










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.53 no.5 Cuernavaca sep./oct. 2011
ARTÍCULO DE REVISÍON
Isabelle Romieu, MD, MPH, ScD
International Agency for Research on Cancer (IARC). France
ABSTRACT
Both diet and nutrition have been studied in relationship with breast cancer risk, as the great variation among different countries in breast cancer incidence could possibly be explained through the inflammatory and immune response, as well as antioxidant intake, among others.To date, no clear association with diet beyond overweight and weight gain has been found, except for alcohol consumption. Nonetheless, the small number of studies done in middle to low income countries where variability of food intake is wider,is beginning to show interesting results.
Key words: breast neoplasms;diet;risk;epidemiology;energy intake
RESUMEN
Tanto la dieta como la nutrición han sido estudiadas en relación con el riesgo de cáncer de mama, dada la gran variación de incidencia de cáncer entre países, y la posibilidad de explicarla a través de la respuesta inflamatoria o inmune, así como ingesta de antioxidantes,entre otros.Hasta la fecha, ninguna asociación clara con la dieta ha sido encontrada, excepto para el consumo de alcohol, más allá del sobrepeso y del incremento de peso. Sin embargo, los estudios que se están realizando en países de mediano a bajo nivel de ingresos, con mayor variabilidad de ingesta de alimentos, comienzan a mostrar resultados interesantes.
Palabras clave: neoplasia de mama;dieta;riesgo;epidemiología; ingestión de energía
Breast cancer is the most common cancer in women of high-income countries: however, over the past20 to 30 years, data support a trend of increasing incidence and mortality from breast cancer in lower income countries.1 Multiple risk factors have beenidentified for breast cancer and can be divided into those that cannot be modified and those that are potentially modifiable. Diet is part of the modifiable risk factors together with adiposity, physical activity, smoking, alcohol consumption, and use of hormonal replacement therapy.2
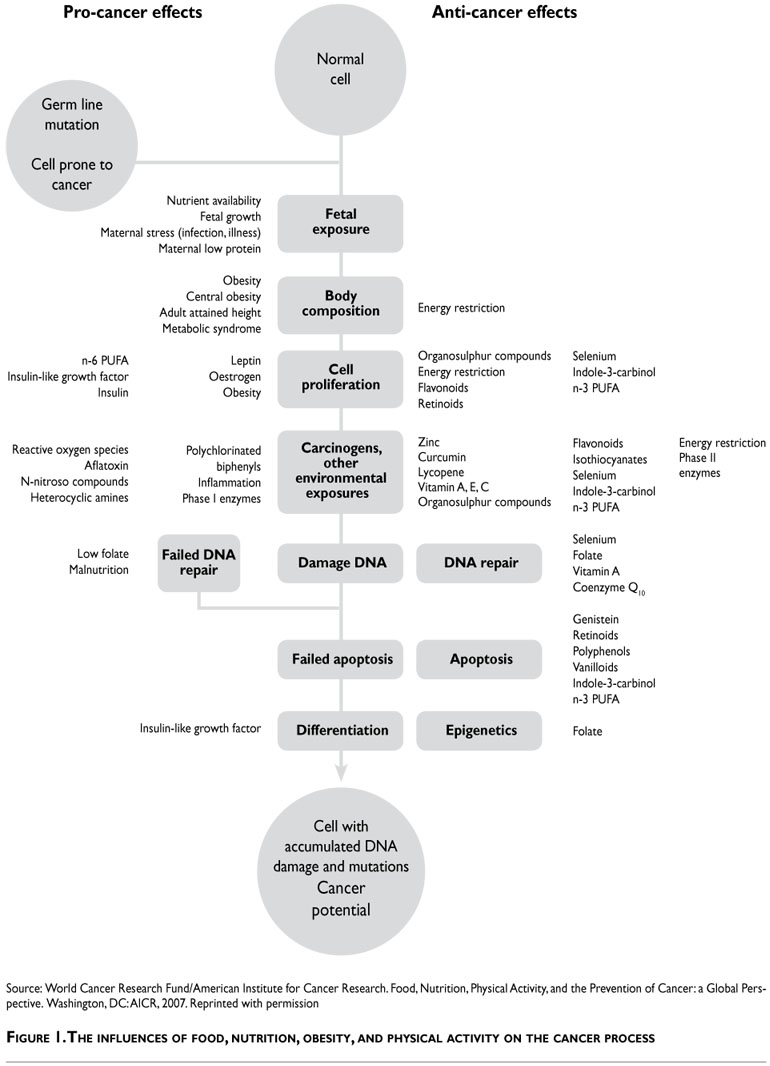
Arole for diet in cancer etiology has been suggested in part because of the large international variation in cancer rates and may be ascribed to the antioxidant properties of selected nutrients, their influence on inflammatory and immune response, on the progression of cells through the cells cycle and DNA repair, DNAmutations, DNA adducts, metabolic detoxification, the stimulation of growth factors and the potential antiestrogen influence of some nutrients3 (Figure 1).
Some foods and nutrients have also been suggested to increase the risk for breast cancer through an increase in circulating levels of endogenous estrogen, insulin like growth factor 1 or other growth factors. Energy balance, the interplay of caloric intake, physical activity and metabolic rate, is another important factor impacting breast cancer risk through mechanisms not entirely understood.4
Study design
Both case-control and cohort studies have been used to evaluate the association between diet and breast cancer, while few randomized trials have been conducted because it is difficult to randomize large numbers of women to specific diet and maintain long term compliance. The long latency of breast cancer makes evaluation of diet during early life, a period when environmental exposure may play a strong role, a further methodological challenge.2
Dietary assessment
The use of a questionnaire to assess diet in the past is limited by participant's memory, in particular with a self administered questionnaire. In addition dietary intake reported by subjects most likely represents current diet or diet a few years in the past. The measurement error resulting from inaccurate reporting would tend to underestimate the association between dietary factors and breast cancer. Dietary questionnaires usually provide adequate ranking of individuals for dietary intake but cannot provide accurate quantitative intake. In case-control studies, recall of diet might be differential between cases and controls and lead to bias in the estimation.
Biomarkers of intake
The use of biomarkers that reflect dietary intake has potential advantages compared with the assessment of dietary intake through self reports, as reporting errors and limitations of food composition tables are avoided. However, levels of biomarkers can be affected by several factors other than diet, such as smoking or metabolic factors. In addition, levels of biomarkers reflecting intake in an accurate manner are only for a limited number of foods and nutrients. Finally, depending on the biomarkers it can reflect longer or shorter exposure (e.g. the fatty composition of adipose tissue reflects long-term intake , whereas the fatty acid profile of serum or plasma phospholipids reflect medium term intake).4
Links between diet and risk of breast cancer have been extensively investigated but many topics remain controversial. This apparent lack of association may be real, or may be due to measurement error exceeding variation in the diet studied, and to a low heterogeneity of intake in the populations under study.
Diet and breast cancer
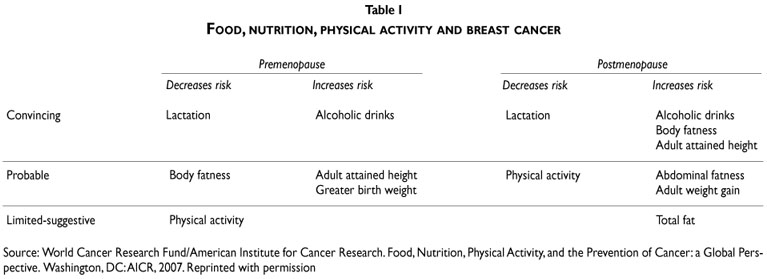
The large body of literature on nutrition and breast cancer has been recently reviewed and summarized.2,4-6 An international panel of the World Cancer Research Fund and the American Institute for Cancer Research concluded that there is convincing evidence that alcohol intake raises the risk of breast cancer at all ages, while body fatness increase the risk of breast cancer after menopause.7 Taller height is related to elevated risk of breast cancer, possibly because it is a marker for genetic, environmental, hormonal and nutritional factors affecting growth, and body fatness is probably related to a decreased risk of premenopausal breast cancer. The panel found limited evidence and drew no firm conclusions on the role of individual's foods and nutrients on overall breast cancer risk (Table I).
Carbohydrates, glycemic index and glycemic load
Carbohydrates and carbohydrate quality could influence breast cancer risk by affecting insulin resistance and plasma levels of insulin and glucose.4 Chronically Limited-suggestive Physical activity Total fat Source: World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. Washington, DC:AICR, 2007. Reprinted with permission raised insulin levels may increase carcinogenesis in breast tissue by directly stimulating insulin receptors or through a reduction in plasma and tissue levels of IGF binding proteins 1 and 2, which may in turn increase the availability of IGF-1.8 Experimental studies have found strong proliferative and antiapoptotic effects of IGF-1 in breast tissue.9 Elevated carbohydrate intake, and in particular rapidly-absorbed carbohydrates, may affect BC risk by maintaining a constant insulin demand through rapid increases in blood glucose.
Nevertheless, these insulin-mediated mechanisms have not been fully supported by observational studies where circulating IGF-1 levels have not been associated to postmenopausal cancer and seem to be only marginally relevant for premenopausal cancer.10 To date the 12 prospective cohort studies have not shownconsistent associations between total carbohydrate, glycemic index, glycemic load and breast cancer.2
Nevertheless, there is a suggestion that carbohydrates may play a role when lifestyle factors, menopausal status and hormone receptor status are considered. In a recent large prospective study in France, overall glycemic index was associated with BC risk amongoverweight women (RR= 1.35 (95% CI: 1.00, 1.82)]when comparing extreme quartiles of intake11 suggesting that carbohydrates intake may be of relevance forBC in the presence of underlying insulin resistance.
Data from Mexico support the association between carbohydrate intake and glycemic load with breast cancer among pre- and postmenopausal women.12 Compared with women in the lowest quartile of total carbohydrate intake, the odds ratio of BC for women in the highest quartile was 2.22 (95% CI: 1.63-3.04).Carbohydrates account for 64% of caloric intake in the Mexican population.13 This large variability in intake is not observed in western populations and may account for the apparent discrepancy between observations made in Mexico and elsewhere. It is also likely that high intake of refined carbohydrates could have stronger associations with risk of BC in populations genetically susceptible to insulin resistance, such as inMexico, particularly when combined with low levels of physical activity and obesity.
Dietary fat
Potential mechanisms of fat intake of breast cancer include an influence on sex hormone levels or higher energy density affecting other risk factors such as weigh gain or age at menarche.2 While animal feeding studies have shown for several decades that high-fat diets induce mammary carcinogenesis,14 experimental and epidemiologic data have been unable to clearly define the biological pathways that would lead to carcinogenesis.15,16 Evidence from large cohort studies has been unsupportive. Two meta analyses and clinical trials have not supported a strong association with total fat. A pooled analysis of eight prospective cohorts and a recent analysis of the Nurses' Health study over a 20 years follow up found a null association.17,18 In the large Women's Health Initiative (WHI) randomized trial low-fat diet was related to a 9% lower risk of BC in the intervention group.19 However, results of this trial are difficult to interpret because actual fat intake between the intervention and the control group was small. The difference in BC incidence between groups could be explained by the observed reduction of weight and an increase in fruit and vegetable intake in the intervention group.
Considering specific type of fats, results are also inconclusive. Long chain polyunsaturated fatty acids (LCPUFA) might increase breast cancer risk and than high levels of antioxidants might oppose the apoptic effect of n-3 LCPUFA.20 Data using the lipidome approach (integrated view over the complex lipid interaction or lipid profile based on adipose tissue samples) suggest that elevated monounsaturated and low n-6/n-3 fatty acids ratio is associated with decreased breast cancer risks.21
Recently interest has been raised on the impact of trans-fatty acids on cancer. Trans-fatty acids are unsaturated fatty acids with at least a double bond in the trans-configuration. Humans do not synthesize trans-fatty acids; the main source is therefore dietaryintake of industrialized products containing partially hydrogenated oils such as margarine, rolls, etc.22 Little data is available on the role of transfatty acids on BC. However in a large cohort of French women (E3N cohort study), an increased risk of BC was observed with increasing levels of the trans-monounsaturated fatty acids (palmitoleic and elaidic acid) (OR 1.75, 95% CI: 1.08-2.83) suggesting the role of industrially processed food on the risk of BC.22
Red meat and processed food
Red meat consumption could affect the risk of breast cancer because of the highly bioavailable iron content, growth-promoting hormones used in animal production, carcinogenetic heterocyclic amines formed during cooking and its specific fatty acids contents. Pooled analyses of case-control and cohort studies have yield conflicting results.2 However, recent reports suggest a positive association between the consumption of red meat and processed meat and the risk of breast cancer according to specific receptor status [estrogen receptors (ER) and progesterone receptors (PR)]23 and potential susceptibility to carcinogenic amines due to polymor phisms in N-acetyl transferase.24
Fruits and vegetables
The antioxidant and fiber content of fruits and vegetables has been hypothesized to protect from BC. Apooled analysis from eight prospective studies found no significant association for neither vegetable nor fruits with breast cancer25 and results from a large prospective European study confirm those results.26 No reduction on recurrence or mortality was observed in the Women's Health Eating and Living (WHEL) trial randomized to a very high intake of fruits and vegetables and fiber and low fat.27 When considering antioxidant intake, there is no consistent association between any antioxidant and BC incidence;4 However, three studies have suggested a protective effect of vitamin E. In a Danish study, vitamin E intake has been related to a lower risk of BC among postmenopausal women28 and two reports suggest a protective effect of high serum vitamin E on breast cancer risk.29,30
Alcohol
Alcohol is the dietary factor for which the associationwith BC is most consistent and biological mechanisms are more clearly defined. Prospective studies involving several thousand BC cases report that increasing alcohol consumption is associated with a moderate linear increase in the risk of BC ranging from 3 to 9% for oneadditional drink per day (10 g).31,32 The association is present in both premenopausal and postmenopausal women, does not vary by type of alcoholic beverage,31,32 does not seem to depend on drinking frequency,31,33 and is mostly restricted to estrogen positive breast tumors.34 The relevant timing of exposure seems to be recent alcohol intake: alcohol intake during adolescence35,36 and after adjustment for current alcohol consumption, intake in the 20s, 30s and 40s age periods is not associated to subsequent BC.31 The best supported mechanism underlying this association is related circulatingestrogen levels. Experimental studies have shown that addition of alcohol to BC cells results in estrogenmediated signaling and proliferation.37,38 Controlled feeding trials have shown that moderate alcohol intake increases circulating estrogen levels in both pre-and postmenopausal women.39,40 Alcohol intake in Mexican women is still relatively low, less than 5% of middle aged women report weekly consumption of alcohol.41
However, 10% of adolescent girls aged 16 to 19 report alcohol consumption at least once a week. Elevated alcohol intake in younger women may result in alcohol intake patterns later in life that may increase BC risk.
Folate
Folate participates in DNA metabolism in the synthesis of purines and thymidilate and is a methyl donor for DNA methylation reactions. Low levels of folate may result in a disruption of DNA repair and replication processes and in abnormal methylation and gene expression.42 Most prospective studies do not provide evidence of an association between folate intake and BC risk43,44 and results from the Nurses' Health Study are only suggestive of an inverse association with circulating folate levels.45 High intake of folate as well as circulating levels may be associated with lower risk of BC among moderate to high alcohol-drinkers.45,46 Ethanol may produce a physiologic deficiency that affects one carbon metabolism by reducing folate absorption in the gastrointestinal tract or by inhibiting enzymatic activity.42 It is possible that the benefit of folate may only be observable in individuals with low folate status. This is supported by observations in populations where folate fortification is not present and vitamin supplementation is infrequent.47-51 In a population-based case-control study in Mexico, where folate intake is low, the odds ratio for the highest quartile of folate intake compared to the lowest was 0.62 (95% CI: 0.45-0.90).51 Folate may play a dual role in human cancer etiology by conferring protection in early carcinogenesis and promoting cancer growth later in the carcinogenic process. In a screening trial in the United States after widespread folate fortification a significant increase in BC risk with increasing folate intake was observed [RR=1.32 (95%CI: 1.04-1.68) comparing the highest to the lowest level of intake].52 In this population total folate intake was several times higher than what was observed in other studies and the increased risk was mostly related to folic acid supplementation. Furthermore, there is a suggestion that vitamin B12, a co-enzyme in folate metabolism, may be associated to lower risk of BC and that low vitamin B12 intake may reduce the apparent protection in the risk for BC conferred by folate.51-54
Vitamin D
Vitamin D has recently emerged as a potentially important determinant of BC; however, information is still scant. Vitamin D is a fat-soluble vitamin and a hormone present in food in two forms: cholecalciferol (D3) from animal sources and ergocalciferol (D2) from plant sources. The main source of vitamin D3 in humans is epidermally-generated through the exposure to UV light.55 Vitamins D2 and D3 are metabolized to 25-hydroxyvitamin D [25-(OH) D] in the liver and then transformed in the kidneys into the biologicallyactive and closely regulated 1,25-dihydroxyvitamin D [1,25-(OH2) D].56 Experimental studies have shown that 1,25-(OH2) D can inhibit cellular proliferation, induce differentiation and apoptosis, inhibit angiogenesis in normal and cancer cells and modulate gene expression.57
Results from epidemiologic studies suggest an inverse association between vitamin D intake and BC, particularly among premenopausal women. The risk ratiofor premenopausal BC comparing extreme categories of intake was 0.72 (95%CI: 0.55-0.94) in the Nurses' HealthStudy58 and 0.65 (95%CI: 0.42-1.00) in the Women'sHealth Study.59 A pooled analysis found a strong linear inverse association between serum 25(OH)D and BCrisk;60 while results for 1,25-(OH2) D were less clear.
Vitamin D status appears to be affected by factors associated to intake, UV light exposure and factors that may affect its metabolism. Among Mexican women, intake of vitamin D is well below the Recommended Dietary Allowance of 5µg/day13 and the finding that Mexican-Americans have a significantly lower level of circulating vitamin D as compared to US whites61 is supported by the observation that individuals with pigmented skin may have deficient vitamin D levels even when sun exposure is abundant.62
Dietary fiber and other foods and nutrients
Fiber could play a role on the risk of BC by decreasing the intestinal reabsorption of estrogen and therefore lowering its circulating levels.63 Fiber intake has also been related to an increase in serum levels of insulin growth factor binding protein-3 (IGFBP-3), the main protein carrier for IGF-1.64 However to date there is no clear data on the role of fiber on the risk of BC.65 In Mexico, case-control studies suggest a protective effect of fiber intake on BC risk.12,66 Tea has been hypothesized to be associated with a reduced risk of BC through the anticarcinogenic effect of polyphenolic flavonoids.67 A meta-analysis found an inverse association between green tea and BC, the summary odds ratio for the highest versus the lowest exposure level was 0.78 (95%CI: 0.61-0.98).67 However, results for black tea have been consistently null and a prospective analysis of total polyphenol intake did not yield significant findings.68 70
Interest in coffee as a potential determinant of BC originated from observation that women who reduced consumption of coffee experienced a regression of fibrocystic disease of the breast, a known risk factor for BC.71 However, results for coffee intake and BC on most large prospective cohorts are essentially null.72,73 In Sweden, the largest per capita consumer of coffee, women who consumed four or more cups of coffee a day had a relative risk of 0.94 (95% CI: 0.75-1.28) as compared to women who had one cup a week or less.74 Phytoestrogens have been evaluated as nutrients that may potentially reduce BC risk. Isoflavonoids, coumestrol and lignans are mainly found in soybeans, cereals and grains and these nutrients have been hypothesized to act as weak estrogen agonist or antagonists.75,76 A recent meta analysis reported a pooled relative risk comparing high and low soy intake of 0.86 (95%CI: 0.75-0.99).77 In Mexico case-control studies observed a protective effect of phytoestrogen intake on BC risk.78,79
Early-life diet and breast cancer
Exposure in early life may be particularly importantin predicting later risk of breast cancer. The mammary gland is most susceptible to environmental exposure before the accelerated cell differentiation during puberty and first pregnancy. Animal studies suggest that mammary tissue is especially sensitive to carcinogenic exposures that occur after menarche and before first pregnancy.80 Nutrition in early life can affect height and age at menarche, established risks factors for BC. Data from case-control studies suggest decreased risk for cancer with diets high in fat from dairy foods, milk, vitamin D and increased risk with high consumption of meat with visible fat.2 Data from the NHSII suggest a protective effect of vegetable consumption and vitamin E and an increased risk with the consumptionof foods with high glycemic index during adolescencewith BC.81 Data in Asian population suggest that high intake of soy and phytoestrogen in adolescence isrelated to lower risk of BC.82-84
Dietary pattern and breast cancer
Assessment of dietary patterns reported in population studies is an approach to analyzing intake of foods in the context of the whole diet and may be of particular interest to public health, providing a basis to make recommendations on eating practices to prevent disease, such as healthy food choices. A recent meta-analysis of studies on dietary pattern and breast cancer suggest a decreased risk of breast cancer in the highest compared to the lowest categories of prudent/healthy pattern and an increased risk in the highest category of a drinker pattern.85 Data from Singapore suggest that a diet rich in vegetable (cruciferous) fruit and tofu items had a protective effect on breast cancer among postmenopausal women.86 Data from a large cohort study conducted in French women support the protective effect of a healthy/Mediterranean pattern (essentially vegetables, fruits, seafood, olive oil and sunflower oil) on breast cancer among postmenopausal women particularly on ER + and PR+ tumors.87
Conclusion
Among the prospective epidemiological studies conducted on diet and breast cancer to date there is no clear association with diet except for alcohol consumption in addition to overweight and weight gain. Most of the studies have been conducted in Western countries with some limitations in variability of diet exposure. Few studies are available from middle to low income countries where variability in food intake is wider and food supplementation less prevalent. Data from Mexico suggest that high intake of carbohydrate and high glycemic load is related to an increase of breast cancer and that high intake of folate and phytoestrogens are related to lower risk. Although these results need to be confirmed in other populations, they suggest that baseline nutritional status and genetic susceptibility might interact with food intake in relation with BC.
Several factors need to be considered in the interpretation of the current literature:
1. Variation in diet in the study population conditions the power of a study to detect a true association. While some studies have combined several populations with different diet, the variability might not be sufficient to evaluate small effect of diet. Taking advantage of international variation and population in epidemiological transition as observed in low to middle income countries would increase our ability to evaluate the role of diet and changing diet on cancer risk.
2. Dietary assessment was mostly based on questionnaires and self reports. Although in many studies these questionnaires had been validated, there is potential for measurement error leading to an underestimation of any causal association between diet and breast cancer. Development of methods for a better evaluation of dietary intake is needed using biomarkers and metabolic profiles.
3. Timing of dietary assessment and follow up time. Experimental data suggest that adolescence might be a period of more susceptibility to environmental factors. Most of the cohort studies have focused on adult intake assessed at baseline among women 40 and older, exploring mostly the relation of diet in postmenopausal women. There is not sufficient information on the relation of diet during early years and the association with premenopausal breast cancer. In addition, in some cases follow up may not be sufficient to fully capture the effect of diet.
4. Stratification of breast cancer by specific characteristic should be considered, in particular receptor status (ER, PR, HER). It is likely that diet may act differently on different types of cancer and this need to be further explored. However, given the lost of power in stratified analyses, only studies with large numbers of cases or pooling of studies will allow such analyses.
5. Food toxins might be ingested with regular diet and could counteract some beneficial effect of foods. Studying intake of organic foods or, vegetarian regimes need to be further explored.
6. Foods and nutrients have interactive effects and this is difficult to capture in epidemiological studies. Having metabolic profiles of individuals through a metabolomic approach could provide a more integrated evaluation about the impact of diet on breast cancer.
7. Gene-diet interaction is particularly important in the field of diet and breast cancer because most existing evidence has not revealed strong association with risk. Large genome wide association studies are on their way and will provide further insight on potential gene-diet interaction.
8. Diet may also interact with genetic predisposition via epigenetic mechanisms. Epigenetic refers to the study of processes that alter gene activity without changing the DNA sequences.88 Dietary intake of methyl donors (such as folate, vitamin B12, choline and betaine) during pregnancy influence methylation in mouse models.89 In addition, emerging evidences suggest that exposures during adulthood can influence methylation90 and epigenetic malfunction appear to play an important role in cancer development.91 Further investigations are needed in order to unravel the role of diet on the DNA hypermethylome in breast cancer cells.
Declaration of conflict of interests: The author declares not to have conflict of interests.
References
1. Potter I. Global trends in breast cancer incidence and mortality. Salud Publica Mex 2009;51:S141-S146. [ Links ]
2. Mahoney MC, Bevers T, Linos E,Willett WC. Opportunities and strategies for breast cancer prevention through risk reduction. CA Cancer J Clin 2008;58:347-371. [ Links ]
3.World Cancer research Fund/American Institute for Cancer Research. The cancer process. In:World Cancer research Fund/American Institute for Cancer Research, editor. Food, nutrition, physical activity, and the prevention of cancer: a global perspective.Washington, DC:AICR, 2007:30-46. [ Links ]
4. Michels KB, Mohllajee AP, Roset-Bahmanyar E, Beehler GP, Moysich KB. Diet and breast cancer: a review of the prospective observational studies. Cancer 2007;109:2712-2749. [ Links ]
5. Linos E,Willett WC. Diet and breast cancer risk reduction. J Natl Compr Canc Netw 2007;5:711-718. [ Links ]
6.World Cancer research Fund/American Institute for Cancer Research. Food, nutrition, physical activity, and the prevention of cancer: a global perspective.Washington, DC:AIRC, 2007. [ Links ]
7.World Cancer research Fund/American Institute for Cancer Research. Breast. In:World Cancer research Fund/American Institute for Cancer Research, editor. Food, nutrition, physical activity, and the prevention of cancer: a global perspective.Washington, DC:AICR; 2007: 289-298. [ Links ]
8. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 2004;4:579-591. [ Links ]
9.Yanochko GM, Eckhart W.Type I insulin-like growth factor receptor over-expression induces proliferation and anti-apoptotic signaling in a three-dimensional culture model of breast epithelial cells. Breast Cancer Res 2006;8:R18. [ Links ]
10. Fletcher O, Gibson L, Johnson N,Altmann DR, Holly JM,Ashworth A, et al. Polymorphisms and circulating levels in the insulin-like growth factor system and risk of breast cancer: a systematic review. Cancer Epidemiol Biomarkers Prev 2005;14:2-19. [ Links ]
11. Lajous M, Boutron-Ruault MC, Fabre A, Clavel-Chapelon F, Romieu I. Carbohydrate intake, glycemic index, glycemic load, and risk of postmenopausal breast cancer in a prospective study of French women.Am J Clin Nutr 2008;87:1384-1391. [ Links ]
12. Romieu I, Lazcano-Ponce E, Sanchez-Zamorano LM,Willett W, Hernandez-Avila M. Carbohydrates and the risk of breast cancer among Mexican women. Cancer Epidemiol Biomarkers Prev 2004;13:1283-1289. [ Links ]
13. Rivera-Dommarco J, Shamah-Levy T,Villalpando-Hernández S, González-Cossio T, Hernández-Prado B, Sepúlveda J. Encuesta Nacional de Nutrición 1999. Estado nutricio de niños y mujeres en México. Cuernavaca, Morelos, México: Instituto Nacional de Salud Pública, 2001. [ Links ]
14. Fay MP, Freedman LS. Meta-analyses of dietary fats and mammary neoplasms in rodent experiments. Breast Cancer Res Treat 1997;46:215-223. [ Links ]
15.Wu AH, Pike MC, Stram DO. Meta-analysis: dietary fat intake, serum estrogen levels, and the risk of breast cancer. J Natl Cancer Inst 1999;91:529-534. [ Links ]
16.Woutersen RA,Appel MJ, van Garderen-Hoetmer A,Wijnands MV. Dietary fat and carcinogenesis. Mutat Res 1999;443:111-127. [ Links ]
17. Smith-Warner SA, Spiegelman D,Adami HO, Beeson WL, van den Brandt PA, Folsom AR, et al.Types of dietary fat and breast cancer: a pooled analysis of cohort studies. Int J Cancer 2001;92:767-774. [ Links ]
18. Kim EH,Willett WC, Colditz GA, Hankinson SE, Stampfer MJ, Hunter DJ, et al. Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up.Am J Epidemiol 2006;164:990-997. [ Links ]
19. Prentice RL,Thomson CA, Caan B, Hubbell FA,Anderson GL, Beresford SA, et al. Low-fat dietary pattern and cancer incidence in the Women's Health Initiative Dietary Modification Randomized Controlled Trial. J Natl Cancer Inst 2007;99(20):1534-1543. [ Links ]
20. Gerber M. Background review paper on total fat, fatty acid intake and cancers.Ann Nutr Metab 2009;55:140-161. [ Links ]
21. Bougnoux P, Hajjaji N, Couet C.The lipidome as a composite biomarker of the modifiable part of the risk of breast cancer. Prostaglandins Leukot Essent Fatty Acids 2008;79:93-96. [ Links ]
22. Chajès V,Thiébaut AC, Rotival M, Gauthier E, Maillard V, Boutron-Ruault MC, et al.Association between serum trans-monounsaturated fatty acids and breast cancer risk in the E3N-EPIC Study.Am J Epidemiol 2008;167:1312-1320. [ Links ]
23. Cho E, Chen WY, Hunter DJ, Stampfer MJ, Colditz GA, Hankinson SE, et al. Red meat intake and risk of breast cancer among premenopausal women.Arch Intern Med 2006;166:2253-2259. [ Links ]
24. Egeberg R, Olsen A,Autrup H, Christensen J, Stripp C,Tetens I, et al. Meat consumption, N-acetyl transferase 1 and 2 polymorphism and risk of breast cancer in Danish postmenopausal women. Eur J Cancer Prev 2008;17:39-47. [ Links ]
25. Smith-Warner SA, Spiegelman D,Yaun SS,Adami HO, Beeson WL, van den Brandt PA, et al. Intake of fruits and vegetables and risk of breast cancer: a pooled analysis of cohort studies. JAMA 2001;285:769-776. [ Links ]
26. van Gils CH, Peeters PH, Bueno-de-Mesquita HB, Boshuizen HC, Lahmann PH, Clavel-Chapelon F, et al. Consumption of vegetables and fruits and risk of breast cancer. JAMA 2005;293:183-193. [ Links ]
27. Pierce JP, Natarajan L, Caan BJ, Parker BA, Greenberg ER, Flatt SW, et al. Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: the Women's Healthy Eating and Living (WHEL) randomized trial. JAMA 2007;298:289-298. [ Links ]
28. Nissen SB,Tjønneland A, Stripp C, Olsen A, Christensen J, Overvad K, et al. Intake of vitamins A, C, and E from diet and supplements and breast cancer in postmenopausal women. Cancer Causes Control 2003;14:695-704. [ Links ]
29. Hultén K,Van Kappel AL,Winkvist A, Kaaks R, Hallmans G, Lenner P, et al. Carotenoids, alpha-tocopherols, and retinol in plasma and breast cancer risk in northern Sweden. Cancer Causes Control 2001;12:529-537. [ Links ]
30.Wald NJ, Boreham J, Hayward JL, Bulbrook RD. Plasma retinol, betacarotene and vitamin E levels in relation to the future risk of breast cancer. Br J Cancer 1984;49:321-324. [ Links ]
31.Tjonneland A, Christensen J, Olsen A, Stripp C,Thomsen BL, Overvad K, et al.Alcohol intake and breast cancer risk: the European Prospective Investigation into Cancer and Nutrition (EPIC). Cancer Causes Control 2007;18:361-373. [ Links ]
32. Smith-Warner SA, Spiegelman D,Yaun SS, van den Brandt PA, Folsom AR, Goldbohm RA, et al.Alcohol and breast cancer in women: a pooled analysis of cohort studies. JAMA 1998;279:535-540. [ Links ]
33. Horn-Ross PL, Canchola AJ,West DW, Stewart SL, Bernstein L, Deapen D, et al. Patterns of alcohol consumption and breast cancer risk in the California Teachers Study cohort. Cancer Epidemiol Biomarkers Prev 2004;13:405-411. [ Links ]
34. Zhang SM, Lee IM, Manson JE, Cook NR,Willett WC, Buring JE.Alcohol consumption and breast cancer risk in the Women's Health Study.Am J Epidemiol 2007;165:667-676. [ Links ]
35. Marcus PM, Newman B, Millikan RC, Moorman PG, Baird DD, Qaqish B.The associations of adolescent cigarette smoking, alcoholic beverage consumption, environmental tobacco smoke, and ionizing radiation with subsequent breast cancer risk (United States). Cancer Causes Control 2000;11:271-278. [ Links ]
36. Holmberg L, Baron JA, Byers T,Wolk A, Ohlander EM, Zack M, et al. Alcohol intake and breast cancer risk: effect of exposure from 15 years of age. Cancer Epidemiol Biomarkers Prev 1995;4:843-847. [ Links ]
37. Singletary KW, Frey RS,Yan W. Effect of ethanol on proliferation and estrogen receptor-alpha expression in human breast cancer cells. Cancer Lett 2001;165:131-137. [ Links ]
38. Fan S, Meng Q, Gao B, Grossman J,Yadegari M, Goldberg ID, et al. Alcohol stimulates estrogen receptor signaling in human breast cancer cell lines. Cancer Res 2000;60:5636-5639. [ Links ]
39. Reichman ME, Judd JT, Longcope C, Schatzkin A, Clevidence BA, Nair PP, et al. Effects of alcohol consumption on plasma and urinary hormone concentrations in premenopausal women. J Natl Cancer Inst 1993;85:722-727. [ Links ]
40. Dorgan JF, Baer DJ,Albert PS, Judd JT, Brown ED, Corle DK, et al. Serum hormones and the alcohol-breast cancer association in postmenopausal women. J Natl Cancer Inst 2001;93:710-715. [ Links ]
41. Olaiz G, Barquera S, Shamah T, Cravioto P, López P, Hernández M, et al. Encuesta Nacional de Salud 2000.Tomo I Vivienda, población y utilización de servicios de salud. Cuernavaca, Morelos, México: Instituto Nacional de Salud Pública, 2003. [ Links ]
42. Mason JB, Choi SW. Folate and carcinogenesis: developing a unifying hypothesis.Adv Enzyme Regul 2000;40:127-141. [ Links ]
43. Lewis SJ, Harbord RM, Harris R, Smith GD. Meta-analyses of observational and genetic association studies of folate intakes or levels and breast cancer risk. J Natl Cancer Inst 2006;98:1607-1622. [ Links ]
44. Larsson SC, Giovannucci E,Wolk A. Folate and risk of breast cancer: a meta-analysis. J Natl Cancer Inst 2007;99:64-76. [ Links ]
45. Zhang SM,Willett WC, Selhub J, Hunter DJ, Giovannucci EL, Holmes MD, et al. Plasma folate, vitamin B6, vitamin B12, homocysteine and risk of breast cancer. J Natl Cancer Inst 2003;95:373-380. [ Links ]
46. Zhang S, Hunter DJ, Hankinson SE, Giovannucci EL, Rosner BA, Colditz GA, et al.A prospective study of folate intake and the risk of breast cancer. JAMA 1999;281:1632-1637. [ Links ]
47. Shrubsole MJ, Gao YT, Cai Q. MTHFR polymorphisms, dietary folate intake, and breast cancer risk: results from Shanghai Breast Cancer Study. Cancer Epidemiol Biomark Prev 2004;13:190-196. [ Links ]
48. Ronco A, De Stefani E, Boffetta P, Deneo-Pellegrini H, Mendilaharsu M, Leborgne F.Vegetables, fruits, and related nutrients and risk of breast cancer: a case-control study in Uruguay. Nutr Cancer 1999;35:111-119. [ Links ]
49. Negri E, La Vecchia C, Franceschi S. Re: dietary folate consumption and breast cancer risk. J Natl Cancer Inst 2000;92:1270-1271. [ Links ]
50. Levi F, Pasche C, Lucchini F, La Vecchia C. Dietary intake of selected micronutrients and breast-cancer risk. Int J Cancer 2001;91:260-263. [ Links ]
51. Lajous M, Lazcano E, Hernandez M,Willett W, Romieu I. Folate, vitamin B6 and vitamin B12 intake and the risk of breast cancer among Mexican women. Cancer Epidemiol Biomarkers Prev 2006;15:443-448. [ Links ]
52. Stolzenberg-Solomon RZ, Chang SC, Leitzmann MF, Johnson KA, Johnson C, Buys SS, et al. Folate intake, alcohol use, and postmenopausal breast cancer risk in the prostate, lung, colorectal, and ovarian cancer screening trial.Am J Clin Nutr 2006;83:895-904. [ Links ]
53. Shrubsole MJ, Jin F, Dai Q, Shu XO, Potter JD, Hebert JR, et al. Dietary folate intake and breast cancer risk: results from the Shanghai Breast Cancer Study. Cancer Res 2001;61:7136-141. [ Links ]
54. Lajous M, Romieu I, Sabia S, Boutron-Ruault MC, Clavel-Chapelon F. Folate, vitamin B12 and postmenopausal breast cancer in a prospective study of French women. Cancer Causes Control 2006;17:1209-1213. [ Links ]
55.Welsh J.Vitamin D and prevention of breast cancer.Acta Pharmacol Sin 2007;28:1373-1382. [ Links ]
56. Holick MF.Vitamin D deficiency. N Engl J Med 2007;357:266-281. [ Links ]
57. Cui Y, Rohan TE.Vitamin D, calcium, and breast cancer risk: a review. Cancer Epidemiol Biomarkers Prev 2006;15:1427-1437. [ Links ]
58. Shin MH, Holmes MD, Hankinson SE,Wu K, Colditz GA,Willett WC. Intake of dairy products, calcium, and vitamin d and risk of breast cancer. J Natl Cancer Inst 2002;94:1301-1311. [ Links ]
59. Lin J, Manson JE, Lee IM, Cook NR, Buring JE, Zhang SM. Intakes of calcium and vitamin D and breast cancer risk in women.Arch Intern Med 2007;167:1050-1059. [ Links ]
60. Garland CF, Gorham ED, Mohr SB, Grant WB, Giovannucci EL, Lipkin M, et al.Vitamin D and prevention of breast cancer: pooled analysis. J Steroid Biochem Mol Biol 2007;103:708-711. [ Links ]
61. Kant AK, Graubard BI. Ethnicity is an independent correlate of biomarkers of micronutrient intake and status in American adults. J Nutr 2007;137:2456-2463. [ Links ]
62. Goswami R, Gupta N, Goswami D, Marwaha RK,Tandon N, Kochupillai N. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi.Am J Clin Nutr 2000;72:472-475. [ Links ]
63. Cohen LA. Dietary fiber and breast cancer.Anticancer Res 1999;19:3685-3688. [ Links ]
64. Probst-Hensch NM,Wang H, Goh VH, Seow A, Lee HP,Yu MC. Determinants of circulating insulin-like growth factor I and insulin-like growth factor binding protein 3 concentrations in a cohort of Singapore men and women. Cancer Epidemiol Biomarkers Prev 2003;12:739-746. [ Links ]
65. Mattisson I,Wirfalt E, Johansson U, Gullberg B, Olsson H. Intakes of plant foods, fibre and fat and risk of breast cancer--a prospective study in the Malmo Diet and Cancer cohort. Br J Cancer 2004;90:122-127. [ Links ]
66. Bonilla-Fernández P, López-Cervantes M,Torres-Sánchez LE,Tortolero-Luna G, López-Carrillo L. Nutritional factors and breast cancer in Mexico. Nutr Cancer 2003;45:148-155. [ Links ]
67.Yang CS, Maliakal P, Meng X. Inhibition of carcinogenesis by tea.Annu Rev Pharmacol Toxicol 2002;42:25-54. [ Links ]
68. Sun CL,Yuan JM, Koh WP. Green tea, black tea and breast cancer risk: a meta-analysis of epidemiological studies. Carcinogenesis 2006;27:1310-1315. [ Links ]
69. Baker JA, Beehler GP, Sawant AC, Jayaprakash V, McCann SE, Moysich KB. Consumption of coffee, but not black tea, is associated with decreased risk of premenopausal breast cancer. J Nutr 2006;136:166-171. [ Links ]
70. Adebamowo CA, Hu FB, Cho E, Spiegelman D, Holmes MD,Willett WC. Dietary patterns and the risk of breast cancer.Ann Epidemiol 2005;15:789-795. [ Links ]
71. Marshall LM, Hunter DJ, Connolly JL, Schnitt SJ, Byrne C, London SJ, et al. Risk of breast cancer associated with atypical hyperplasia of lobular and ductal types. Cancer Epidemiol Biomarkers Prev 1997;6:297-301. [ Links ]
72. Folsom AR, McKenzie DR, Bisgard KM, Kushi LH, Sellers TA. No association between caffeine intake and postmenopausal breast cancer incidence in the Iowa Women's Health Study.Am J Epidemiol 1993;138:380-383. [ Links ]
73. Hunter D, Manson JE, Stampfer MJ, Colditz GA, Rosner B, Hennekens CH.A prospective study of caffeine, coffee, tea and breast cancer.Am J Epidemiol 1992;136:1000-1001. [ Links ]
74. Michels KB, Holmberg L, Bergkvist L,Wolk A. Coffee, tea, and caffeine consumption and breast cancer incidence in a cohort of Swedish women. Ann Epidemiol 2002;12:21-26. [ Links ]
75. Messina M, McCaskill-Stevens W, Lampe JW.Addressing the soy and breast cancer relationship: review, commentary, and workshop proceedings. J Natl Cancer Inst 2006;98:1275-1284. [ Links ]
76. Dixon RA. Phytoestrogens. Phytoestrogens Annu Rev Plant Biol 2004;55:225-261. [ Links ]
77.Trock BJ, Hilakivi-Clarke L. Meta-analysis of soy intake and breast cancer risk. J Natl Cancer Inst 2006;98:459-471. [ Links ]
78.Torres-Sánchez L, López-Carrillo L, López-Cervantes M, Rueda-Neria C,Wolff MS. Food sources of phytoestrogens and breast cancer risk in Mexican women. Nutr Cancer 2000;37:134-139. [ Links ]
79.Torres-Sanchez L, Galvan-Portillo M,Wolff MS, Lopez-Carrillo L. Dietary consumption of phytochemicals and breast cancer risk in Mexican women. Public Health Nutr 2008;23:1-7. [ Links ]
80.Ariazi JL, Haag JD, Lindstrom MJ, Gould MN. Mammary glands of sexually immature rats are more susceptible than those of mature rats to the carcinogenic, lethal, and mutagenic effects of N-nitroso-N-methylurea. Mol Carcinog. 2005;43:155-164. [ Links ]
81. Frazier AL, Li L, Cho E,Willett WC, Colditz GA.Adolescent diet and risk of breast cancer. Cancer Causes Control 2004;15:73-82. [ Links ]
82. Shu XO, Jin F, Dai Q,Wen W, Potter JD, Kushi LH, et al. Soyfood intake during adolescence and subsequent risk of breast cancer among Chinese women. Cancer Epidemiol Biomarkers Prev 2001;10:483-488. [ Links ]
83.Thanos J, Cotterchio M, Boucher BA, Kreiger N,Thompson LU. Adolescent dietary phytoestrogen intake and breast cancer risk (Canada). Cancer Causes Control 2006;17:1253-1261. [ Links ]
84.Wu AH,Wan P, Hankin J,Tseng CC,Yu MC, Pike MC.Adolescent and adult soy intake and risk of breast cancer in Asian-Americans. Carcinogenesis 2002;23:1491-1496. [ Links ]
85. Brennan SF, Cantwell MM, Cardwell CR,Velentzis LS,Woodside JV. Dietary patterns and breast cancer risk: a systematic review and metaanalysis.Am J Clin Nutr 2010 Mar 10. [Epub ahead of print] [ Links ].
86. Butler LM,Wu AH,Wang R, Koh WP,Yuan JM,Yu MC.A vegetable-fruitsoy dietary pattern protects against breast cancer among postmenopausal Singapore Chinese women.Am J Clin Nutr 2010;91:1013-1019. [ Links ]
87. Cottet V,Touvier M, Fournier A,Touillaud MS, Lafay L, Clavel-Chapelon F, et al. Postmenopausal breast cancer risk and dietary patterns in the E3N-EPIC prospective cohort study.Am J Epidemiol 2009;170:1257-1267. [ Links ]
88. Jirtle RL, Skinner MK. Environmental epigenomics and disease susceptibility. Nat Rev Genet 2007;8:253-262. [ Links ]
89.Waterland RA, Jirtle RL.Transposable elements: targets for early nutritional effects on epigenetic gene regulation. Mol Cell Biol 2003;23:5293-5300. [ Links ]
90. Fraga MF, Ballestar E, Paz MF, Ropero S, Setien F, Ballestar ML, et al. Epigenetic differences arise during the lifetime of monozygotic twins. Proc Natl Acad Sci U S A 2005;102:10604-10609. [ Links ]
91.Veeck J, Esteller M. Breast cancer epigenetics: from DNA methylation to microRNAs. J Mammary Gland Biol Neoplasia 2010;15:5-17. [ Links ]
 Corresponding author:
Corresponding author:
Isabelle Romieu
International Agency for Research on Cancer
150 cours Albert Thomas
69372 Lyon cedex 08, France
E-mail: romieui@iarc.fr
Accepted on: September 27, 2011


{kind=link}
{kind=link}