










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkSalud Pública de México
versão impressa ISSN 0036-3634
Salud pública Méx vol.54 no.1 Cuernavaca Jan./Fev. 2012
ORIGINAL ARTICLE
Prevalence of obesity and metabolic syndrome components in Mexican adults without type 2 diabetes or hypertension
Prevalencia de obesidad y componentes del síndrome metabólico en adultos mexicanos sin diabetes tipo 2 o hipertensión arterial
Rosalba Rojas-Martínez, MC, PhDI; Carlos A Aguilar-Salinas, M EspII; Aída Jiménez-Corona, MC, PhDI; Francisco J Gómez-Pérez, M EspII; Simón Barquera, MC, PhDI; Eduardo Lazcano-Ponce, MC, ScDI
IInstituto Nacional de Salud Pública. Cuernavaca, Morelos, México
IIInstituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. México, DF, México
ABSTRACT
OBJECTIVE: To describe the number of Mexican adults with undiagnosed diabetes and arterial hypertension and their association with obesity.
MATERIAL AND METHODS: The study included a sub-sample of 6 613 subjects aged 20 years or more who participated in the 2006 National Health and Nutrition Survey (ENSANUT 2006). Subjects with a previous diagnosis of diabetes or hypertension (n=1 861) were excluded. Prevalences and standard errors were estimated, taking into account the complex sample design.
RESULTS: 6.4 million adults have obesity and undiagnosed impaired fasting glucose. Almost two million more have fasting glucose levels diagnostic for diabetes. As for arterial blood pressure, 5.4 million adults had prehypertension. Another 5.4 million adults had blood pressure levels suggestive of probable hypertension. A total of 21.4 million Mexican adults with obesity had at least one further component of the metabolic syndrome.
CONCLUSIONS: A large proportion of adults with obesity-related metabolic comorbidities remains undiagnosed in Mexico.
Key words: obesity; waist circumference; metabolic syndrome; Mexico
RESUMEN
OBJETIVO: Estimar el número de adultos mexicanos que tienen diabetes o hipertensión arterial no diagnosticadas y el riesgo de tales condiciones asociado a la obesidad.
MATERIAL Y MÉTODOS: Se analiza una submuestra de 6 613 sujetos mayores de 20 años que participaron en la Encuesta Nacional de Salud y Nutrición 2006. Los sujetos con diagnóstico previo de diabetes o hipertensión arterial fueron excluidos (n=1 861). Las prevalencias y errores estándar fueron estimados considerando el diseño complejo de la muestra.
RESULTADOS: 6.4 millones de adultos tienen obesidad y glucemia anormal de ayuno. Casi dos millones más tienen una glucemia de ayuno diagnóstica de diabetes En cuanto a la presión arterial, 5.4 millones tienen prehipertensión. El mismo número de casos tienen valores diagnósticos de hipertensión. Un total de 21.4 millones de adultos con obesidad tienen al menos un componente del síndrome metabólico.
CONCLUSIONES: Un alto porcentaje de los adultos que tienen comorbilidades metabólicas de la obesidad permanecen sin ser diagnosticados en México.
Palabras clave: obesidad; perímetro de cintura; síndrome metabólico; México
Obesity is recognized as a preventable disease that can be treated through the adoption of a healthy lifestyle, including an adequate caloric intake according to each individual's nutritional needs and regular physical activity.1,2 Obesity is also a prominent risk factor for the development of chronic diseases, such as type 2 diabetes3,4 and cardiovascular disease.5 Obesity results from the combination of genetic6 and enviromental7 factors. The prevalence of obesity in adults varies from 10% to 25% in Western European countries and from 20% to 25% in Latin American countries. Those percentages rise to 40% for women from Eastern Europe and Mediterranean countries, as well as for Afro American women.8 American Indians and the populations of Latin America and of certain Pacific Islands (Melanesians, Micronesians, and Polynesians) have the highest prevalences.9 In Latin America, data from surveys carried out in Brazil, Mexico, and some Caribbean countries show that obesity is an increasingly serious public health problem, especially among women.10 In Mexico, several research groups have described obesity prevalence and obesity-related morbidity, as well as the associated risk factors and the outcome of a number of prevention and treatment programs.11-15 The prevalence of obesity in Mexican adults has increased markedly over the years. Data from the 1993 National Survey of Chronic Diseases (ENEC) showed an obesity prevalence of 21.5%.16 Those from the 2000 National Health Survey (ENSA) indicated that 24% of adults suffered obesity.17 Finally, data from the 2006 National Health and Nutrition Survey (ENSANUT 2006) revealed that 30% of adults of both sexes were obese.18
Weight loss and the adoption of a healthy lifestyle have proved to be the best strategy to prevent type 2 diabetes and other chronic non-transmissible diseases. Thus, the identification of cases of obesity or overweight having one or more components of the metabolic syndrome is the first step to design a nationwide program for the prevention of type 2 diabetes. This information is required to assess the resources needed and may be useful for the estimation of future incident diabetes.
The aim of this report is to describe the number of Mexican adults with undiagnosed obesity-related metabolic comorbidities (i.e. diabetes and hypertension) in the ENSANUT 2006. The identification of this group is required because it constitutes the prime target for prevention programs.
Material and Methods
The 2006 National Health and Nutrition Survey (ENSANUT 2006) was designed to collect information about the health and nutrition status of the Mexican population, the prevalence of certain chronic and infectious diseases, and the perception of the population regarding the quality and response of health services. A probability, multistage, stratified, cluster sample design was used. Villages with less than 2 500 inhabitants were considered as rural localities. A total of 47 152 households were visited; data from 45 446 adults aged 20 years or more were gathered through a questionnaire. These subjects were asked about previous physician diagnosis of diabetes, hypertension, cardiovascular disease, and other chronic diseases. Anthropometric measurements were made (weight, height, and waist circumference were obtained, and blood pressure was measured).
A subsample of 6 613 participants was randomly selected in order to have the statistical power to detect conditions (i.e. type 2 diabetes and dyslipidemias) with a prevalence rate equal to or above 8%. The subsample was balanced by geographic region. Sample weights for each participant were calculated in order to estimate the total adult population. Given that the participants who provided blood were in the slightly lower age range, with a higher proportion of women, post-stratification weights were calculated for the final subsample. Taking into account differences of age and gender distribution between the subsample and the 2005 census information, final weights were obtained. The ability of this subsample to be representative of the Mexican population has been assessed and demonstrated in a series of reports.18-21 All individuals with previous physician diagnosis of diabetes or hypertension were excluded; therefore, our study sample was considered to comprise 4 752 adults.
Definitions
Diabetes was defined by a fasting (8-12 hours) plasma glucose ≥ 126 mg/dl. Hypertension was diagnosed when systolic blood pressure was ≥140 mmHg or diastolic blood pressure ≥90 mmHg (mean of two readings with a 5 minute interval between each). Impaired fasting glucose was defined by a fasting plasma glucose of 100-125.9 mg/dl. Pre-hypertension was diagnosed when systolic blood pressure was of 120-139 mmHg or diastolic blood pressure of 80-89 mmHg. Obesity was considered to be present when the body mass index (BMI) (estimated by weight/height2) was ≥30kg/m2. Overweight was defined as a BMI between 25kg/m2 and 29.9 kg/m2. Abdominal obesity was defined by a waist circumference of >102 cm in men and >88 cm in women, according to the American Heart Association/National Heart, Lung and Blood Institute [AHA/NHLBI]),22 and waist circumference >90 cm in men and >80 cm in women, according to the International Diabetes Federation (IDF).23 Hypercholesterolemia was considered to be present when total cholesterol concentrations were ≥200 mg/dl. Hypertriglyceridemia was defined by plasma triglycerides concentrations of ≥ 150 mg/dl. Hypoalphalipoproteinemia was considered to be present when HDL cholesterol concentrations were <40 mg/dl in men and <50 mg/dl in women. The metabolic syndrome was diagnosed using the AHA/NHLBI criteria.22 This requires the presence of at least 3 of the following components: waist circumference ≥102 cm in men and ≥88 cm in women; triglycerides ≥ 150 mg/dl; HDL cholesterol < 40 mg/dl in men and < 50 mg/dl in women; systolic blood pressure ≥ 135 mm Hg or diastolic blood pressure ≥ 85 mm Hg; and a fasting glucose ≥ 100 mg/dl.
Statistical analysis
Prevalences, standard errors, and frequencies were obtained using weighted data and considering the complex sample design. In order to determine the association between diabetes, hypertension and obesity adjusted for the confounding variables, multiple logistic regressions were carried out, including all variables that had a univariate correlation coefficient with a p-value of less than 0.1. Odds ratio and its corresponding 95% confidence interval were obtained as a measure of the association. Statistical analyses were performed using SAS v9.2, considering the complex sample design.
Results
Table I summarizes the characteristics of the study population, which consisted of 4 752 adults representing 41 million Mexican adults aged 20 years or more.
Prevalence of obesity in this study group was 25.2%, being higher in women (29.8%) than in men (20.1%), and in individuals aged 40 years or more (30.8 vs 21.9%). The prevalence of undiagnosed diabetes was 6.5% (8.0% in men and 5.1% in women). Prevalence of undiagnosed hypertension was 17.5% (21% in men and 14.2% in women).
Of the population with obesity, 83.4% lived in urban areas, 49.4% had 6 years or less of schooling and 59.4% were in the lowest deciles of socioeconomic status. Also, 25.3% had hypertriglyceridemia, 23.9% had hypercholesterolemia, and 56.4% showed low levels of HDL cholesterol. In addition, 86.3% had abdominal obesity (according the AHA/NHLBI criteria). Ten percent of the individuals with obesity had blood glucose levels above 126 mg/dl, and 23.9% had undiagnosed arterial hypertension.
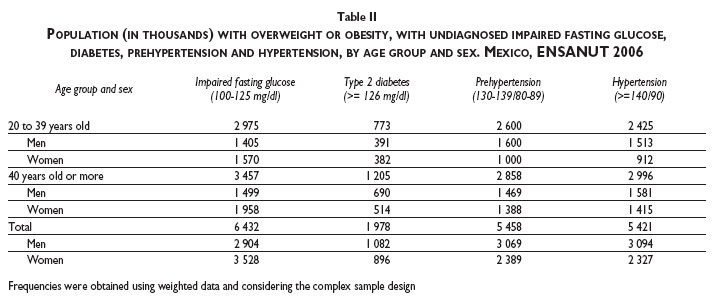
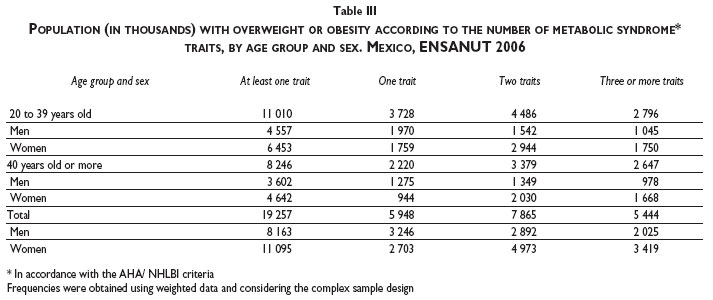
Because ENSANUT 2006 is representative of Mexican adults, we can estimate the number of cases existing nationwide (table II). After excluding the previously diagnosed cases with diabetes and/or arterial hypertension, 6.4 million adults were shown to have obesity and undiagnosed impaired fasting glucose (100-126 mg/dl); the majority was over 40 years old. A further two million individuals, mostly men, have serum glucose levels of 126mg/dl or higher. In regard to arterial blood pressure, 5.4 million adults, the majority of whom were male, had pre-hypertension. Likewise, a further 5.4 million adults had blood pressure levels compatible with arterial hypertension. A total of 19.2 million Mexican adults with obesity had at least one component of the metabolic syndrome; of these, 13.3 million showed two or more components, and 5.4 million had three or more components (table III).
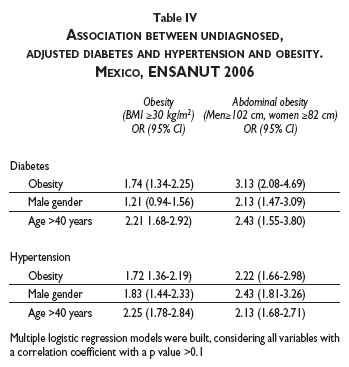
Individuals with obesity had a 74% greater probability of having diabetes compared with non-obese individuals. Likewise, they had a 72% greater probability of having hypertension compared with the non-obese population. Those associations were obtained after adjustment for sex and age (table IV). By using central obesity as an independent variable, we found that the population with abdominal obesity had three times more risk for diabetes and two times more risk of hypertension than individuals without central obesity (table IV).
Discussion
Mexico faces an epidemic of non-transmissible chronic diseases as a result of the increasing prevalence of obesity. This study, which is a secondary analysis of the ENSANUT 2006 survey, shows that a high percentage of persons whose BMI is above 25 kg/m2 have diabetes or hypertension, but have not been diagnosed. This indicates that our health system is not detecting and preventing chronic diseases efficiently, even in those cases in which risk factors are evident. Our data provide evidence that supports the systematic search for diabetes and hypertension in every patient with abdominal adiposity.
Diabetes prevention programs have been shown to be an effective approach to decrease the incidence of type 2 diabetes.24 The intervention includes the adoption of a healthy lifestyle, a diet program and increased physical activity. The efficacy of the intervention heavily depends on inducing weight loss. Several drugs (i.e. metformin) have been shown to delay the onset of the disease, but their use is still debated at population level.25 Diabetes prevention programs can be prescribed in primary care clinics and are relatively inexpensive.26 However, their implementation requires a proper organization of the health services and the identification of the populations at risk. Age, family history and adiposity are the main risk factors for type 2 diabetes.21 These conditions can easily be detected by physicians and health personnel every time a member of the population requests a consultation. Our data show that close to 10 million Mexicans are at risk of developing diabetes or hypertension over the next 10 years. Excess body weight should be used as a screening tool for detecting cases of diabetes and/or high blood pressure. This recommendation is based on the high risk that obese individuals have of developing type 2 diabetes and arterial hypertension. However, a large number of cases remain undiagnosed and as a result do not have the opportunity of participating in a prevention program. Almost two million adults with excess body weight have undiagnosed diabetes. Our data suggest that patients and physicians do not recognize obesity as a criterion for diabetes and arterial hypertension screening. About eight million people in Mexico are obese or overweight and have undiagnosed impaired fasting glucose or diabetes; they must receive medical treatment in order to lower the incidence of new cases of diabetes or to manage hyperglycemia. The same is true for the prevention and/or treatment of arterial hypertension; the target population in this case is close to 11 million individuals. Therefore, our health care system must modify its screening procedures and initiate treatment of these individuals.
Our data will help decision-makers plan and implement diabetes prevention programs. The magnitude of the challenge is considerable. A nationwide training program for primary care physicians is urgently needed to improve their ability to screen for chronic diseases and treat obesity. Resources and medications should be allocated to all primary care clinics to diagnose and manage obesity-related comorbidities. Multidisciplinary teams capable of providing efficient treatment for obesity should be available in every region.27
A limitation of the study is the use of fasting blood glucose levels, a technique employed in field surveys; other parameters are necessary to confirm the diagnosis of diabetes (i.e oral glucose tolerance test or a second fasting plasma glucose value).
In conclusion, a large number of Mexican adults who are at risk of type 2 diabetes and arterial hypertension, based on their body weight, fasting plasma glucose and blood pressure, are currently undiagnosed. The systematic detection of abdominal obesity may be helpful to remedy this problem. Our health care system must modify procedures in order to identify and initiate treatment in these individuals.
References
1. Jakicic JM, Otto AD. Physical activity considerations for the treatment and prevention of obesity. Am J Clin Nutr 2005;82(1 Suppl):226S-229S. [ Links ]
2. Avenell A, Sattar N, Lean M. ABC of obesity. Management: Part I--behaviour change, diet, and activity. BMJ 2006;333:740-743 [ Links ]
3. Carey VJ, Walters EE, Colditz GA, Solomon CG, Willet WC, Rosner BA, et al. Body fat distribution and risk of non-insulin-dependent diabetes mellitus in women. The Nurses' Health Study. Am J Epidemiol 1997;145:614-619. [ Links ]
4. Wild SH, Byrne CD. ABC of obesity. Risk factors for diabetes and coronary heart disease. BMJ 2006;333:1009-1011. [ Links ]
5. Kannel WB, D'Agostino RB, Cobb JL. Effect of weight on cardiovascular disease. Am J Clin Nutr 1996;63:419S-422S. [ Links ]
6. Rankinen T, Zuberi A, Chagnon YC, Weisnagel J, Argyopoulus G, Wats B, et al. The human obesity gene map: the 2005 update. Obesity 2006;14:529-644. [ Links ]
7. Hill JO, Peters JC. Environmental contributions to the obesity epidemic. Science 1998;280:1371-1377. [ Links ]
8. Popkin BM. Does global obesity represent a global public health challenge? Am J Clin Nutr 2011;93:232-233. [ Links ]
9. Popkin BM. Recent dynamics suggest selected countries catching up to US obesity. Am J Clin Nutr 2010;91:284S-288S. [ Links ]
10. Uauy R, Albala C, Kain J. Obesity Trend in Latin American; Transiting from under-to overweight. J Nutr 2001;131:893S-899S. [ Links ]
11. Vazquez-Martínez JL, Gómez-Dantés H, Gómez-García F, Lara Rodríguez MA, Navarrete-Espinosa J, Pérez-Pérez G. Obesity and overweight in IMSS female workers in Mexico City. Salud Publica Mex 2005;47:268-275. [ Links ]
12. Sánchez-Castillo CP, Lara JJ, Villa AR, Aguirre J, Escobar M, Gutiérrez H, et al. Unusually high prevalence rates of obesity in four Mexican rural communities. Eur J Clin Nutr 2001;55:833-840. [ Links ]
13. Williams KK, Stern MP, Gonzalez-Villalpando C. Secular trends in obesity in Mexico City and in San Antonio. Nutr Rev 2004;62:S158-S162. [ Links ]
14. Flores-Huerta S, Acosta-Cázares B, Gutiérerz-Trujillo G. Prevalencia de peso bajo, sobrepeso, obesidad general y obesidad central. Rev Med Inst Mex Segur Soc 2006;44(Supl 1):S55-S62. [ Links ]
15. Arroyo P, Fernández V, Loria A, Pardío J, Laviada H, Vargas L, et al. Obesidad, morfología corporal y presión arterial en grupos urbanos y rurales de Yucatán. Salud Publica Mex 2007;49:274-285. [ Links ]
16. SSA. Encuesta Nacional de Enfermedades Crónicas. México, DF: Secretaria de Salud, 1993 [ Links ]
17. Olaiz G, Rojas R, Barquera S, Shamah T, Aguilar C, Cravioto P, et al. Encuesta Nacional de Salud 2000. La Salud de los Adultos. México: Instituto Nacional de Salud Pública, 2003. [ Links ]
18. Barquera S, Campos-Nonato I, Carrión-Rábago C, Villalpando S, López-Ridaura R, Rojas R, et al. Methodology for the analysis of type 2 diabetes, metabolic syndrome and cardiovascular disease risk indicators in the ENSANUT 2006. Salud Publica Mex 2010;52 Suppl 1:S4-S10. [ Links ]
19. Rojas R, Aguilar-Salinas CA, Jimenez A, Shamah-Levy T, Rauda J, Ávila-Burgos L, et al. Metabolic Syndrome in Mexican adults. Results from the National Health and Nutrition Survey 2006. Salud Publica Mex 2010:52 (supl1) S11-S18. [ Links ]
20. Aguilar-Salinas CA, Gómez Pérez FJ, Rull JA, Villalpando S, Barquera S, Rojas R. Prevalence of dyslipidemias in the 2006 Encuesta Nacional de Salud y Nutrición. Salud Publica Mex 2010:52 (supl1) S44-S53 [ Links ]
21. Gómez-Pérez FJ, Rojas R, Villalpando S, Barquera S, Rull JA, Aguilar-Salinas CA. Prevention of cardiovascular disease based on the modification of low density lipoprotein cholesterol (LDL-C) levels: A huge challenge for the Mexican health system. Salud Publica Mex 2010:52 (supl1) S54-S63 [ Links ]
22. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the Metabolic Syndrome. American Hearth Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005;112:2735-2752. [ Links ]
23. Alberti KG, Zimmet P, Shaw J. The metabolic syndrome: a new worldwide definition. Lancet 2005;366:1059-1062. [ Links ]
24. Harris S, Zinman B. Primary prevention of type 2 diabetes in high-risk populations. Diabetes Care 2000;23:879-881. [ Links ]
25. Alberti KGMM, Zimmet P, Shaw J. International Diabetes Federation: a consensus on type 2 diabetes prevention. Diabet Med 2007;24:451-463. [ Links ]
26. Satterfield D, Volansky M, Caspersen C, Engelgau MM, Bowman BA, Gregg EW, et al. Community-based lifestyle interventions to prevent type 2 diabetes. Diabetes Care 2003; 26:2643-2652. [ Links ]
27. Sassi F. Obesity and the economics of prevention 2010. Paris: Organization for Economic Co-Operation and Development, 2010. [ Links ]
 Correspondence to autor:
Correspondence to autor:
Dr. Carlos A.
Aguilar-Salinas.
Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán.
Vasco de Quiroga 15, col.
Sección XVI. 14000 Tlalpan México, DF, México
E-mail: caguilarsalinas@yahoo.com
Received on: August 24, 2011
Accepted on: October 25, 2011
Declaration of conflict of interests: The authors declare that they have no conflict of interests.


{kind=link}
{kind=link}
{kind=link}