










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.53 no.5 Cuernavaca sep./oct. 2011
ARTÍCULO DE REVISÍON
Alcohol consumption and the risk of breast cancer
Gloria D Coronado, PhDI; Jeannette Beasley, PhDII; Jennifer Livaudais, PhCII
IKaiser Permanente Center for Health Research. Portland, OR, USA
IICancer Prevention Program, Fred Hutchinson Cancer Research Center. Seattle WA, USA
ABSTRACT
Epidemiologic studies addressing the association of alcohol consumption with breast cancer consistently suggest a modest association and a dose-response relationship. The epidemiologic evidence does not point to a single mechanism to explain the association, and several mechanisms have been proposed. Alcohol consumption is shown to increase levels of endogenous estrogens, known risk factors for breast cancer. This hypothesis is further supported by data showing that the alcohol-breast cancer association is limited to women with estrogen-receptor positive tumors. Products of alcohol metabolism are known to be toxic and are hypothesized to cause DNA modifications that lead to cancer. Recent research has focused on genes that influence the rate of alcohol metabolism, with genes that raise blood concentrations of acetaldehyde hypothesized to heighten breast cancer risk. Mounting evidence suggests that antioxidant intake(e.g.folate)mayreducealcohol-associatedbreast cancer risk, because it neutralizes reactive oxygen species, a second-stage product of alcohol metabolism. Diets lacking sufficient antioxidant intake, as a result, may further elevate the risk of breast cancer among alcohol consumers. Given that alcohol consumption is increasing worldwide and especially among women in countries of rapid economic growth, a greater understanding of the mechanisms underlying the known alcohol-breast cancer association is warranted.Avoiding overconsumption of alcohol is recommended, especially for women with known risk factors for breast cancer.
Keywords: breast cancer; alcohol consumption; risk factors
RESUMEN
Diversos estudios epidemiológicos muestran la asociación del consumo de alcohol con el cáncer de mama de forma consistente, lo que sugiere una modesta asociación, y una relación de dosis-respuesta.La evidencia no apunta a un mecanismo único para explicar la asociación y varios mecanismos han sido propuestos. El consumo de alcohol incrementa los niveles endógenos de estrógeno, un riesgo conocido para cáncer de mama. Esta hipótesis es apoyada por información que muestra que la asociación entre el alcohol y el cáncer de mama está limitada a mujeres con tumores con receptores positivos de estrógeno. Es conocido que los derivados de la metabolización del alcohol son tóxicos, y se ha pensado que causan modificaciones en el DNA que llevan al cáncer. La investigación reciente se ha enfocado en genes que influencian la velocidad con la que se metaboliza el alcohol, y elevan las concentraciones de acetaldehído que se piensa puede aumentar el riesgo de cáncer de mama. La evidencia actual sugiere que la ingesta de antioxidantes (e.g. folato) puede reducirelriesgode cáncer asociadoalalcohol,porque neutraliza las especies reactivas de oxígeno, un producto de la segunda etapa del metabolismo del alcohol. Las dietas con ingesta insuficiente de antioxidantes,como resultado de esto, pueden elevar el riesgo de cáncer entre los consumidores de alcohol.Dado que el consumo de alcohol está incrementando en todo el mundo, especialmente en mujeres de países con rápido crecimiento económico, un mejor entendimiento de los mecanismos subyacentes a la asociación del cáncer de mama y el alcohol es necesario. Evitar el consumo excesivo es recomendado, especialmente para mujeres con factores de riesgo conocidos para cáncer de mama.
Palabras clave: cáncer demama;consumo de alcohol;factores de riesgo
Evidence from a substantial number of epidemiologic and experimental studies suggests that alcohol consumption is a modest risk factor for breast cancer. Worldwide consumption of alcohol has increased substantially in the past two decades, and the increase has been particularly evident among women in countries of rapid economic growth.1 This article describes the strength of the evidence for the association between alcohol and breast cancer, the primary mechanisms that have been proposed to explain the association, and alcohol consumption patterns worldwide.
Data from a variety of epidemiologic studies suggest that chronic alcohol consumption even in moderate amounts increases a woman's risk for breast cancer.2-4 The vast majority of the case-control studies (84% of 69)and cohort studies (76% of 21) published to-date haveshown a positive association between alcohol consumption and breast cancer.5 Nevertheless, the magnitudeof the association is modest:6-10 A meta-analysis of data from over 40 reports and 41 477 incident cases of breastcancer estimate that compared to non-drinkers, women who consumed one drink per day (defined as 12g) had a 10% [95% Confidence Interval (CI)= 6%-14%] increased risk of breast cancer.11 While most studies have reportedconsistent findings, inconsistencies are thought to be dueto the low magnitude of the association, low consumption patterns, and/or the tendency to underreport alcohol consumption.
Epidemiologic data further suggest that consumption of larger amounts of alcohol is associated with a higher risk of breast cancer. Prospective follow-up for an average of 7.3 years of 1.3 million women showed that of women who reported recent alcohol consumption, a 12% (95% CI=9% to 14%) elevation in breast cancer risk was observed for each additional drink (defined as 10g).12 These findings are consistent with data from a pooled analysis of cohort studies suggesting a dose-response relationship.9
The number of cases of breast cancer that can be attributed to alcohol consumption varies by geographic region and depends upon consumption patterns and the prevalence of breast cancer within a given region. In the United States (US), an estimated 2.1 to 4.0% of breast cancers are primarily due to alcohol consumption,5,13 accounting for 14 000 to 27 000 new cases per year.13 In countries with higher average consumption, the attributable risk is much higher; in Italy for example, the attributable risk is estimated to be 10%.14
Few studies have examined the relationship between alcohol consumption and specific subtypes of breast cancer, although there is growing recognition that breast cancer is a heterogeneous disease and that different subtypes are associated with unique risk factors, tumor characteristics, and prognoses. One study found differences in the association by tumor histology, noting a 1.8-fold (95%CI: 1.3 – 2.5) excess risk for lobular cancers and only a 1.2-fold (95%CI: 0.9 – 1.4) excess risk for ductal cancers;15 one other small study reported similar findings.16 A limited number of studies have examined the known alcohol-breast cancer association by tumors according to the presence of estrogen and/or progesteronereceptors; though the results have been contradictory.16-19 Future research is needed to further elucidate differences in the association by tumor characteristics.
Evidence for whether the strength of the alcoholbreast cancer association varies by stage of breast cancer detection is lacking. Alimited number of epidemiologic investigations have reported that individuals who consume alcohol are more likely to experience late stage detection of breast cancer. High consumers of alcohol, however, are thought to be less likely to receive regular screening for early breast cancer detection, a factor known to result in delayed detection of disease. Other studies have linked alcohol consumption to heightened risk of breast cancer recurrence,7 although this has been the subject of relatively few published studies.
The strength of the association between alcohol consumption and breast cancer is similar for pre-menopausal and post-menopausal women.8,20 While this may weaken the rationale for a hormone-based mechanism, data from controlled feeding studies suggests that alcohol intake leads to immediate elevations in levels of circulating endogenous estrogens (see Proposed Mechanism 1: Effects on estrogen levels and estrogen receptors). Further research in this area is warranted.
There is limited data on whether consumption patterns (i.e. sporadic consumption vs. regular consumption) impact the magnitude of breast cancer risk. Some reports suggest that regular (as low as 1-2 drinks per day) and not sporadic consumption contributes to the increased risk.8 Nevertheless, data have shown a consistent association across type of alcohol consumed (e.g. wine, beer, hard liquor).20-22 Evidence linking breast cancer to the consumption of alcohol during specific time periods of life has been inconsistent; however, there is some evidence that delaying the onset of alcohol consumption can reduce the risk of breast cancer.4,23
Proposed mechanisms underlying the alcohol-breast cancer association
Despite consistent evidence linking alcohol consumption to breast cancer, to date the mechanisms explaining the relationship are unclear. Several mechanisms have been hypothesized; these include effects on estrogen levels and estrogen receptors,24 release of carcinogenic metabolites of alcohol, such as acetaldehyde or reactive oxygen species,25 and decreased absorption of essential nutrients.26 In this section, we describe the strength of evidence for each of these proposed mechanisms
Proposed mechanism 1: Effects on estrogen levels and estrogen receptors
Association with estrogen receptor-positive (ER+) tumors
Several epidemiologic studies have shown an association between alcohol and breast cancer exclusively for tumors that express the estrogen receptor, i.e. estrogen receptor-positive (ER+ tumors).15-17,27 Data analyzed from two case control studies of breast cancer cases from the LosAngeles Tumor Registry and neighborhood controls found that the increased risk of breast cancer among postmenopausal women associated with alcohol intake was restricted to ER+/progesterone receptorpositive (PR+) breast cancer.17 The authors concluded that alcohol may preferentially increase the risk of ER+/PR+ breast cancer in postmenopausal women, as a high level of daily alcohol consumption (>27 g/day) was associated with an odds ratio of 1.75 (95% CI 1.14-2.71) for this subtype. Alcohol intake was not associated with other hormone receptor subtypes of breast cancer.17
Similarly, a population-based case control study in western Washington State including women ages 65-79 years found that ever-users of alcohol had an increased risk of ER+/PR+ tumors relative to never-users (OR=1.3, 95% CI 1.1-1.7). No association was observed between alcohol intake and ER+/PR- or ER-/PR- tumors.15 The authors concluded that alcohol was more strongly associated with hormone-receptor positive tumors than with other types of breast cancer, consistent with an underlying hormonal basis for the association between alcohol use and breast cancer.15
Results from the Swedish mammography cohort were similar. The cohort included 51 847 postmenopausal women and 1 188 invasive breast cancer cases and alcohol consumption was found to be associated with increased risk of ER+ tumors, regardless of PR status.27 Compared to non-drinkers, the relative risk for ER+/PR+ breast cancer for those drinking >10 g/day was equal to 1.35 (95% CI 1.02-1.80) and the relative risk for ER+/PR- breast cancer was 2.36 (95% CI 1.56-3.56). No association was observed between alcohol intake and ER- tumors. Of note was a significant interaction between alcohol intake and the use of postmenopausal hormones on risk for ER+/PR+ tumors.27
In contrast to these findings, several studies have found no difference in the association between alcohol intake and breast cancer according to ER status.19,28-30 However, critics of these studies suggest that they may have been limited in their ability to detect differences by tumor subtype due to small sample size19,29-30 or nonstandardized methods for measuring ER status.28
Potential pathways
Alcohol intake has been associated with increased levels of circulating endogenous estrogen,8,31 which may directly contribute to elevated risk for breast cancer. Alcohol increases hormone levels, particularly estrone sulfate and dehydroepiandrosterone (DHEAS), and this is believed to be one of the mechanisms underlying the association between alcohol and breast cancer. In a controlled feeding study of 51 postmenopausal women not taking hormone therapy, when women consumed 8 weeks of 15 or 30g of alcohol per day, they had increased concentrations of estrone sulfate (increase of 7.5% and 10.7% respectively). DHEAS concentrations also increased by 5.1% and 7.5% respectively, relative to levels when women consumed placebo.31
Among premenopausal women, moderate intake of alcohol can decrease menstrual cycle variability and increase the frequency of long menstrual cycles, increasing exposure to endogenous estrogens.8 Blood levels of the reactive ethanol metabolite acetaldehyde are elevated during the high estradiol phase of menstrual cycle among women who drink, and particularly among women who drink and use oral contraceptive pills. Among postmenopausal women not using hormone therapy, moderate alcohol intake can lead to increased blood estrogen or androgen levels, and among postmenopausal women using hormone therapy, there is an even more pronounced effect of alcohol on blood estradiol levels.8
Alcohol may affect breast cancer risk through the ER signaling pathways as the elevated levels of intracellular estrogens resulting from alcohol intake may act through the estrogen receptor to promote breast tumor growth31 In human breast cancer cells, ethanol stimulates cell proliferation and enhances ER-alpha and aromatase expression, supporting a role for ER signaling in the proliferation of breast cancer cells. Ethanol has been shown to stimulate proliferation of ER+ but not ER- breast tumors in breast cancer cells in culture,8,32 causing a 10-to 15-fold increase in transcriptional activity of liganded estrogen receptors. In addition to increasing the transcriptional activity of ER alpha, ethanol may also affect breast cancer risk by down-regulating the expression of the tumor suppressor gene BRCA1, an inhibitor of ER-alpha activity.32,33
Proposed mechanism 2: Alcohol metabolism
Another proposed mechanism underlying the relationship between alcohol consumption and breast cancer is carcinogenesis resulting from alcohol metabolism. The metabolism of alcohol occurs through a two stage process. During the first stage, acetaldehyde is a primary product. This and other products of alcohol metabolism are known to induce DNA modifications, by causing strand deletions, chromosomal aberrations, or generating protein adducts. Once DNA modifications occur, acetaldehyde may promote breast tumorigenesis by interfering with DNA repair mechanisms. Several alcohol metabolism genes have been explored for their association with breast cancer. Laboratory and epidemiologic studies have examined genes that result in the rapid metabolism of alcohol to acetaldehyde (during the first stage of metabolism) and genes that result in slow metabolism of acetaldehyde to acetate (during the second stage of metabolism); both are thought to raise blood concentrations of acetaldehyde and result in a higher risk for DNA modifications that can lead to cancer.
The first stage of alcohol metabolism is characterized by the conversion of ethanol to acetaldehyde, which is facilitated by two enzymes: alcohol dehydrogenase (ADH) and cytochrome P4502E1. Nearly 80% of alcohol is metabolized by ADH.34 During the second stage of metabolism, acetaldehyde is converted to acetate by three enzymes: aldehyde dehydrogenase (ALDH), xanthine oxidoreductase (XOR), and aldehyde oxidase (AOX).33 Acetate is then excreted in the urine.
Both acetaldehyde and free radicals produced in the second stage of metabolism have been implicated for their role in alcohol-associated carcinogenesis. Acetaldehyde is highly toxic and is shown in several laboratory studies to cause DNA modifications through the generation of protein adducts, causing DNA crosslinkage, chromosomal aberrations, and DNA point mutations33,35-37 Importantly, acetaldehyde is thought to interfere with DNArepair machinery,5 further increasing the risk of cancer once modifications of the DNA have occurred. It does this by inhibiting enzymes important for the repair of protein adducts and the repair of chromosomal breaks.1,33 Similarly, free radicals are thought to lead to carcinogenesis by causing DNA damage, strand breakage and base alterations.33
Levels of acetaldehyde and alcohol-associated free radicals are influenced by levels of enzymes responsible for both their production and for their break-down. For this reason, recent studies have examined the efficiency of alcohol metabolism and genetic factors related to the efficiency. Specifically, alleles for ADH and ALDH have been examined for their relationship to levels of acetaldehyde37-39 and alleles for glutathione-S-transferase genes, GSTM1 and GSTT1, have been examined for their relationship to levels of free radicals.40 Moreover, genes that influence the process by which DNA modifications are repaired have been examined for their relationship to alcohol-associated breast cancer; one candidate is XRCC1 399Q.33 Nevertheless, there remain relatively few published reports on this topic.
One important genetic polymorphism encodes for ADH, the primary enzyme responsible for the oxidation of ethanol to acetaldehyde and thereby plays a rate-limiting role in the metabolic pathway. Data from experimental studies show that polymorphisms in ADH influence the rate of alcohol metabolism, such that individuals having the ADH1-13, ADH1-23, and ADH2-23 allele are considered fast, intermediate, and slow metabolizers. Among these, fast metabolizers are thought to experience the greatest risk of breast cancer, likely due to their prolonged exposure to acetaldehyde. Data from three studies support this hypothesis. One study used data from 1047 breast cancer cases and 1101 controls that were part of the Long Island Breast Cancer Study and examined the strength of the alcohol-breast cancer association among fast, intermediate and slow metabolizers (as determined by ADH genotyping).37 Analysisfrom the study showed that among fast metabolizers the odds of breast cancer associated with an average lifetime consumption of 15 -30 grams of alcohol per day (the equivalent of 1 to 2 drinks per day) was two-fold (OR: 2.0; 95% CI: 1.1 – 3.5) higher than for non drinkers. By comparison, the relative odds of breast cancer for intermediate and slow metabolizers associated with similar average lifetime consumption of alcohol was 1.5 (OR: 1.5; 95%CI: 0.9 – 2.4) and 1.3 (OR: 1.3; 95%CI: 0.5 – 3.5), respectively. Data from two additional studies suggest a 1.8-fold higher risk of breast cancer among women with the fast metabolizing alleles.38-39 Terry and colleagues further demonstrate that the excess risk was more pronounced among pre-menopausal versus post-menopausal women.37 Freudenheim et al. reported a similar finding; specifically, premenopausal women with the ADH1-13 allele who had higher alcohol intake were over 3.5 times likely to develop breast cancer, compared to those with lower alcohol intake.39 Among post-menopausal women with the ADH1-13 allele, the relative odds of developing breast cancer were 1.2 among those with higher compared to lower levels of alcohol consumption. These data suggest a possible gene-environment interaction.
As noted above, there is consistent though limited evidence that genetic polymorphisms in regions of the genome responsible for acetaldehyde generation are associated with an elevated risk of breast cancer. Scientists have further hypothesized genetic polymorphisms in the regions responsible for acetaldehyde detoxification may also influence breast cancer risk. Seitz et al. compared blood acetaldehyde levels among individuals who were homozygous for the ALDH allele (ALDH2-2) to those who were heterozygous (ALDH2-1). The findings suggested that those with the homozygous allele had levels of acetaldehyde that were 6 to 20 times higher than among heterozygous individuals. The elevated level of acetaldehyde among homozygous individuals is thought to cause "flush syndrome" and may deter excess alcohol consumption.41
During the second stage of metabolisms, the enzymes that catalyze acetaldehyde to form acetate, XOR and AOX, can generate reactive oxidative species (ROS), including superoxide anion (O2*-), hydroxyl radical (*OH), and hydrogen peroxide (H2O2). ROS have been shown to cause DNAdamage, strand breakage and base alterations.33 Notably, *OH modifications are thought to be 8- to 17-fold higher in breast cancer DNA than in normal tissue DNA.42 Moreover, *OH modified DNA has been directly linked to the progression of human breast cancer and has been proposed as a prognostic indicator of breast disease.42 Efficient or "fast" metabolizers of acetaldehyde may significantly elevate the risk for ROS-associated DNA modifications.42 This may explain the reduction in breast cancer incidence among individuals with diets enriched in antioxidants (see Proposed mechanism 3: Alcohol metabolism and nutrient intake).
Because of the role of ROS and other alcohol byproducts in carcinogenesis, research has examined polymorphisms in genetic loci associated with the metabolisms of these by-products. The ability to metabolize reactive lipid peroxidases, free radicals, andcytotoxic products of alcohol metabolism is thought to be influenced by glutathione-S-transferase genes (GSTM1 and GSTT1); Park and colleagues report that alcohol-consuming pre-menopausal women lackingthese genes were at a 5.3-fold greater risk for breast cancer, compared to women having these genes.40 Further data on the role of genetic polymorphisms in the metabolism of alcohol are needed.
Polymorphisms in DNA repair genes may also produce excess risk of breast cancer, especially when combined with alcohol consumption.33 One candidate gene is XRCC1 399Q, which is involved in DNA base excision repair. Further research is needed to elucidate a possible gene-environment interaction.
Proposed mechanism 3: Alcohol metabolism and nutrient intake
The direct association between alcohol consumption and breast cancer risk may be modified, at least in part, by alcohol's interference with the absorption of folate,5 a micronutrient known to be important in DNA synthesis and repair. Data from a cohort study of over 35 000 postmenopausal women show that those who consumed 1272 or more dietary folate equivalents per day had a 22% reduction in breast cancer risk, compared to women who consumed less than 345 dietary equivalents.43 In the U.S. and Canada, mandatory fortification programs started in 1998; this, combined with a higher prevalence of vitamin supplementation,43 reduces folate deficiency in the population. Arandomized, controlled trial of combined folate (2.5 mg), Vitamin B6 (50 mg), and Vitamin B12 (1mg) supplementation compared to placebo among women at high risk of cardiovascular disease reported no overall association between supplementation and invasive breast cancer (HR 0.83, 95% CI 0.60-1.14, P=0.24).44 Vitamin B12, along with riboflavin and Vitamin B6, are cofactors in the folate pathway converting homocysteineinto methionine for DNA methylation. Prior research has also reported no significant associations between Vitamin B6 and breast cancer risk among premenopausal women45 and postmenopausal women.43,46,47
It has been observed that the magnitude of the alcohol–breast cancer association differs by levels of folate consumption.48 Previous epidemiologic studies have suggested that low levels of folate, and other onecarbon methyl group donors such as vitamin B12,49 may form part of the pathway by which alcohol elevates the risk of breast cancer.48,50-52 Similarly, higher intake of folate or multivitamin use has been shown to attenuate the alcohol-breast cancer association.43 Since alcohol is a known folate antagonist and could therefore interfere with DNA repair, several studies have investigated joint associations between alcohol and folate and breast cancer, as recently reviewed.53 The majority of cohort studies provide evidence to support a protective effect of folate on breast cancer among women who consume alcohol.48,50-52 However, data from the Women's Health Initiative Observational study53 as well as other large cohort studies54-55 reported no evidence for an attenuation of risk in postmenopausal women.
Types of alcohol and consumption patterns
Major types of alcohol include beer, wine, and liquor. The limited evidence available suggests consistency in the magnitude of the alcohol-breast cancer association across type of alcohol consumed. Nevertheless, the amount of alcohol within a serving varies by source. The United States Department of Agriculture (USDA) reports the mean alcohol content of a serving of beer is 13.9g, wine 15.4g, and liquor 14g (serving defined as 12 oz beer, 5 oz wine, 1.5 oz 80 proof liquor).56 The actual amount varies by type: the range for beer is 3 to7%, wine 9 to 15%, and liquor 35 to 50% by volume.57
Because of this variability, the definition of an alcoholic drink often varies across studies, ranging from ~10-15 grams of alcohol; thus some authors report total grams of ethanol for comparison purposes.
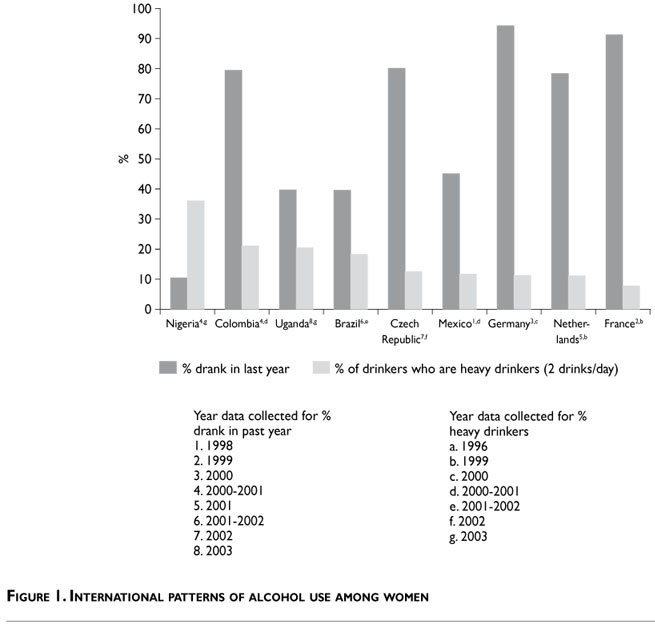
Data from the World Health Organization suggest that an estimated 2 billion people worldwide consume alcoholic beverages.58 Alcohol consumption patterns among women vary substantially by geographic region (Figure 1). According to data from the World Health Organization, having ever drunk alcohol in the past year was highest in Germany, France, the Czech Republic, and the Netherlan Columbia. Among those who drank alcohol in the past year, the proportion of heavy drinkers, as defined by drinking two or more servings of alcohol (>20g) a day, was highest in Nigeria, suggesting relatively high consumption among a smaller proportion of consumers.58 Notably, consumption of alcohol is reported to be rising in many countries, especially among women in regions of rapid economic growth.59 Within a given country, drinking patterns vary by subpopulations and across different regions; it is generally believed that those of low education and income consume more alcohol than those of high education and income, resulting in economic disparities in alcohol-associated breast cancer.60
Alcohol consumption behaviors are thought to be influenced by migration. Prior epidemiologic research suggests that the proportion of Hispanic women born in the U.S. who drink alcohol is lower than for non-Hispanic whites (60.3% vs. 40.1% report no alcohol consumption, respectively), and the proportion is even lower among women who are recent immigrants (68.9% abstained from alcohol).61
Conclusion
Alcohol consumption is a modifiable risk factor for breast cancer; thus several behavioral recommendations have been offered. Given the dose-response relationship between alcohol consumption and breast cancer, recommendations generally focus on limiting overconsumption of alcohol. Nevertheless, the widely publicized cardiovascular benefit to moderate alcohol consumption suggests that the risks and benefits of alcohol consumption should be weighed in making individual lifestyle choices.59 Women who are low to moderate consumers of alcohol should consider their overall risk of chronic disease.
Nevertheless, some general recommendations regarding consumption practices should be followed. While definitions vary for what constitutes a low or moderate level of consumption, it is generally recommended that excess consumption be avoided. This is generally thought to amount to three or more drinks per day. Lower intake is recommended for women who have known risk factors for breast cancer; for these women Poschl et al. suggests avoiding regular consumption and that consumption be limited to no more than twice weekly in moderate doses (10-20g for women).5
In the past two decades, a tremendous amount of research has addressed the association between alcohol consumption and breast cancer. Nevertheless, more research is needed. Future research to elucidate the interaction between alcohol consumption and other breast cancer risk factors and to explain the role of genetic factors in alcohol metabolism will advance the field. Such research can lead to improved health recommendations and more informed decisions about lifestyle and risk, by placing alcohol into a broader context of interactions with other choices.33 In addition, further research can inform prevention strategies targeting high-risk individuals and communities.
Declaration of conflict of interests: The author declares not to have conflict of interests.
References
1. Seitz HK, Simanowski UA.Alcohol and carcinogenesis.Ann Rev Nutr 1988(8):99-119. [ Links ]
2. Rohan TE, Jain M, Howe GR, Miller AB.Alcohol consumption and risk of breast cancer: a cohort study. Cancer Causes Control 2000;11(3):239-247. [ Links ]
3. Bowlin SJ, Leske MC,Varma A, Nasca P,Weinstein A, Caplan L. Breast cancer risk and alcohol consumption: results from a large case-control study. Int J Epidemiol 1997;26(5):915-923. [ Links ]
4. Colditz GA. Epidemiology of breast cancer. Findings from the nurses' health study. Cancer 1993;71(4 Suppl):1480-1489. [ Links ]
5. Poschl G, Stickel F,Wang XD, Seitz HK.Alcohol and cancer: genetic and nutritional aspects. Proc Nutr Soc 2004;63(1):65-71. [ Links ]
6. Longnecker MP.Alcoholic beverage consumption in relation to risk of breast cancer: meta-analysis and review. Cancer Causes Control 1994;5(1):73-82. [ Links ]
7. Singletary KW, Frey RS,Yan W. Effect of ethanol on proliferation and estrogen receptor-alpha expression in human breast cancer cells. Cancer Lett 2001;165(2):131-137. [ Links ]
8. Singletary KW, Gapstur SM.Alcohol and breast cancer: review of epidemiologic and experimental evidence and potential mechanisms. JAMA 2001;286(17):2143-2151. [ Links ]
9. Smith-Warner SA, Spiegelman D,Yaun SS, van den Brandt PA, Folsom AR, Goldbohm RA, et al.Alcohol and breast cancer in women: a pooled analysis of cohort studies. JAMA 1998;279(7):535-540. [ Links ]
10. Wiseman M.The second World Cancer Research Fund/American Institute for Cancer Research expert report. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Proc Nutr Soc 2008;67(3):253-256. [ Links ]
11. Ellison RC, Zhang Y, McLennan CE, Rothman KJ. Exploring the relation of alcohol consumption to risk of breast cancer.Am J Epidemiol 2001;154(8):740-747. [ Links ]
12. Allen NE, Beral V, Casabonne D, Kan SW, Reeves GK, Brown A, et al. Moderate alcohol intake and cancer incidence in women. J Natl Cancer Inst 2009;101(5):296-305. [ Links ]
13.Tseng M,Weinberg CR, Umbach DM, Longnecker MP. Calculation of population attributable risk for alcohol and breast cancer (United States). Cancer Causes Control 1999;10(2):119-123. [ Links ]
14. Mezzetti M, La Vecchia C, Decarli A, Boyle P,Talamini R, Franceschi S. Population attributable risk for breast cancer: diet, nutrition, and physical exercise. J Natl Cancer Inst 1998;90(5):389-394. [ Links ]
15. Li CI, Malone KE, Porter PL,Weiss NS,Tang MT, Daling JR.The relationship between alcohol use and risk of breast cancer by histology and hormone receptor status among women 65-79 years of age. Cancer Epidemiol Biomarkers Prev 2003;12(10):1061-1066. [ Links ]
16. Nasca PC, Liu S, Baptiste MS, Kwon CS, Jacobson H, Metzger BB. Alcohol consumption and breast cancer: estrogen receptor status and histology. Am J Epidemiol 1994;140(11):980-988. [ Links ]
17. Enger SM, Ross RK, Paganini-Hill A, Longnecker MP, Bernstein L. Alcohol consumption and breast cancer oestrogen and progesterone receptor status. Br J Cancer 1999;79(7-8):1308-1314. [ Links ]
18. Gapstur SM, Potter JD, Drinkard C, Folsom AR. Synergistic effect between alcohol and estrogen replacement therapy on risk of breast cancer differs by estrogen/progesterone receptor status in the Iowa Women's Health Study. Cancer Epidemiol Biomarkers Prev 1995;4(4):313-318. [ Links ]
19. Yoo KY,Tajima K, Miura S,Takeuchi T, Hirose K, Risch H, et al. Breast cancer risk factors according to combined estrogen and progesterone receptor status: a case-control analysis.Am J Epidemiol 1997;146(4):307-314. [ Links ]
20. Petri AL,Tjonneland A, Gamborg M, Johansen D, Hoidrup S, Sorensen TI, et al.Alcohol intake, type of beverage, and risk of breast cancer in pre- and postmenopausal women.Alcohol Clin Exp Res 2004;28(7):1084-1090. [ Links ]
21.Terry MB, Zhang FF, Kabat G, Britton JA,Teitelbaum SL, Neugut AI, et al. Lifetime alcohol intake and breast cancer risk.Ann Epidemiol 2006;16(3):230-240. [ Links ]
22. Newcomb PA, Nichols HB, Beasley JM, Egan K,Titus-Ernstoff L, Hampton JM, et al. No difference between red wine or white wine consumption and breast cancer risk. Cancer Epidemiol Biomarkers Prev 2009;18(3):1007-1010. [ Links ]
23. Stevens RG, Hilakivi-Clarke L.Alcohol exposure in utero and breast cancer risk later in life.Alcohol Alcohol 2001;36(3):276-277. [ Links ]
24. Mahabir S, Baer DJ, Johnson LL, Dorgan JF, Campbell W, Brown E, et al. The effects of moderate alcohol supplementation on estrone sulfate and DHEAS in postmenopausal women in a controlled feeding study. Nutr J 2004;3:11. [ Links ]
25. Wiseman MJ.The World Cancer Research Fund Expert Report: the next steps. IARC Sci Publ 2002;156:523-524. [ Links ]
26. Thomas SM, Fick AC.Women's health. Part II: Individual, environmental and economic factors affecting adherence to recommended screening practices for breast cancer. J La State Med Soc 1995;147(4):149-155. [ Links ]
27. Suzuki R,Ye W, Rylander-Rudqvist T, Saji S, Colditz GA,Wolk A. Alcohol and postmenopausal breast cancer risk defined by estrogen and progesterone receptor status: a prospective cohort study. J Natl Cancer Inst 2005;97(21):1601-1608. [ Links ]
28. Cotterchio M, Kreiger N,Theis B, Sloan M, Bahl S. Hormonal factors and the risk of breast cancer according to estrogen- and progesterone-receptor subgroup. Cancer Epidemiol Biomarkers Prev 2003;12(10):1053-1060. [ Links ]
29. Huang WY, Newman B, Millikan RC, Schell MJ, Hulka BS, Moorman PG. Hormone-related factors and risk of breast cancer in relation to estrogen receptor and progesterone receptor status.Am J Epidemiol 2000;151(7):703-714. [ Links ]
30. Potter JD, Cerhan JR, Sellers TA, McGovern PG, Drinkard C, Kushi LR, et al. Progesterone and estrogen receptors and mammary neoplasia in the Iowa Women's Health Study: how many kinds of breast cancer are there? Cancer Epidemiol Biomarkers Prev 1995;4(4):319-326. [ Links ]
31. Dorgan JF, Baer DJ,Albert PS, Judd JT, Brown ED, Corle DK, et al. Serum hormones and the alcohol-breast cancer association in postmenopausal women. J Natl Cancer Inst 2001;93(9):710-715. [ Links ]
32. Fan S, Meng Q, Gao B, Grossman J,Yadegari M, Goldberg ID, et al. Alcohol stimulates estrogen receptor signaling in human breast cancer cell lines. Cancer Res 2000;60(20):5635-5639. [ Links ]
33. Dumitrescu RG, Corarla I. Understanding breast cancer risk - where do we stand in 2005? J Cell Mol Med;9(1):208-221. [ Links ]
34. American Institute for Cancer Research. Food, Nutrition and the Prevention of Cancer:A Global Perspective.Washington, DC:American Institute for Cancer Research, 1997. [ Links ]
35. Garro AJ, Lieber CS.Alcohol and cancer.Annu Rev Pharmacol Toxicol 1990;30:219-249. [ Links ]
36. Homann N, Jousimies-Somer H, Jokelainen K, Heine R, Salaspuro M. High acetaldehyde levels in saliva after ethanol consumption: methodological aspects and pathogenetic implications. Carcinogenesis 1997;18(9):1739-1743. [ Links ]
37. Terry MB, Gammon MD, Zhang FF, Knight JA,Wang Q, Britton JA, et al.ADH3 genotype, alcohol intake and breast cancer risk. Carcinogenesis 2006;27(4):840-847. [ Links ]
38. Coutelle C, Hohn B, Benesova M, Oneta CM, Quattrochi P, Roth HJ, et al. Risk factors in alcohol associated breast cancer: alcohol dehydrogenase polymorphism and estrogens. Int J Oncol 2004;25(4):1127-1132. [ Links ]
39. Freudenheim JL,Ambrosone CB, Moysich KB,Vena JE, Graham S, Marshall JR, et al.Alcohol dehydrogenase 3 genotype modification of the association of alcohol consumption with breast cancer risk. Cancer Causes and Control 1999;10:369-377. [ Links ]
40. Park SK,Yoo KY, Lee SJ, Kim SU,Ahn SH, Noh DY, et al.Alcohol consumption, glutathione S-transferase M1 and T1 genetic polymorphisms and breast cancer risk. Pharmacogenetics 2000;10(4):301-309. [ Links ]
41. Seitz HK, Stickel F. Molecular mechanisms of alcohol-mediated carcinogenesis. Nat Rev Cancer 2007;7(8):599-612. [ Links ]
42.Wright RM, McManaman JL, Repine JE.Alcohol-induced breast cancer: a proposed mechanism. Free Radical Biology and Medicine 1999;26(3/4):348-354. [ Links ]
43. Maruti SS, Ulrich CM,White E. Folate and one-carbon metabolism nutrients from supplements and diet in relation to breast cancer risk.Am J Clin Nutr 2009;89(2):624-633. [ Links ]
44. Zhang SM, Cook NR,Albert CM, Gaziano JM, Buring JE, Manson JE. Effect of combined folic acid, vitamin B6, and vitamin B12 on cancer risk in women: a randomized trial. JAMA 2008;300(17):2012-2021. [ Links ]
45. Cho E, Holmes M, Hankinson SE,Willett WC. Nutrients involved in one-carbon metabolism and risk of breast cancer among premenopausal women. Cancer Epidemiol Biomarkers Prev 2007;16(12):2787-2790. [ Links ]
46. Lajous M, Lazcano-Ponce E, Hernandez-Avila M,Willett W, Romieu I. Folate, vitamin B(6), and vitamin B(12) intake and the risk of breast cancer among Mexican women. Cancer Epidemiol Biomarkers Prev 2006;15(3):443-448. [ Links ]
47. Lajous M, Romieu I, Sabia S, Boutron-Ruault MC, Clavel-Chapelon F. Folate, vitamin B12 and postmenopausal breast cancer in a prospective study of French women. Cancer Causes Control 2006;17(9):1209-1213. [ Links ]
48. Baglietto L, English DR, Gertig DM, Hopper JL, Giles GG. Does dietary folate intake modify effect of alcohol consumption on breast cancer risk? Prospective cohort study. BMJ 2005;331(7520):807. [ Links ]
49. Park HM, Shin SJ, Choi DH, Oh D, Lee S, Kim NK.Association between folate metabolism-related gene polymorphisms and methylation of p16(INK4A) and hMLH1 genes in spontaneously aborted embryos with normal chromosomal integrity. Fertil Steril 2008;90(5):1605-1610. [ Links ]
50. Sellers TA, Kushi LH, Cerhan JR,Vierkant RA, Gapstur SM,Vachon CM, et al. Dietary folate intake, alcohol, and risk of breast cancer in a prospective study of postmenopausal women. Epidemiology 2001;12(4):420-428. [ Links ]
51. Sellers TA,Alberts SR,Vierkant RA, Grabrick DM, Cerhan JR,Vachon CM, et al. High-folate diets and breast cancer survival in a prospective cohort study. Nutr Cancer 2002;44(2):139-144. [ Links ]
52. Zhang Y, Kreger BE, Dorgan JF, Splansky GL, Cupples LA, Ellison RC. Alcohol consumption and risk of breast cancer: the Framingham Study revisited.Am J Epidemiol 1999;149(2):93-101. [ Links ]
53. Duffy CM,Assaf A, Cyr M, Burkholder G, Coccio E, Rohan T, et al. Alcohol and folate intake and breast cancer risk in the WHI Observational Study. Breast Cancer Res Treat 2009;116(3):551-562. [ Links ]
54. Feigelson HS, Jonas CR, Robertson AS, McCullough ML,Thun MJ, Calle EE.Alcohol, folate, methionine, and risk of incident breast cancer in the American Cancer Society Cancer Prevention Study II Nutrition Cohort. Cancer Epidemiol Biomarkers Prev 2003;12(2):161-164. [ Links ]
55. Tjonneland A, Christensen J, Olsen A, Stripp C, Nissen SB, Overvad K, et al. Folate intake, alcohol and risk of breast cancer among postmenopausal women in Denmark. Eur J Clin Nutr 2006;60(2):280-286. [ Links ]
56. U.S. Department of Agriculture. USDA National Nutrient Database for Standard Reference. [Accessed 2009, december 28].Available from: http://www.ars.usda.gov/ba/bhnrc/ndl. [ Links ]
57. World Congress Research Fund and American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective.Washington, DC:World Congress Research Fund and American Institute for Cancer Research, 2007. [ Links ]
58. World Health Organization. Global Status Report on Alcohol 2004. Geneva:World Health Organization, 2004. [ Links ]
59. Boffetta P, Hashine M.Alcohol and cancer. Lancet Oncol [Review] 2006;7:149-156. [ Links ]
60. Moller HHT.Alcohol drinking, social class and cancer. In: Kogevinas M, Pearce N, editors. Social inequalities and cancer. Lyon, France: International Agency for Research on Cancer 1997:251-263. [ Links ]
61. Pike MC, Kolonel LN, Henderson BE,Wilkens LR, Hankin JH, Feigelson HS, et al. Breast cancer in a multiethnic cohort in Hawaii and Los Angeles: risk factor-adjusted incidence in Japanese equals and in Hawaiians exceeds that in whites. Cancer Epidemiol Biomarkers Prev 2002;11(9):795-800. [ Links ]
 Corresponding author:
Corresponding author:
Gloria D. Coronado
Kaiser Permanente Center for Health Research
3800 N Interstate. Ave. Portland, OR, 97227, USA
E-mail: gloria.d.coronado@kpchr.org
Accepted on: September 27, 2011


{kind=link}