19 años de edad. Se tomó hemoglobina capilar y muestras de sangre venosa para medir las concentraciones séricas de ferritina, sTFR, CRP, zinc, hierro, cobre y magnesio. Se construyeron modelos de regresión logística para evaluar el riesgo de deficiencia de minerales.
RESULTADOS: La prevalencia de anemia fue de 11.8% en mujeres y 4.6% en hombres. Las deficiencias de hierro fueron de 18.2 y 7.9% La deficiencia tisular de hierro fue 6.9%; la baja concentración de cobre fue de 14.4 y 12.25% la de zinc de 28.4 y 24.5%, la de magnesio fue 40 y 35.3% en mujeres y hombres, respectivamente.
CONCLUSIONES: Existe una alta prevalencia de deficiencia de minerales en los adolescentes; las mujeres tuvieron mayor riesgo. Son necesarias intervenciones nutricionales para reducir o controlar estas deficiencias.
Palabras clave: hierro; zinc; cobre; magnesio; adolescentes mexicanos
The deficiency of micronutrients is a health issue far from being resolved globally.1 Some mineral deficiencies as such iron and zinc impact negatively on physical growth, immune response, cognitive and emotional development, among others.2
There is limited information on the mineral status of copper and magnesium in adolescents. In adult German population, prevalence of magnesium deficiency reached 14.5%.3 Knovich et al reported an association between serum copper levels and anaemia in American population (NHANES II).4 Reports on the prevalence of anemia, iron and zinc deficiency are available for several groups of adolescents;5-7 varying from 2% to 5% for zinc deficiency in British, 43% in Ethiopia and over 50% in Sri Lanka population. Also were found 24% of iron deficiency in Sri Lanka. The Mexican National Nutrition Survey -1999 (NNS-99), described the prevalences of anemia, iron, zinc and iodine status in women between 12 and 49 years of age. The overall prevalence of anemia was 20.8%,8 iron deficiency was 40% and zinc deficiency 30%.9 However no distinctions were made for adolescents. No information is available for cooper and magnesium deficiencies in population-based surveys in Mexico. The objective of the present analysis is to describe the frequency and distribution of anemia and iron, zinc, copper and magnesium deficiencies among Mexican adolescents, aiming to identify opportunities for intervention.
Population and methods
Study population. Information for the present analysis was extracted from the dataset of the Mexican National Health and Nutrition Survey of 2006 (ENSANUT 2006). This is a probabilistic survey, representative at the national, regional, urban and rural levels.
A detailed description of the design and sampling procedures was published elsewhere.10 Demographic and socioeconomic information was collected using ad hoc questionnaires. Ethnicity was classified if an indigenous language was spoken. Localities with less than 2 500 inhabitants were considered as rurals. A socioeconomic index was constructed based on the household characteristics and family assets by a principal component analysis, the index was divided into tertiles being 1 the lowest. The country was divided in four geographic regions: Northern, Center, Mexico City and Southern. Anthropometric information (weight and height) was collected using validated and standardized methods.11,12 Body Mass Index (BMI) was computed based on height and weight.13
This sample (n= 2447), was extracted from the general dataset of the ENSANUT 2006 including 12-19 yrs of age with a blood sample available.
Methods for serum mineral concentrations and C reactive protein
Venous blood samples were drawn and centrifuged at 268 g, in situ. Serum was separated and stored in coded cryovials, preserved in liquid nitrogen until delivery to a central laboratory in Cuernavaca, Mexico.
The serum concentrations of ferritin, soluble transferrin receptors (sTfR) were measured by immunoassay method using commercial kits (Dade Behring Inc). C reactive protein (CRP) was measured by nephelometry, using ultra sensitive monoclonal antibodies (Behring Nephelometer 100 Analyzer).
Low iron stores (LIS) was defined if serum concentrations of ferritin <12 µg /L; tisssue iron deficiency (TID) was defined if serum concentrations of sTfR were >6 mg/L.
The total body iron (TBI) (mg/kg) was calculated based on the concentrations of sTfR and s-ferritin using the Cook's equation.14
The serum concentrations of iron, zinc, copper and magnesium were measured by inductively coupled plasma atomic emission spectroscopy using a Varian Vista Pro CCD spectrometer.
Zinc deficiency was defined if <65 µg/dL.15 Low serum copper (LSC) if <70 µg/dL for males or <80 µg /dL for females4 and low serum magnesium if <1.82 mg/dL (<0.75 mmol/L).16
Anemia
Capillary hemoglobin was measured using a portable photometer. Anemia was defined when hemoglobin concentration (Hb) adjusted by altitude was <120 g/L for females or <130g/L for males.17 Iron deficiency anemia (IDA) was defined if an anormal Hb value coexisted with at least one of the following abnormalities: s-ferritin, sTfR or serum iron. Others causes of anemia were defined when they did not meet the above criteria.
Dietary intake
Obtained using food-frequency questionnaire (FFQ) collecting information on the seven days prior to the survey, including 101 food items. The validation of the FFQ was published elsewhere.18 The intake of energy and macronutrients was computed; the intake in g/day was transformed into total energy, macro and micronutrients using the food composition tables compiled by Instituto Nacional de Salud Pública, combining the USDA Food Composition Tables, and other tables from Mexico and Latin America.18 The adequacy was referred to the Dietary Reference Intakes (DRI) of the Institute of Medicine of USA.19
Statistical analysis
The characteristics of the sample are described as frequencies and 95% confidence intervals, stratified by sex. The distribution of TBI, age and sex interactions were evaluated through multiple linear regression models. Logistic regression models were constructed to test the risks for low tissue iron, low serum zinc, copper and magnesium. Heterogeneity of effects by sex and age were tested adjusted by Socioeconomic Status (SES), BMI, CRP, dwelling, geographical regions, ethnicity and being beneficiary of Oportunidades.
Statistical significance was set at α=0.05 and α=0.1 for interactions. All analyses were adjusted for the sampling design of the survey, using STATA SE v11.
The protocol was approved by the Research, Ethics, and Biosecurity Comitee of Instituto Nacional de Salud Pública, Mexico. Individual assents and informed consent letters were obtained from the parents of all participants.
Results
This analysis includes 2 447 adolescents. The characteristics of the sample are presented in Table I. Briefly, the mean age was 15.1 y, with a proportion male/female 45.9/54.1; 34.1% lived in rural areas, 7.1% were of Indian ethnicity and 35.4% were overweight/obese (Table I).
Prevalence of anemia
The overall prevalence of anemia was 8.5%, greater in females (11.8%), than in males (4.6%).
The geometric mean of s-ferritin was lower in the anemic than in the non anemic subjects (18.32 µg/L vs 32.14 µg/L, respectively, p<0.001). On the contrary, the geometric mean of serum copper in anemic was significantly higher than in non anemic subjects (104.5 µg/dL vs 97.4 µg/dL, respectively, p= 0.018) (data not shown). Iron deficiency was present in 41.6% of all cases of anemia. IDA was greater in anemic females than in males (43.5 vs 36.1%, respectively).
Low iron stores
The geometric mean of s-ferritin was greater in males than in females (39.94±1.03 µg/L vs 24.73±1.04 µg/L respectively). The overall prevalence of LIS was higher in females than in males (18.2% vs 7.9%, respectively) (Table II).
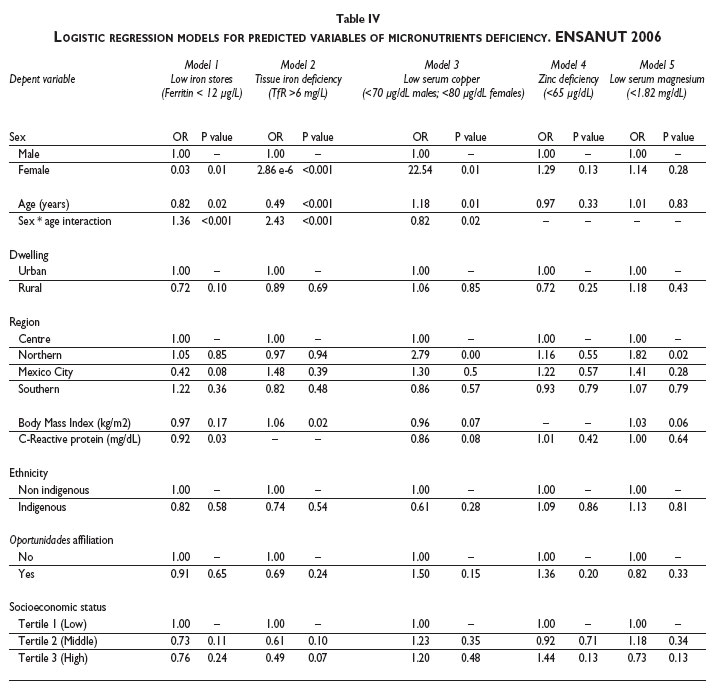
In a logistic model, age and gender had a differential effect on LIS (OR=1.36, p<0.001). The risk increased in females for each year of age (OR= 1.11, p= 0.017); in males the risk was lower with increasing age (OR= 0.82, p= 0.019). No associations were found with dwelling, geographical distribution, SES or ethnicity (Table IV).
Tissue iron deficiency
The geometric mean concentration of sTfR was 3.58±1 mg/L with no significant differences by sex. The overall prevalence of TID was 6.96% (Table II).
In a logistic model, age and gender had a differential effect on TID (OR= 2.43, p<0.001). Age was a higher risk for females (OR=1.19, p= 0.003), but protective in males (OR= 0.5, p<0.001). Higher SES tended to be protective and higher BMI was a risk for TID (OR= 1.05, p= 0.022). No significant differences were found by dwelling, ethnicity, geographical regions, or affiliation to Oportunidades (Table IV).
Dietary iron intake
The overall median daily intake of hem (0.26 mg/d) and non-hem (10.88 mg/d) iron were above the recommended intake. The overall median adequacy for iron intake was 157.3%; 181.5% for males and 136.9% for females. The adequacy of folate and vitamin B12 intake was 70.2% and 110% respectively. The daily intake of enhancers of iron absorption as such as ascorbic acid (vitamin C) had an adequacy of 120%, the intake of inhibitors as such phytic acid was very high (1 240 mg/d).
Total body iron
The adjusted mean of the calculated TBI was lower in females (5.58±0.15 mg/kg) than in males (7.07±0.13 mg/kg, p<0.001). The distribution of TBI was different by sex (K-Smirnof p-value <0.001). A total exhaustion of TBI (TBI= ≤ 0), was more frequent in females (9.12%) than in males (4.82%, p= 0.002).
The TBI increased with age in males (coefficient= 0.66 mg/kg; p<0.001); while it decreased in females (coefficient= -0.15 mg/kg, p= 0.023), adjusted by CRP (Figure 1).

Low serum copper
The mean concentration of serum copper was lower in males (93.23±1.01 µg/dL) than in females (102.9±1.01 µg/dL).
The overall prevalence of low serum copper was 14.14%; with not significant differences by sex. The prevalence was significantly higher in the Northern region (27.14%) than in the Center (11.8%) or the Southern (10.6%) regions; it was also lower in indigenous (7%) than in non indigenous (14.5%) subjects (Table III).
The median daily intake of copper was 0.90 mg/d, with an overall adequacy of 140%; 162% for males and 127.7% for females.
In a logistic regression model, the risk to suffer low serum copper increased with age in males (OR=1.18, p=0.01), but not in females (OR=0.96, p=0.58). Living in the Northern region (OR=2.79, p<0.001) represented a risk for low serum copper. No significant differences were observed by dwelling, SES or affiliation to Oportunidades (Table IV). Intake of copper, phytic acid and fiber (as tertiles) were not associated with LSC (data not shown).
Zinc deficiency
The overall mean of serum concentration of zinc was 92.82±1.02 µg/dL, 95.43±1.03 µg/dL for males and 90.72±1.03 µg/dL for females. The overall prevalence of zinc deficiency was 26.4% (Table III).
The median of dietary intake of zinc was significantly higher for males (8.1 mg/d) than females (6.4 mg/d), with an adequacy of 93%.
In a logistic regression model, no significant associations were found among zinc deficiency and sex, dwelling, region, age, height-for- age z-score, CRP, intake of fiber or phytic acid, zinc, ethnicity, SES or affiliation to Oportunidades. (Table IV). Zinc deficiency was no associated with dietary intake of zinc, phytic acid and fiber (data not shown).
Low serum magnesium
The mean serum concentration of magnesium was 1.92±1.01mg/dL, with no differences by sex. The overall prevalence of low serum magnesium was 37.6%, being higher in the Northern (48.8%) than the Southern region (33.8%) (Table III).
The overall median daily intake of magnesium was 234.9 mg/d, slightly higher for male than for female (268.5 mg/d vs. 215.7 mg/d, respectively), with a median adequacy of 85%.
In a logistic regression model, living in the Northern region was a risk for low serum magnesium (LSM) (OR=1.82, p=0.02). No significant associations were found with sex, dwelling, BMI, CRP, SES, ethnicity or affiliation to Oportunidades (Table IV). LSM was no associated with dietary intake of magnesium, phytic acid and fiber (data not shown).
Discussion
We present evidence herein for a high prevalence of iron, zinc, copper and magnesium deficiencies in Mexican male and female adolescents. Females were more prone to suffer most of mineral deficiencies. When comparing the prevalence of LIS in female adolescents in the NNS-99 with those herein reported, there is a decrement in the prevalence (40.5% vs 18.4%).9,20 However, methodological differences may confound such a big decrease; in 1999 LIS was assessed by percent saturation of transferrin, while in 2006 a direct measurement of s-ferritin was used.
The puberty onset is probably critical to enhance the sexual differences in TBI in this study, i.e. a larger growth of muscle mass in males21 and losses of iron throughout menstruation results in larger TBI in males relative to females. Information on population based estimates of TBI are scanty; data from NHANES III reported in adults older than 20 years mean TBI values of 9.89 ± 2.82 mg/kg for males and 4.87 ±4.14 mg/kg for females,14 similar to those reported herein. We are aware that Cook's equation is not validated for adolescents, however, even if the external validity may be questionable, the internal validity allows for valid comparisons between both genders. We made efforts to homologate our TfR results to Cook's laboratory, correcting as by Ramco's kit.
In the present study, the majority of cases of anemia were not explained by ID; other nutritional causes of anemia as such folate and vitamin B12 deficiencies were not evaluated.22 However, the adequacy of the dietary intake of vitamin B12 was 110%, while the adequacy for folate was 70%. This may explain, in part, the high proportion of non IDA. Both, low and excessive copper serum concentrations are associated with IDA.4,23 In our study, adolescents with anemia had significantly higher serum concentrations of copper than their non anemia counterparts, in line with the reported by NHANES-II.4 The association between iron and copper deficiencies is most probably due to the role of copper as a cofactor of iron oxidizing proteins as such hefastin and ceruloplasmine.24
The possibility of subestimating ID as a cause of anemia could be influenced by acute infections and inflammation. However, the rate of acute infections at this age is low.25 We used a 6 mg/L cut-off for CRP, instead of the usual 3 mg/dL, because in a segmented regression model using data from two probabilistic surveys in Mexican population (n=5 000) the inflexion point for ferritin values occurred at a concentration of 6 mg/L of CRP (data not published).
Low serum copper
The lack of population-based studies on copper status in adolescents prevents from an adequate comparison of our data. The prevalence of low copper concentrations among adolescent girls from Sudan was 5.9%;26 in Iranian pre and postmenopausal women was 17%;27 in Chilean adults the prevalence was 8.6% in males and 5.9% in females.28 The prevalence of low serum copper in our series is one of the highest in the literature. The rarity and letality of genetic diseases associated with copper deficiencies as such Menkes disease and aceruloplasminemia29,30 make difficult to invoke them as significant causes of this large proportion of LSC. It is possible that the higher copper requirement during the puberty growth spurt drains copper out of the circulation.30
Zinc deficiency
The prevalence of zinc deficiency in female adolescents herein reported was similar to that in NNS-99 (29.7%). The overall prevalence was higher than reported for developed countries but lower than for developing countries. In American children 9-19 years of age, the prevalence was 1% for males and 1.3% for females.31 In British children 11-14 and 15-18 years of age the prevalence of zinc deficiency for boys was 0 and 2%, and for girls 2 and 5% respectively.7 Prevalence in Nepalese females 13-35 years of age, varied from 78 to 90%.32 The Mexican prevalence herein reported is lower than for Southeast Asia (71.2%), Africa (68%), East Mediterranean (73.5%) and the Americas (45.8%) but higher than for the West Pacific (18.6%) and Europe: 8.0%.1
The high prevalence of zinc deficiency is relevant for the future health of adolescents because it is associated with higher risks for low birth weight33 and impinges on physical growth in small children.34,35 It also affects negatively on the cognitive function and emotional performance.36
Low serum magnesium
The prevalence of low serum magnesium in this survey is higher than the reported for German individuals (14.5%),3 though, they used a higher cut-off than in this study (1.85 mg/dL vs 1.82 mg/dL, respectively), it is not enough to explain such a large difference. It is more probable that an insufficient diet in Mexico, especially in animal tissue may explain such a difference. We were not able to find serum magnesium data from suboptimally nourished countries. The lower prevalence in the Southern region could be due to the observed higher daily intake of magnesium than in the Northern region (data not shown). We ascertained that the high prevalence was not due to an inaccurate magnesium determination, results were calibrated against NIST SRM 3131a reference materials.
Low serum magnesium causes potassium, calcium and neuromuscular disturbances, central nervous system and cardiovascular alterations, like arrhythmias.37 Also, can alter glucose homeostasis, increase atherosclerosis, hypertension, myocardial infarction, osteoporosis, migraine, asthma, chronic fatigue syndrome, among others.37-39 More research on the effects of magnesium deficiency on the health of adolescents is needed to warrant interventions to prevent it.
The high prevalence of iron deficiency and low serum zinc, magnesium and copper detected in Mexican adolescents could be partially explained by their relatively high intake of antagonists of the absorption of those minerals, as such fiber, tannins and phytates,40 and low intake of enhancers of mineral absorption as such vitamin C.41 The best sources for iron, zinc and copper are animal tissues scarce in the Mexican diet, and could explain the coexistence of deficiencies of those minerals.
The deficiencies detected by the serum concentrations of zinc, cooper and magnesium can be graded from moderate to severe; slight deficiencies are not detected by this method thus their prevalence might be underestimated.
In summary we document here the prevalence and distribution of several mineral deficiencies including iron, copper, zinc and magnesium in Mexican adolescents. Despite several public nutritional interventions in Mexico provide iron and zinc supplementation, the prevalence of iron and zinc deficiencies are still very high, calling for a more careful examination of the effectiveness of those interventions in order to redesign them aiming for better outcomes.
References
1. Ramakrishnan U. Prevalence of micronutrient malnutrition worldwide. Nutr Rev 2002;60:S46-S52. [ Links ]
2. Viteri FE, Gonzalez H. Adverse outcomes of poor micronutrient status in childhood and adolescence. Nutr Rev 2002;60(5 Pt 2):S77-83. [ Links ]
3. Schimatschek HF, Rempis R. Prevalence of hypomagnesemia in an unselected German population of 16,000 individuals. Magnes Res 2001;14(4):283-290. [ Links ]
4. Knovich MA, Il'yasova D, Ivanova A, Molnar I. The association between serum copper and anaemia in the adult Second National Health and Nutrition Examination Survey (NHANES II) population. Br J Nutr 2008;99(6):1226-1229. [ Links ]
5. Hettiarachchi M, Liyanage C, Wickremasinghe R, Hilmers DC, Abrahams SA. Prevalence and severity of micronutrient deficiency: a cross-sectional study among adolescents in Sri Lanka. Asia Pac J Clin Nutr 2006;15(1):56-63. [ Links ]
6. Kassu A, Yabutani T, Mulu A, Tessema B, Ota F. Serum zinc, copper, selenium, calcium, and magnesium levels in pregnant and non-pregnant women in Gondar, Northwest Ethiopia. Biol Trace Elem Res 2008;122(2):97-106. [ Links ]
7. Thane CW, Bates CJ, Prentice A. Zinc and vitamin A intake and status in a national sample of British young people aged 4-18 y. Eur J Clin Nutr 2004;58(2):363-375. [ Links ]
8. Shamah-Levy T, Villalpando S, Rivera JA, Mejia-Rodriguez F, Camacho-Cisneros M, Monterrubio EA. Anemia in Mexican women: a public health problem. Salud Publica Mex 2003;45 Suppl 4:S499-507. [ Links ]
9. Villalpando S, Garcia-Guerra A, Ramirez-Silva CI, Mejia-Rodriguez F, Matute G, Shamah-Levy T, et al. Iron, zinc and iodide status in Mexican children under 12 years and women 12-49 years of age. A probabilistic national survey. Salud Publica Mex 2003;45 Suppl 4:S520-S529. [ Links ]
10. Olaiz-Fernández G, Rivera-Dommarco J, Shamah-Levy T, Rojas R, Villalpando-Hernández S, Hernández-Avila M, eds. Encuesta Nacional de Salud y Nutrición 2006. Cuernavaca, México: Instituto Nacional de Salud Pública, 2006. [ Links ]
11. Lohman T, Roche A, Martorell R. Anthropometric Standardization Reference Manual. Champaign(IL): Human Kinetics Books, 1991. [ Links ]
12. Habicht JP. Standardization of quantitative epidemiological methods in the field. Bol Oficina Sanit Panam 1974;76(5):375-384. [ Links ]
13. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000;320(7244):1240-1243. [ Links ]
14. Cook JD, Flowers CH, Skikne BS. The quantitative assessment of body iron. Blood 2003;101(9):3359-3364. [ Links ]
15. Hess SY, Peerson JM, King JC, Brown KH. Use of serum zinc concentration as an indicator of population zinc status. Food Nutr Bull 2007;28(3 Suppl):S403-S429. [ Links ]
16. Gibson R. Principles of nutritional assessment. Nueva York (NY) ed. O.U. Press, 2005. [ Links ]
17. UNICEF/UNU/WHO. Iron deficiency anemia: assessment, prevention, and control. A guide for programme managers. WHO/NHD (2001)[report no. 01.3] [ Links ].
18. Rodríguez-Ramírez S, Mundo-Rosas V, Jiménez-Aguilar A, Shamah-Levy T. Methodology for the analysis of dietary data from the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2009;51 suppl 4:S523-S529. [ Links ]
19. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington DC: National Academies Press, 2002. [ Links ]
20. Villalpando S, Shama-Levy T, Mundo V, Rivera-Dommarco J. Análisis crítico de la evolución de la prevalencia de anemia y la deficiencia de micronutrimentos en la población. Salud Publica Mex 2007;49 ed especial: E270-E272. [ Links ]
21. Rubinstein JH. Broad thumb-hallux (Rubinstein-Taybi) syndrome 1957-1988. Am J Med Genet Suppl 1990;6:3-16. [ Links ]
22. Chandra J. Megaloblastic anemia: back in focus. Indian J Pediatr 2010;77(7):795-799. [ Links ]
23. Huff JD, Keung YK, Thakuri M, Beaty MW, Hurd DD, Owen J, et al. Copper deficiency causes reversible myelodysplasia. Am J Hematol 2007;82(7):625-630. [ Links ]
24. Frazer DM, Anderson GJ. Iron imports. I. Intestinal iron absorption and its regulation. Am J Physiol Gastrointest Liver Physiol 2005;289(4):G631-G635. [ Links ]
25. Martinez-Garcia MC, Munoz O, Peniche A, Ramirez-Grande ME, Gutierrez G. Epidemiology of acute diarrhoea in a rural medical care system in Mexico (IMSS-COPLAMAR). Arch Invest Med (Mex) 1989;20(1):69-78. [ Links ]
26. Weisstaub S, Bustos M, Olivares M, Castillo D, Araya M. Situación nutricional de hierro, cobre y zinc en escolares de Tacopaya, Bolivia. Rev Bol Ped 2004;43(2):77-80. [ Links ]
27. Mir E, Hossein-nezhad A, Bahrami A, Bekheirnia M, Javadi E, Afshar-Naderi A, et al. Adequate Serum Copper Concentration Could Improve Bone Density, Postpone Bone Loss and Protect Osteoporosis in Women. Iranian J Public Health 2007:24-29. [ Links ]
28. Cediel G, Olivares M, Araya M, Letelier M, López de Romana D, Pizarra F. Efecto de la inflamación subclínica sobre el estado nutricional de hierro, cobre y zinc en adultos. Rev Chil Nutr 2009;36:8-14. [ Links ]
29. Houwen RH. Copper: two sides of the same coin. Neth J Med 2008;66(8):325-326. [ Links ]
30. Olivares M, Araya M, Uauy R. Copper homeostasis in infant nutrition: deficit and excess. J Pediatr Gastroenterol Nutr 2000;31(2):102-111. [ Links ]
31. Pilch SM, Senti FR. Analysis of zinc data from the second National Health and Nutrition Examination Survey (NHANES II). J Nutr 1985;115(11):1393-1397. [ Links ]
32. Chandyo RK, Strand TA, Mathisen M, Ulak M, Adhikari RK, Bolann BJ, et al. Zinc deficiency is common among healthy women of reproductive age in Bhaktapur, Nepal. J Nutr 2009;139(3):594-597. [ Links ]
33. King JC. Determinants of maternal zinc status during pregnancy. Am J Clin Nutr 2000;71(5 Suppl):1334S-1343S. [ Links ]
34. Brown KH, Peerson JM, Rivera J, Allen LH. Effect of supplemental zinc on the growth and serum zinc concentrations of prepubertal children: a meta-analysis of randomized controlled trials. Am J Clin Nutr 2002;75(6):1062-1071. [ Links ]
35. Bhutta ZA, Black RE, Brown KH, Gardner JM, Gore S, Hidayat A, et al. Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: pooled analysis of randomized controlled trials. Zinc Investigators' Collaborative Group. J Pediatr 1999;135(6):689-697. [ Links ]
36. Tupe RP, Chiplonkar SA. Zinc supplementation improved cognitive performance and taste acuity in Indian adolescent girls. J Am Coll Nutr 2009;28(4):388-396. [ Links ]
37. Swaminathan R. Magnesium metabolism and its disorders. Clin Biochem Rev 2003;24(2):47-66. [ Links ]
38. King DE. Inflammation and elevation of C-reactive protein: does magnesium play a key role? Magnes Res 2009;22(2):57-59. [ Links ]
39. Barbagallo M, Dominguez LJ. Magnesium metabolism in type 2 diabetes mellitus, metabolic syndrome and insulin resistance. Arch Biochem Biophys 2007;458(1):40-47. [ Links ]
40. Hambidge KM, Miller LV, Westcott JE, Sheng X, Krebs NF. Zinc bioavailability and homeostasis. Am J Clin Nutr 91(5):1478S-1483S. [ Links ]
41. Lozada AL, Flores M, Rodríguez S, Barquera S. Patrones dietarios en adolescentes mexicanas. Una comparación de dos métodos. Encuesta Nacional de Nutrición, 1999. Salud Publica Mex 2007;49(4):263-273. [ Links ]
 Corresponding author:
Corresponding author:
Dr. Salvador Villalpando.
Instituto Nacional de Salud Pública.
Av. Universidad 655, Col. Santa María Ahuacatitlán.
62100 Cuernavaca, Morelos, México.
E-mail: svillalp@insp.mx
Received on: April 18, 2011
Accepted on: August 24, 2011
Declaration of conflict of interest: The authors declare that they have no conflict of interests.


{kind=link}
{kind=link}
{kind=link}
{kind=link}