










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkSalud Pública de México
Print version ISSN 0036-3634
Salud pública Méx vol.54 n.1 Cuernavaca Jan./Feb. 2012
ORIGINAL ARTICLE
Cost-effectiveness analysis of the use of palivizumab in the prophylaxis of preterm patients in Mexico
Análisis de costo-efectividad del uso de palivizumab en la profilaxis de pacientes prematuros en México
Guillermo Salinas-Escudero, MScI; Silvia Martínez-Valverde, MScI; Alfonso Reyes-López, MScI; Juan Garduño-Espinosa, MD, MScII; Onofre Muñoz-Hernández, MD, MScII; Víctor Granados-García, MSc,III; Kely Rely, MD, MSc.IV
ICentro de Estudios Económicos y Sociales en Salud. Dirección de Investigación, Hospital Infantil de México Federico Gómez, Secretaría de Salud. México, DF
IIDirección de Investigación, Hospital Infantil de México Federico Gómez, Secretaría de Salud. México, DF
IIIUnidad de Investigación en Economía de la Salud, Instituto Mexicano del Seguro Social. México, DF
IVCEA Health Tech. México DF
ABSTRACT
OBJECTIVE: The study evaluated the incremental cost-effectiveness ratio (ICER) of the prophylaxis of palivizumab, for the reduction of complications associated to the respiratory syncytial virus in preterm patients in Mexico.
MATERIAL AND METHODS: A decision tree was developed in preterm groups [<29 and 29-32 weeks of gestational age (wGA)], by using epidemiological and cost local data; the effectiveness was obtained with a systematic review. Patients were evaluated according to their life expectancy. Mexican Health System perspective was used. Effectiveness measures employed were LYG and QALYs. The costs are reported in USD 2009.
RESULTS: ICERs per LYG resulted on values of USD $25,029 and USD $29,637 for <29 wGA and 29-32 wGA respectively, whereas ICERs per QALYs obtained in the model accounted for USD $17,532 and USD $20,760.
CONCLUSIONS: Palivizumab prophylaxis for preterm newborn patients ≤32 weeks of age resulted in a cost-effective alternative.
Key words: cost effectiveness; respiratory syncytial virus; antibodies; monoclonal; QALY; Mexico.
RESUMEN
OBJETIVO: El estudio evaluó la razón costo-efectividad incremental (RCEI) de profilaxis con palivizumab para reducción de complicaciones asociadas al virus sincicial respiratorio en prematuros en México.
MATERIAL Y MÉTODOS: Se empleó un árbol de decisiones en los grupos pretérmino [<29 y 29-32 semanas de edad gestacional (SEG)], empleando datos epidemiológicos y costos locales; la eficacia se obtuvo con una revisión sistemática, evaluando a los pacientes de acuerdo con su esperanza de vida. Se empleó la perspectiva del Sistema Nacional de Salud. Las medidas de eficacia fueron AVG y AVAC. Los costos son reportados en dólares de 2009.
RESULTADOS: Las RCEI por AVG resultaron de USD $25 029 y USD $29 637 para <29 y 29-32 SEG, mientras que las RCEI por AVAC fueron de USD $17 532 y USD $20 760.
CONCLUSIONES: La profilaxis con palivizumab en pacientes recién nacidos pretérmino ≤32 semanas de edad resultó ser una alternativa costo-efectiva.
Palabras clave: costo-efectividad; virus sincicial respiratorio; anticuerpo monoclonal; AVAC; México.
Respiratory syncytial virus (RSV) is the most frequent etiologic agent associated with acute respiratory infection during childhood. Clinical expression of the RSV in children is more commonly observed as bronchiolitis or viral pneumonia, and the group under two years of age is the most affected by this infections.1
The majority of healthy children who develop this infection do not need hospitalisation; the infection is self-limiting and mortality in this group is less than 1%.2 However, in high-risk groups, such as premature newborn, children suffering from chronic lung disease (CLD) or congenital cardiophaty (CC), hospitalisation rates are higher, up to 20% in the US2 and 13% in Spain.3
RSV-associated pneumonia or bronchiolitis during childhood are considered a risk factor for children to develop recurrent wheezing or asthma,4-6 especially in those premature and those with bronchopulmonary dysplasia.7-9 These factors may contribute to diminish the child's quality of life in further stages.10,11
Studies conducted in Brazil, Colombia, and Thailand, demonstrated that RSV causes between 20 and 30% of acute respiratory disease (ARD) in children between 1-4 years of age, similar to prevalence in developed countries.12 In the US between 85 000 and 144 000 children are hospitalised due to RSV infection every year.13 These numbers represent between 20 and 25% of pneumonia hospitalisations and up to 70% of bronchiolitis hospitalisations.14,15 RSV is responsible of four million children deaths per year due to lower acute respiratory infection.16
At the current time, and given that there is no available vaccine to prevent RSV infection, control measures are employed to prevent the aerial transmission of the virus, in addition to administration of specific antibodies, such as palivizumab, which is a monoclonal humanized antibody developed against the fusion protein of the RSV. This drug was approved by the US Food and Drug Administration (FDA) in 1998 and by the European Medicines Agency (EMEA) in 1999.
Palivizumab is a monoclonal lgG1k humanized antibody, directed against an epitope of the A antigenic space of the RSV fusion protein. This monoclonal humanized antibody is composed by human and murine antibody sequences (95, and 5%, respectively).
Controlled clinical trials mentioned at the systematic review section have demonstrated the efficacy of palivizumab for the reduction of RSV infection-related hospitalisation in high-risk patients.
However, due to the fact that most of the studies already published include different risk groups (in terms of gestational age and co-morbidities), generalization of results is not feasible. In the specific case of preterm newborn infants [<32 weeks of gestational age (wGA)], results on cost-effectiveness are controversial in relation to quality adjusted life years (QALY)17-20 and life years gained (LYG).18
In Mexico, prophylaxis with palivizumab has been included in the Interinstitutional Basic Formulary; however, there is not strong evidence about its clinical and economic benefits. Due to this, the purpose of the current study is to undertake an assessment of the economic and clinical benefits of palivizumab and of the potential impact of palivizumab prophylaxis on the public health institutions and on the Mexican population, contributing in that way with elements to inform health authorities´ decision making.
The perspective of the evaluation is based on the public health institutions in Mexico, by employing the Social Security Mexican Institute (IMSS) cost data. IMSS covers 80.8% of the people with social security,21 and 44.9% of the entire population.22,23 Due to this, the study considers only direct medical costs which are evaluated during patient's lifetime (time horizon), and costs and health results were discounted by using an annual 3% discount rate.
Material and Methods
Model
The analysis is based on a pharmacoeconomic model represented by a decision tree which compares three different scenarios and two wGA groups:1
• The employment of palivizumab prophylaxis during the six months corresponding to the RSV season in Mexico (from October to March every year), given to preterm patients <29 wGA and preterm patients 29-32 wGA who were born during the RSV season and those who were up to six months old when the RSV season started (full coverage scenario).
• The employment of palivizumab prophylaxis during the six months corresponding to the RSV season in Mexico, given only to those preterm patients <29 wGA and 29-32 wGA who were born during the RSV season (partial coverage scenario).
• No prophylaxis scenario.
The model begins with the selection of each of the possible treatment alternatives for each preterm group (<29 wGA and 29-32wGA), where there is the option to receive prophylaxis or not.
In the case of management without prophylaxis, the natural history of the disease is taken into account, i.e., it is assumed a probability of infection within the RSV season during the first life year, which means that a percentage of patients are not infected with RSV, the rest of the patients will attend the emergency department of a hospital, where they can be sent back home (discharge or ambulatory care) or can be hospitalized for treatment within the medical facility (hospital management). We assumed that patients with RSV infection may die or survive the disease episode, and in case of survival, the patient might present, during the second life year, sequelae related to the disease such as episodes of asthma, where the patient might again die or survive the sequelae episode. If the patient survives after the second year, they will have a normal life expectancy (figure 1).
In the case of prophylaxis with palivizumab, the natural history of the disease is modified in three main aspects: the first corresponds to hospitalization rates that require medical care associated with RSV infections, the second involves mortality rates in both inpatient and outpatient management, and the third affects the prevalence rates of asthma sequelae.
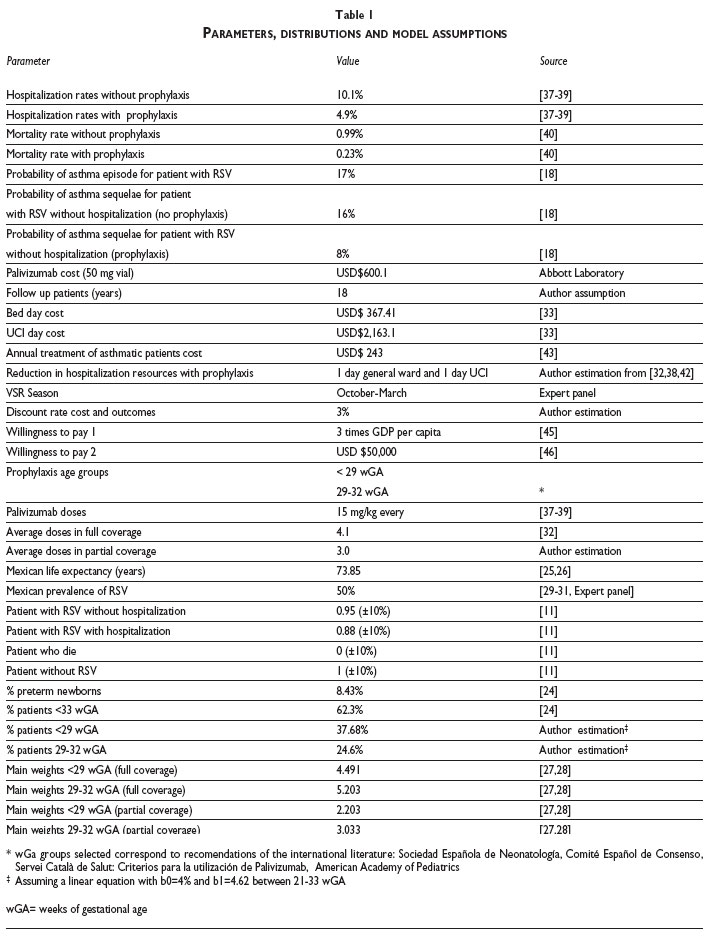
In Mexico, according to the IMSS data,24 8.43% of births are preterm patients, where patients <33 weeks represent 62.3%. In the current model, within the <33 weeks group, it was estimated that the subgroups of preterm patients <29 weeks and 29-32 weeks represent the 60.5 and 39.5% respectively (37.68, and 24.6% of the whole preterm patients).
Life expectancy in the model used for the Mexican population is 73.85 years,25,26 which corresponds to the birth rate by sex and life expectancy of each sub-group.
Also, given that there is a lack of information regarding the time distribution of deaths in Mexico for newborns, it was assumed in the model that, irrespective of the month in which those children died during the first or second year under study, the effectiveness would be adjusted to the half period (0.5 or 1.5 year) rather than considering the full period (1 or 2 years).
The children weights used in the model correspond to Fenton27 and the National Center for Health Statistics28 growth charts of preterm patients by sex, up to the 50th week of age, and posterior estimations (weeks 51–83, where the number of weeks does not correspond to the gestational age but with the age an infant will have when is discharged home) were conducted using the NCHS.28 The weights of the preterm patients used in the different groups analyzed in the scenario of full coverage are 4.491 kg for <29 weeks and 5.203 kg at 29-32 weeks. Meanwhile, in the scenario of patients discharged during the RSV season, the weights used are 2.203 kg for those less than 29 weeks and 3.033 kg in 29-32 weeks.
The cumulative prevalence of RSV used for patients during the first 12 months for Mexico was 50%,29-31 and it was validated by a panel of medical experts on RSV.
We considered a regular pattern of five applications with a dose of 15 mg/kg of palivizumab every 30 days during the RSV season. An average of 4.1 vials given to children was an assumption used in the scenario of complete coverage, which corresponds to what is published in the IRIS study.32 While an average of 3.0 applications was used for the scenario of coverage of patients born during the RSV season.
The quality of life measures used in the model to calculate the QALY were obtained in part from the Greenhough study,11 in which a value of 0.95 per year is reported for patients who presented RSV but did not required hospitalization, and 0.88 for those patients that required hospitalization. The value for those patients who did not suffer from RSV was 1 and for those who died from it was 0. Also, it is assumed that, on average, death arises at the middle point of the period (given that annual cycles were considered in the study).
Effectiveness
A systematic review of literature was conducted in the third quarter of 2009. Controlled clinical trials were identified which evaluated the use of palivizumab prophylaxis in patients at high risk (premature, presenting bronchopulmonary dysplasia, congenital heart disease, etc.). The search was carried out by identifying titles and articles in the following electronic databases, on the OVID platform: Medline, EMBASE and Cochrane Collaboration. The following MeSH terms or text words were used for search strategy: palivizumab, clinical trial, controlled clinical trial, cohort studies. The search period was between January 1, 1998 and August 31, 2009.
From a total of 429 references, 67 articles were reviewed, and 11 fulfilled the inclusion criteria. Studies were published between 1998 and 2008. The main outcome of these studies is the hospitalization frequency due to respiratory infections related to RSV.
Hospitalization rates employed in the model were taken from the rates reported in the clinical trials (Cardiac Synagis Study Group, The IMpact-RSV Study Group, MEDI-493 Study Group), where the non-prophylaxis group had a rate of 10.1% compared with 4.9% of the prophylaxis group.33-35 The use of such trials reduces the probability of bias to occur, expressed in treatment effects differences.
Mortality data were obtained from the Checchia meta-analysis.36 This study reports a mortality rate of 0.99% for preterm newborn ≤32 weeks of age and no-prophylaxis with palivizumab. In contrast the group that received prophylaxis reported a mortality rate of 0.23%. The same rates were employed in the subgroups analysis.
Sequelae rates in terms of asthma for both groups of preterm patients <33 weeks and suffering from RSV infection, correspond to those reported in the Chirico G18 study which recalls Simoes EA8 and Ravasio R37 studies. Reported probability of having posterior episodes of asthma for patients with RSV is 17% (irrespective of whether they received prophylaxis or not). For those patients infected with RSV and who did not required hospitalization, this probability accounts for 8% in the prophylaxis groups and 16% for patients who did not receive prophylaxis.
After evaluating the probability of having asthma episodes, the model considers a patient's follow-up until 18 years of age due to the fact that at that age, patients loose the coverage they receive from the IMSS.
Resource utilization
To obtain the use of medical resources, we conducted a panel of 13 medical experts on RSV in children <2 years familiar with the management of patients in hospitals of the second and third level of attention in IMSS. The physicians were recruited by the authors of this document. A questionnaire was used as a tool to collect data regarding resource utilisation, based on the experience of the experts in the treatment of children infected with RSV.
Costs
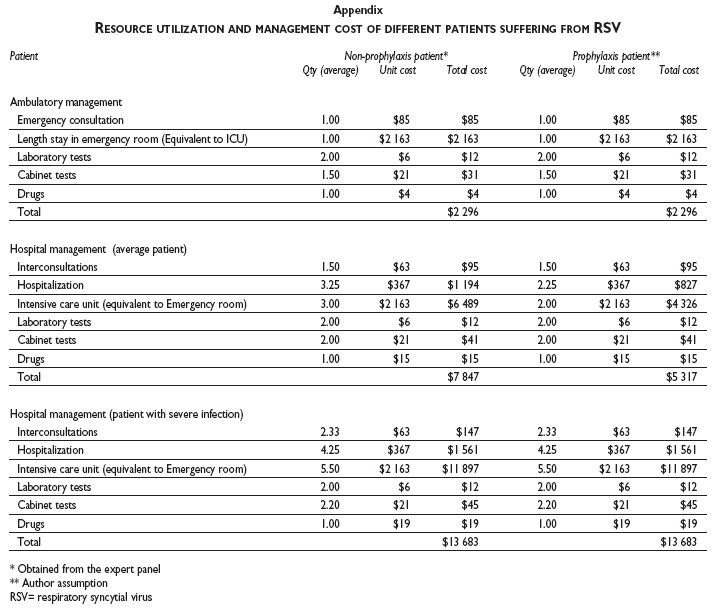
The first cost group corresponds to the direct medical costs incurred by the IMSS-associated with the care of RSV complications of preterm patients (outpatient, inpatient and sequelae) (appendix).
The second cost group corresponds to the IMSS cost if they provide prophylaxis with palivizumab (appendix).
To estimate the costs of care, the medical care costs of IMSS 200938 were used and the unitary purchasing costs of drugs for the IMSS for the period January to December 200839 adjusted for the recent inflation factor in order to obtain all costs in 2009 prices and converted to USD Nov 2009.40 As for the estimation of the costs of palivizumab prophylaxis, we used the USD $ 600.1 (50 mg vial), which corresponds to the price of government sales for Abbott's lab in Mexico for the year 2009.
Outcome parameter for the cost-effectiveness analysis
Life years gained (LYG) and QALY were used as measures of effectiveness. Model results for the base case are expressed in terms of effectiveness and cost differentials between palivizumab prophylaxis scenarios and the scenario without prophylaxis, as well as in terms of the incremental cost-effectiveness ratio (ICER).
Sensitivity analysis
A sensitivity analysis was performed of the parameters subject to greater uncertainty and/or that might influence the outcome of the analysis. We performed a one-way analysis of tornado-like type on the results in QALYs for both palivizumab prophylaxis scenarios: full coverage and partial coverage.
In addition, probabilistic analysis was performed through a Monte Carlo simulation, in which individually clinical outcomes of 1 000 hypothetical patients were modeled.40 The odds have been set as beta distributions based on the number of hits (alpha parameters) and failures (beta parameters) and gamma to the costs of care.
Results
Resource utilization and cost inputs
Table I shows resource utilization patterns for the management of the two possible groups of patients as well as mean costs and their distributions.
For the model purposes, it was assumed that resources employed in patients who received prophylaxis were the same in case of ambulatory management and death. However, given that the reduction in terms of hospitalization reported in the international literature shows savings up to 50% of the total time32,34,42 the model includes a conservative reduction of one day less in ICU and one day less in general ward for hospitalized patients.
Annual costs of treatment for asthmatic patients considered in the model were USD $243, according to the Ceballos ZI43 study conducted in Mexico by using a cohort of asthmatic patients within the IMSS. This cost was adjusted by inflation rate40 and exchange rate.44
Taking into account that social security systems in Mexico give coverage to children until the age of 18, the model considers as costs of consequences the cost of treating asthma for 18 years. So the medical care costs to charge by the IMSS, only have been considered during this time.
Total costs
Prophylaxis groups reported, in the model, a reduction of medical care costs in a range between 23.61 - 23.68% depending on the group under analysis. Notwithstanding these reductions, prophylaxis associated incremental costs depend on the type of coverage and the age group (i.e.: 39% for the group <29 weeks during RSV season; and 180% for the group between 29 – 32 weeks for the whole year prophylaxis). The latter implies that prophylaxis-associated cost represents between 45.3 - 72.1% of the total cost.
Cost effectiveness analysis
Table II reports the results obtained from the deterministic cost-effectiveness analysis in terms of the incremental effectiveness and cost per scenario and wGA group.
When comparing the prophylaxis and non-prophylaxis groups, the mean effectiveness values are for the prophylaxis group: 0.12 LYG and 0.16 QALY.
When evaluating the ICER per QALY and LYG against the USD $50 000 threshold, all age groups within the prophylaxis group are cost effective strategies irrespective of the type of coverage (RSV season or yearly coverage).
In the case of the threshold recommended by the WHO (three times the GDP per capita of the country), all groups where cost effective when the QALY where used as effectiveness units, whereas the ICER distributions expressed in LYG are no more cost effective.
Finally, all the strategies can be considered as cost effective in the case of RSV season coverage, where the group of <29 weeks had the best ICER among the two different age groups.
One way sensitivity analysis results
Figure 2 shows the impact in LYG and QALY given by a one way sensitivity analysis for both scenarios. Once the sensitivity analysis was conducted, similar results were obtained for the analyzed groups, so the figure aggregates in one graph the results of these groups put together.
The variables with the highest sensitivity in the model were:
• Discount rate: At this respect, the higher the discount rate, the higher the ICER is.
• RSV prevalence: The higher the RSV prevalence, the more favorable the ICER. When reducing such prevalence, the ICER resulted in higher costs.
All other variables, including asthma sequelae, mean weight, efficacy, measured in terms of mortality reduction and unit price did not affect the ICER.
Probabilistic sensitivity analysis results
The ICER distributions from the probabilistic model for both full and partial coverage scenarios are cost effective because they are below the USD $50 000 threshold, irrespective of the effectiveness units considered (international benchmark for developed countries).46
When switching to a three times the GDP per capita threshold, the ICER distributions per LYG are no more cost effective. However, the ICER distributions expressed in QALYs remained cost-effective for the full coverage scenario. It is worth to mention that QALYs represent a more complete measurement unit for this study purpose given that they address the quality of life aspect. Quality of life is not captured by LYG. Under the partial coverage scenario, both ICER resulted cost-effective for a 3 times the GDP per capita threshold.
Acceptability curves
In terms of LYG, and according to the model results, the probability of the alternatives to be cost effective in the probabilistic model for the full coverage scenario, when using a three times GDP per capita and USD $50 000 thresholds per group are:
• Group <29 wGA: 51% and 96%.
• Group between 29-32 wGA: 37% and 92%.
In the case of a partial coverage scenario, all the alternatives were 100% likely to be cost effective irrespective of the threshold to be compared with.
The probabilities of the two groups to be cost effective in terms of QALY's, and under the full coverage scenario were 75, and 65% by using a three GDP per capita threshold; and 98, and 96% by using a WTP of USD $50 000 per QALY (figure 3).
For the scenario of partial coverage, all probabilities accounted for a 100% probability of being cost effective irrespective of the WTP.
Discussion
Results obtained from the model are favorable for the prophylaxis groups. When the prophylaxis is provided during the RSV season results are even better. This may be explained because the reduction of weight and mean doses applied to the patients. This represents a good alternative for those countries with high rates of preterm newborn children who are underweight.
The ICER obtained from both deterministic and probabilistic models allocate the prophylaxis scenarios as cost-effective alternatives when using the WTP above mentioned per LYG and per QALY.
Since Mexico does not have a threshold that represents the WTP per unit of effectiveness (LYG or QALY), the ICER results per QALY were evaluated by using two international threshold references in order to evaluate the willingness to pay of the Mexican authorities: the first value is the threshold usually reported for developed countries (USD $50 000), whereas the second reference corresponds to the World Health Organization (WHO) recommendation (three times the GDP per capita).45 This last value would account for about USD $25 24347,48 or MXN $327 666 (exchange rate of MXN$12.98 per USD $1).44
Comparing the results obtained in this study with results from other studies, some differences arise, i.e. in the study of ElHassan17 two models were developed. The first model considered the risk of acquiring recurrent sibilance following a RSV infection, whereas the second model does not consider such risk.
Patients included in the model were premature newborn between 26 and 32 weeks of gestational age. The results of this study conclude that the ICER obtained is cost-effective for the palivizumab prophylaxis only if benefits generated by a decrease in the risk of recurrent sibilance in patients who suffer from RSV infection are taken into account.
Compared with the results obtained in the current study, ElHassan's results did not find evidence about the long term benefits of palivizumab in terms of deaths avoided as well as the long term improvement in quality of life.17
Nuijten20 estimates the cost-effectiveness ratio of palivizumab for the prevention of severe RSV infection in preterm newborn <32 weeks who are considered high-risk patients. The evaluation was conducted under the perspective of the National Spanish Health Service. The ICER accounted for USD $16 914 (exchange rate 0.75 Dollar per Euro) per LYG. The results from the study suggest that palivizumab prophylaxis is a cost-effective alternative with respect to hospitalization in Spain. The main difference with respect to the present study is that the protection factor given by the prophylaxis is 5.2% in terms of hospitalization days avoided versus 9.35 % for the Spanish data. Another difference that came up refers to the employment of indirect costs in the Spanish study, such as productivity losses attributable to premature death.
Chirico18 estimated the ICER per QALY in a group of preterm newborns <33 weeks but the study did not specify the number of weeks to be considered in the evaluation model. The value of the ICER was USD $11 452 (exchange rate 0.75 Dollar per Euro) per LYG, using a 3% discount rate.
Coverage levels employed in the model were located in a range between 20-40%. Such levels were established in accordance with the most likely coverage to be given by the public health institutions in Mexico. It is worth to mention that for the model purposes, coverage was assumed to be given only to high-risk patients during the RSV season. This implies that it is not possible to consider 100% coverage because not all the preterm children are born during the RSV season.
In terms of the RSV season in Mexico, although there is not an official established RSV season, the expert panel determined the season to be between October and March.
Palivizumab prophylaxis for preterm newborn patients ≤32 wGA resulted in a cost-effective alternative for the prevention of RSV infection and its complications in Mexico. The scenario of partial coverage during the RSV season in the country allow having a better a cost-effectiveness results, compared with a non prophylaxis scenario, especially in those situations in which budget restrictions are important.
Disclosure
The authors received support by Abbott Laboratories of Mexico to implement the panel of experts and for the translation of the final version of the paper.
References
1. Meissner HC, Welliver RC, Chartrand SA, Law BJ, Weisman LE, Dorkin HL, et al. Immunoprophylaxis with palivizumab, a humanized respiratory syncytial virus monoclonal antibody, for prevention of respiratory syncytial virus infection in high risk infants: a consensus opinion. Pediatr Infect Dis J 1999;18(3):223-231. [ Links ]
2. Groothuis JR, Simoes EA, Levin MJ, Hall CB, Long CE, Rodríguez WJ, et al. Prophylactic administration of respiratory syncytial virus immune globulin to high-risk infants and young children. The Respiratory Syncytial Virus Immune Globulin Study Group. N Engl J Med 1993;329(21): 1524-1530. [ Links ]
3. Carbonell-Estrany X, Quero J, and the IRIS Study Group. Tasas de hospitalización por infección por virus respiratorio sincitial en prematuros nacidos en dos estaciones consecutivas. Pediatr Infect Dis J 2001;20(9):874-879. [ Links ]
4. Piedimonte G. The association between respiratory syncytial virus infection and reactive airway disease. Respir Med 2002; 96 Suppl B:S25-S29. [ Links ]
5. Sigurs N, Gustafsson PM, Bjarnason R, Lundberg F, Schmidt S, Sigurbergsson F, et al. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am J Respir Crit Care Med 2005;171(2):137-141. [ Links ]
6. Sigurs N, Aljassim F, Kjellman B, Robinson PD, Sigurbersgsson F, Bjarnason R, et al. Asthma and allergy patterns over 18 years after severe RSV bronchiolitis in the first year of life. Thorax 2010; 65(12):1045-1052. doi:10.1136/thx.2009.121582. [ Links ]
7. Cardenas S, Auais A, Piedimonte G. Palivizumab in the prophylaxis of respiratory syncytial virus infection. Expert Rev Anti Infect Ther 2005;3(5):719-726. [ Links ]
8. Simoes EA, Groothuis JR, Carbonell-Estrany X, Rieger CH, Mitchell I, Fredrick LM, et al. Palivizumab prophylaxis, respiratory syncytial virus, and subsequent recurrent wheezing. J Pediatr 2007;151(1):34-42, e1. [ Links ]
9. Puddu M, Fanos V. Respiratory syncytial virus infection and recurrent wheezing: what next? J Chemother 2007;19 Suppl 2:8-11. [ Links ]
10. Bont L, Steijn M, Van Aalderen WM, Kimpen JL. Impact of whezzing after respiratory syncytial virus infection on healthrelated quality of life. Pediatr Infect Dis J 2004;23(5):414-417. [ Links ]
11. Greenough A, Alexander J, Burgess S, Bytham J, Chetcuti PA, Hagan J, et al. Health care utilisation of prematurely born, preschool children related to hospitalisation for RSV infection. Arch Dis Child 2004;89(7): 673-678. [ Links ]
12. World Health Organization (WHO). Respiratory syncytial virus and parainfluenza viruses. [Update September 2009]. [Accessed 2009 November] Available at: http://www.who.int/vaccine_research/diseases/ari/en/index2.html [ Links ]
13. Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bronchiolitis-associated hospitalizations among US children, 1980-1996. JAMA 1999;282(15):1440-1446. [ Links ]
14. Hall CB. Respiratory syncytial virus and parainfluenza virus. N Engl J Med 2001;344(25):1917-1928. [ Links ]
15. Henrickson KJ, Hoover S, Kehl KS, Hua W. National disease burden of respiratory viruses detected in children by polymerase chain reaction. Pediatr Infect Dis J 2004;23(1 Suppl):S11-S118. [ Links ]
16. Garenne M, Ronsmans C, Campbell H. The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries. World Health Stat Q 1992; 45(2-3):180-191. [ Links ]
17. ElHassan NO, Sorbero ME, Hall CB, Stevens TP, Dick AW. Cost-effectiveness Analysis of Palivizumab in Premature Infants Without Chronic Lung Disease. Arch Pediatr Adolesc Med 2006;160(10):1070-1076. [ Links ]
18. Chirico G, Ravasio R, Sbarigia U. Cost-utility analysis of palivizumab in Italy: results from a simulation model in the prophylaxis of respiratory syncytial virus infection (RSV) among high-risk preterm infants. Italian J Pediatr 2009;35(1):4. [ Links ]
19. Yount LE, Mahle WT. Economic Analysis of Palivizumab in Infants With Congenital Heart Disease Pediatrics 2004;114(6);1606-11. [ Links ]
20. Nuijten MJ, Wittenberg W. Cost effectiveness of palivizumab in Spain: an analysis using observational data. Eur J Health Econ 2010;11(1):105-115. [ Links ]
21. Secretaría de Gobernación. Anexo Estadístico Tercer Informe de Gobierno. Felipe Calderón Hinojosa. 2009. Pag 270. [Accessed 2009 November 6]. Available at: http://www.informe.gob.mx/anexo_estadistico/pdf/2_3.pdf. [ Links ]
22. Instituto Nacional de Estadística y Geografía. XII Censo General de Población y Vivienda 2000. México: INEGI, 2000. [ Links ]
23. Instituto Nacional de Estadística y Geografía. II Conteo de Población y Vivienda 2005. México: INEGI, 2006. [ Links ]
24. Instituto Mexicano del Seguro Social (IMSS). Estadísticas Médicas DATA MART. Asistencia Infantil. Peso y Edad Gestacional Enero-Junio 2009. [Accessed 2009 September 15]. Available at: http://www.imss.gob.mx/dpm/dis/Tabla.aspx?ID=SCRS04_0020_09&OPC=opc04&SRV=M00-1 [ Links ]
25. Consejo Nacional de Población (CONAPO). Indicadores demográficos básicos 1990-2030.[ Accessed 2009 November]. Available at: http://www.conapo.gob.mx/index.php?option=com_content&view=article&id=125&Itemid=193 [ Links ]
26. Secretaría de Gobernación. Anexo Estadístico Tercer informe de Gobierno. Felipe Calderón Hinojosa. 2009. Pag 59. [Accessed 2009 October 15] Available at: http://www.informe.gob.mx/anexo_estadistico/pdf/1_4.pdf. [ Links ]
27. Fenton TR. A new growth chart for preterm babies: Babson and Benda's chart updated with recent data and a new format. BMC Pedriatr 2003;16; 3:13 [ Links ]
28. National Center for Health Statistics in collaboration with the National Center for Chronic Disease Prevention and Health Promotion (2000). USA. [Accessed 2009 October]: Available at: http://www.cdc.gov/growthcharts [ Links ]
29. Wright AL, Taussig LM, Ray CG, Harrison HR, Holberg CJ. The Tucson Children's Respiratory Study. II. Lower respiratory tract illness in the first year of life. Am J Epidemiol 1989; 129(6):1232-1246. [ Links ]
30. Darville T, Yamauchi T. Respiratory syncytial virus. Pediatr Rev 1998; 19(2):55-61 [ Links ]
31. Dubois B, Ray G. Viral infections of the lower respiratory tract. Pediatric Respiratory Medicine. China: Taussig-Landau, 1999; 573-579. [ Links ]
32. Pedraz C, Carbonell-Estrany X, Figueras-Aloy J, Quero J, and IRIS Study Group. Effect of palivizumab prophylaxis in decreasing respiratory syncytial virus hospitalizations in premature infants. Pediatr Infect Dis J 2003;22(9):823-827. [ Links ]
33. Feltes TF, Cabalka AK, Meissner HC, Piazza FM, Carlin DA, Top FH Jr, et al. Cardiac Synagis Study Group: Palivizumab prophylaxis reduces hospitalization due to respiratory syncytial virus in young children with hemodynamically significant congenital heart disease. J Pediatr 2003;143(4):532-540. [ Links ]
34. The Impact-RSV Study Group: Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. Pediatrics 1998;102(3):531-537. [ Links ]
35. Subramanian KN, Weisman LE, Rhodes T, Ariagno R, Sánchez PJ, Steichen J, et al. Safety, tolerance and pharmacokinetics of a humanized monoclonal antibody to respiratory syncytial virus in premature infants and infants with bronchopulmonary dysplasia. MEDI-493 Study Group. Pediatr Infect Dis J 1998;17(2):110-115. [ Links ]
36. Checchia PA, Nalysnyk L, Fernandes A, Mahadevia P, Xu Y, Fahrbach K, et al. Mortality and Morbidity Among High-Risk Preterm Infants Receiving Palivizumab Prophylaxis: A Systematic Review and Meta-Analysis. Pediatric Crit Care Med. 2011;12(5):580-588. [ Links ]
37. Ravasio R, Lucioni C, Chirico G. Costo-efficacia di palivizumab versus non profilassi nella prevenzione delle infezioni da VRS nei bambini pretermine, a diversa età gestazionale. PharmacoEconomics – Italian Research Articles 2006; 8(2):105-117. [ Links ]
38. Instituto Mexicano del Seguro Social. Secretaria General de Aviso: Costos unitarios de la atención médica. Diario Oficial de la Federación. Martes 9 de marzo de 2004. Primera Sección. [ Links ]
39. Instituto Mexicano del Seguro Social (IMSS). Portal de Transparencia. IMSS va a comprar, IMSS compró. Periodo Enero-Diciembre 2008: [Accessed 2009 November]. Available at: http://transparencia.imss.gob.mx/trnsp/ncompro.aspx?c=1 [ Links ]
40. Banco de México. Inflación. [Accessed 2009 November 19]. Available at: http://www.banxico.org.mx/portal-inflacion/index.html [ Links ]
41. Briggs AH, Goeree R, Blackhouse G, O'Brien BJ. Probabilistic analysis of cost-effectiveness models: choosing between treatment strategies for gastroesophageal reflux disease. Med Decis Making 2002;22(4): 290-308. [ Links ]
42. Wegner S, Jacobson-Vann J, Liu G, Byrns P, Cypra C, Campbell W, et al. Direct Cost Analyses of Palivizumab Treatment in a Cohort of At-Risk Children: Evidence From the North Carolina Medicaid Program. Pediatrics 2004;114(6):1612-1619. [ Links ]
43. Martínez ZI, Bahena ME, Jurado LS, Hosking JE. Costo directo de la atención por crisis aguda de asma en el servicio de urgencias pediátricas. Rev Alergia Mex 2004; 51(4):134-138. [ Links ]
44. Banco de México. Mercado cambiario. [Accessed 2009 November 19]. Available at: http://www.banxico.org.mx/portal-mercado-cambiario/index.html [ Links ]
45. World Health Organization. World Health Report 2000. Health Systems: Improving Performance. Geneva Switzerland. [Accessed 2009 October]. Available at: http://www.who.int/whr/2000/en/whr00_en.pdf [ Links ]
46. Jonsson B. Changing health environment: the challenge to demonstrate cost-effectiveness of new compounds. Pharmacoeconomics 2004; 22(suppl 4):5-10. [ Links ]
47. Instituto Nacional de Estadística y Geografía (INEGI). Sistema de Cuentas Nacionales. [Accessed 2009 November]. Available at: http://dgcnesyp.inegi.org.mx/cgi-win/bdiecoy.exe/572?s=est&c=12546 [ Links ]
48. Consejo Nacional de Población (CONAPO). Indicadores demográficos básicos 1990-2030. [Accessed 2009 October] Available at: http://www.conapo.gob.mx/index.php?option=com_content&view=article&id=125&Itemid=193. [ Links ]
 Correspondence to autor:
Correspondence to autor:
Silvia Martínez Valverde.
Dr. Márquez 162, Edificio Mundet, col.
Doctores, 06720 Delegación Cuauhtémoc, México, DF, México
E-mail: smartinez@himfg.edu.mx
Received on: March 15, 2011
Accepted on: September 8, 2011


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}