










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkSalud Pública de México
versão impressa ISSN 0036-3634
Salud pública Méx vol.53 no.5 Cuernavaca Set./Out. 2011
ARTÍCULO DE REVISIÓN
Breast cancer in the world: Incidence and mortality
María Paula Curado, MD, PhD
Cancer Information Section, International Agency for Research on Cancer. Lyon, France
ABSTRACT
The aim of this paper is to describe the burden of breast cancer in the world, as the now most common cancer in women in the globe. Here a descriptive pattern based on information available in IARC and WHO databases describing estimated age-specific incidence is presented, both for incidence and mortality. The newer treatment modalities and screening programs have been developed to alleviate the burden of this disease, but much more needs to be done in the developing countries for the impact to reach outside of the developed nations.
Keywords: breast neoplasms; epidemiology; mortality; incidence
RESUMEN
El objetivo de este documento es describir la carga del cáncer de mama en el mundo, puesto que es el cáncer más común entre las mujeres del planeta. Aquí se presenta un patrón descriptivo basado en la información disponible en las bases de datos de la IARC y la OMS, describiendo estimaciones de la incidencia por grupos específicos de edad, tanto para incidencia como mortalidad. Las nuevas modalidades de tratamiento y programas de tamizaje se han desarrollado para aligerar la carga de esta enfermedad, pero necesita hacerse mucho más en los países en vías de desarrollo para que el impacto alcance más allá de las naciones desarrolladas.
Palabras clave: neoplasias de la mama; epidemiología; mortalidad; incidencia
The aim of this paper is to describe the burden of breast cancer in the world: breast cancer is now the most common cancer in women in the world. This document is a descriptive pattern of this cancer based on information available in IARC and WHO databases describing estimated age-specific incidence - ASR(W). Breast cancer is the most frequent type of cancer in women and it was estimated that 1.38 million new breast cancer cases were diagnosed in 2008 (23% of all cancers); it ranks second overall (10.9% of all cancers). It is the most common cancer both in developed and developing regions with around 690 000 new cases estimated in each of them (population ratio 1:4).
Breast cancer incidence
Incidence rates vary from 19.3 per 100 000 women in Eastern Africa to 89.9 per 100 000 women in Western Europe, and are high (more than 80 per 100 000) in developed regions of the world (except Japan) and low (less than 40 per 100 000) in most of the developing regions. Although developed countries have the highest incidence rates, in the transition countries as in Latin America the estimated rates are supposed to increase in the future.1 The rates vary worldwide being the highest in Europe, and they are increasing in Asian and Latin- American countries mainly due to the population ageing and screening practices. 2-5
Incidence rates are produced by Population-Based Cancer Registries (PBCRs) worldwide; however they only cover from 1 to 5% of Asia, Africa and South America. Therefore data on incidence is limited in these continents due to several factors as lack of resources, priority and lack of trained staff.
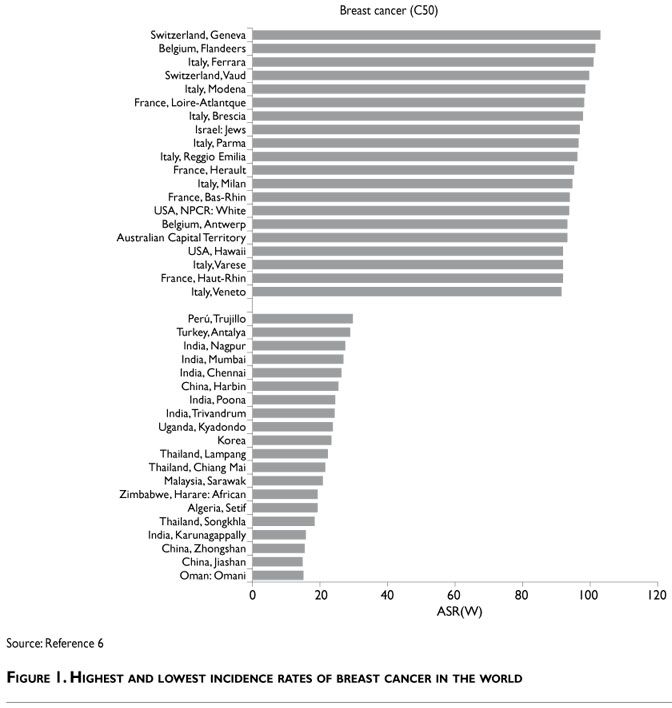
The geographical pattern described in Cancer Incidence in Five Continents, Volume IX6 (C15-IX) allows us to identify the highest and lowest rates of cancer incidence worldwide based on PBCRs data.
The total number of cases registered for the fiveyear period 1998-2002 were 13 120 964 (6 848 973 men and 6 271 991 women), the average of annual cases registered being about 1 250 000 for women and 1 369 795 for men. During this period, 1 775 353 cases of breast cancer were registered worldwide. The highest rates occurred in Europe (Belgium, France, Switzerland, Italy) and in Australia with average rates of 60-100/100 000 cases. The lowest ASR(W) was between 18-30/100 000 in India, Thailand, China and Africa (Harare and Kyadondo ) (Figure 1).
Africa
Due to the limited incidence data found in Population-Based Cancer Registries in this continent, the information is mostly based on studies and reviews from the active population cancer registries in this area.
The highest incidence rates of breast cancer in Africa are estimated for South African Republic and the lowest rates for Sudan and Ghana.1 Recent data from North Africa covering 13% of the population in the region describes low rates for breast cancer: between 30-40/100 000, except in Algiers where the rates are similar to those of Europe, namely 60.5/100 000.7
In the rural area of Eastern Cape Province of South Africa the rate of breast cancer is 7.5/100 000.8 In African women there is an overrepresentation of triple-negative breast cancer, which is the most aggressive cancer with the worst prognosis.9
There has been an increase of breast cancer in Uganda (+4.5% since 1991) but the increase was more evidentin fifty-year old women than in young women.10
Table I shows that the highest incidence rates are in Garbiah (Egypt); Sub-Saharan Africa has intermediate rates and North Africa has the lowest rates of the continent. Although incidence rates for breast cancer are low in Africa, in some of African countries it remains the most common cancer with higher rates in premenopausal women.8,10-12

Asia
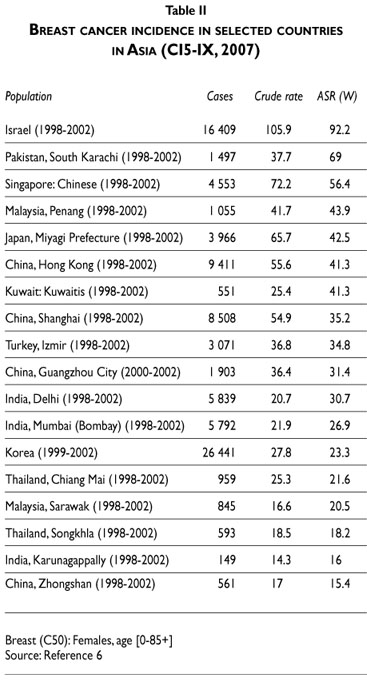
Asia is a continent with a huge population and the coverage on incidence data is a challenging task for PBCRs. From data available of Ci5 IX, the highest incidence rates of breast cancer were in Israel (96.8/100 000) where the population pattern is similar to the one of Europe. If Israel were excluded from Asia, the incidence rate would have a wide range variation from 15-50/100 000, with the highest rates in westernized areas, such as Singapore, Japan, China (Hong Kong) and the lowest rates in India, Korea and Thailand (Table II). Breast cancer in Asia is characterized by a lower incidence than in Western populations, but is still the leading type of cancer in Asian women.
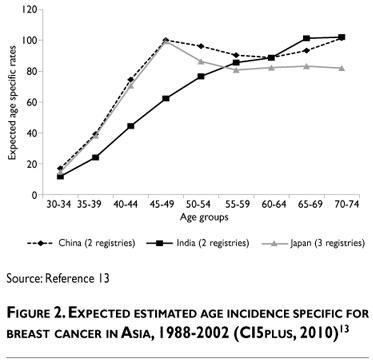
Age is the major factor on breast cancer incidence based on the incidence data for 1998-2002. The most affected women in Japan and China are between 45 and 50 years old, whereas for Indian women the rate is lower for the same age group and increases at old ages, similarly to the western women (Figure 2).13 In China, the affected population in rural areas is young in contrast urban areas. In 2005, rates of breast cancer were 33/100 000 in urban areas and 12.23/100 000 in rural areas. In urban areas, the rate was 217% higher than in rural areas, decreasing to 167% after age-adjustment.14
In spite of the countries' policies for birth control as in China where parity is a limited protection, factors as breastfeeding and parity are unlikely to be a cause of this low rate.
Asian breast cancer is characterized by early tumor onset, showing a relatively younger median age at diagnosis. It was speculated that Asian breast cancer would have a higher frequency of the basal-like subtype of breast cancer, a molecular subtype characterized by poor differentiation, resulting in a relatively poor progression; however, recent findings do not support this speculation.15 The striking difference is that the peak age for breast cancer is between 40 and 50 years in the Asian countries, whereas the peak age in the Western countries is between 60 and 70 years. Also, the incidence of breast cancer in Asia is rising and is associated with increased mortality.16
The differences among the Asian countries need further studies regarding diagnosis, screening activities, lifestyle, genetic susceptibility, in order to clarify the reasons for these dissimilarities.
North America
The highest estimated incidence rates for breast cancer in North and South America are in Canada, USA, Argentina, Uruguay and Barbados: the ASR(W) is 9040/100.000. The lowest estimated rates are in Central America and Mexico: the ASR(W) is 15-25/100 000.17
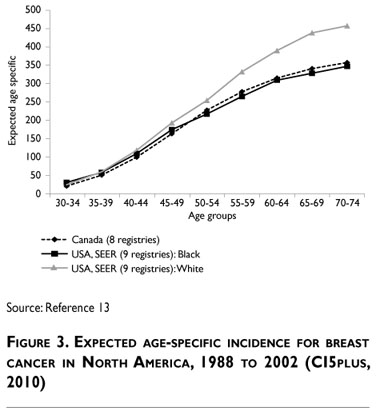
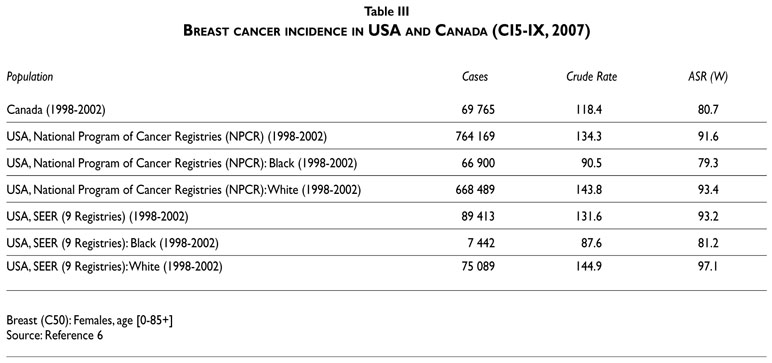
Table III shows the incidence in USAand Canada. In USA, for the period 2003-2207 from SEER, the incidence rates for breast cancer to all races were about 122/100 000 women. The highest rate was for white women, 22% of cases were diagnosed between 45 and 54 years old and 24% between 55 and 64 years old. Trend in incidence is decreasing significantly during the last five years.18 Cancer incidence in five continents volume IX showed similar rates for white women according to SEER and NPCR cancer registries, the second most affected are black women, with a rate of about 10% lower. Rates for breast cancer are decreasing in USA and one of the attributable factors to this trend is the declining use of hormonal therapy replacement in menopausal women. In Canada the rates are slightly lower than in USA.
The impact of incidence is steadily increasing from women in USA, having similar impact on age incidence as in the white women, although the incident rate is slightly lower (Figure 3).
South America
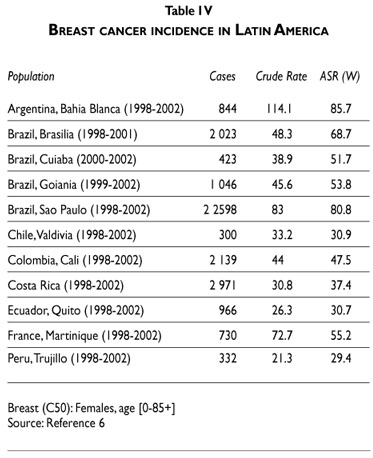
PBCRs of Latin America included in Cancer incidence in five continents volume IX represent 22.7 million people, namely 4.3% of the total population, which gives us an overview of the situation in this continent. For the period of 1998-2002, the high rates were for the south part of the continent (Argentina) and low rates for the north part (Colombia, Ecuador and Peru).
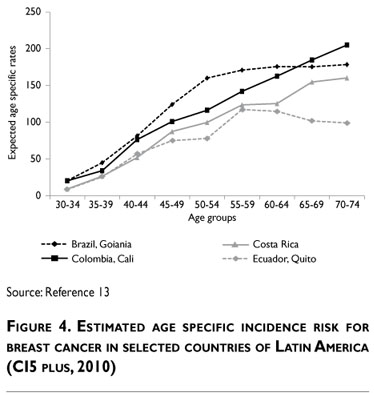
There are strong differences in the economic development between the Latin American countries, and most of them are in transition. It displays a heterogeneous pattern of breast cancer incidence. In Brazil, a continental country, the rates in the south part of the country are higher than in the central part (more rural areas). This can be a consequence of the transition pattern of this cancer incidence within the country (Table IV). Whether these countries are going to adopt policies to reduce breast cancer incidence based on knowledge acquired about some risk factors as hormonal replacement in menopausal women, it is crucial that health decision makers can use scientific evidence to promote the reduction of breast cancer incidence rates in the coming years in South America, although this is not the only attributed risk factor to increasing breast cancer incidence.
The estimated age-specific risk is high in Brazil (Goiania) for the age groups 45-59; this high burden can be attributed to opportunistic screening effects in this age group, as Brazilian policies recommended to the women over 50 to do mammography. Estimated incidence risk is lower for the same age groups 45-59 in Ecuador (Quito), Colombia and Costa Rica. For age group of over 55, pattern is similar among the countries. In the Latin American countries (except Brazil) there are no organized screening programs. The incident cases are diagnosed through a regular health care system approach (Figure 4).
Europe
Incidence rate of breast cancer in Europe is based on coverage of 238.8 million people, namely 33% of the total population. It was estimated that breast cancer comprises 7.5% of the incident cases in 2008 in 40 European countries; the number of cases estimated was 420 800 cases and 129 300 deaths.17 As Table V shows, the highest incidence rates for the period 1998-2002 were in Belgium, Switzerland and France (100/100 000 women). However the rates range from the highest in the world to the lowest as in Slovenia, Poland, Latvia and Belarus, being the lowest in Europe for this period.
₢
The highest estimated incidence rates were in Belgium (109.4/100 000) followed by Metropolitan France (99.7/100 000), and the lowest rate was in Russian Federation (43.2/100 000). In France breast cancer is the most common cancer in women.
A projection for breast cancer suggests a continuous growth in the number of incident cases that would increase from 49.814 to 64.621 between 2005 and 2018. Changes in incidence following the withdrawal of HTM use should be moderate and transient. However, trends in incidence for breast cancer in Europe are declining between 50-64 years old.19
The most important epidemiological parameter explaining the future incidence of breast cancer remains the "cohort" effect that continues to have a significant impact until the extinction of cohorts for which the increase was more marked (birth years 1920 to 1945). This factor alone explains 18% of the growth in the number of incident cases in 2018, while the effect of population growth accounts for 6.6%, the cessation of HTM a 6.4% decrease and population aging a 4.6% growth.20
The estimated age-specific risk for breast cancer in Europe shows an homogenous pattern with high risk for women over 50 with exception for Poland where the risk increases after 55-59 but remains lower in comparison with other countries in Europe (Figure 5).

Oceania
The PBCRs coverage for Oceania comprises 73% of the population of the region and represents 23 million people.
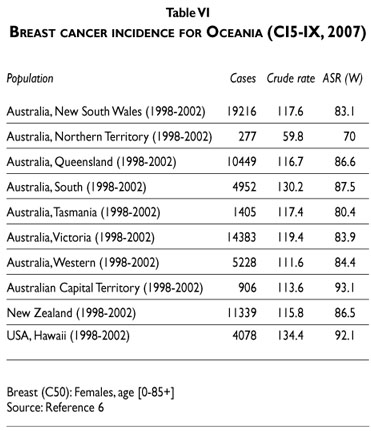
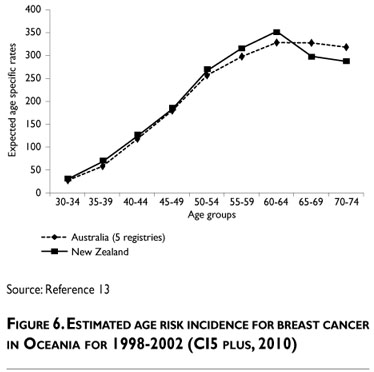
New Zealand and Australia have the highest rates of breast cancer, comparable to those of Europe and North America; however the rates are low in the islands where there is less migration and westernization. Ethnic disparities in breast cancer epidemiology exist in New Zealand. Pacific women may have decreased incidence rates of breast cancer but they present, as well as Maori women, with a more advanced stage of breast cancer than other women (Table VI).21 Estimated age-risk incidence in Oceania is alike in both countries with rates increasing in postmenopausal women, rates having the same patterns as those of Europe (Figure 6).
Mortality of breast cancer in the world
The estimated mortality for breast cancer rates in the world ranges from 6 to 29 per 100 000, resulting that breast cancer ranks as the fifth cause of death from cancer overall (458 000 deaths); but in spite of that, it is the most frequent cause of cancer death in women in both developing (268 000 deaths) and developed regions.1
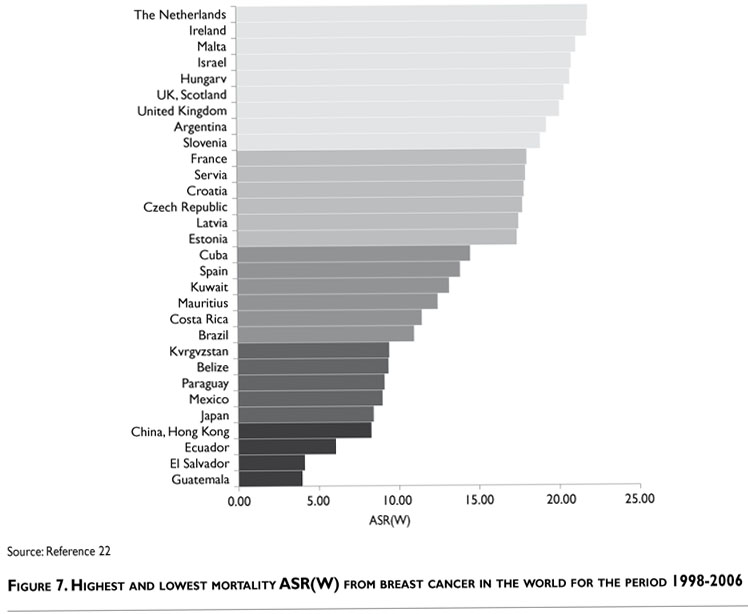
The coverage estimated by WHO mortality database22 ranges from 10 to 100%, being the lowest in lowincome countries. It refers to adult deaths and varies a lot. Figure 7 displays the highest and lowest mortality rates for breast cancer in the world based on WHO mortality database for the period 1998-2005 (http://apps.who.int/whosis/database/mort/table3.cfm - http://apps.who.int/whosis/database/mort/table4.cfm) Denmark, Netherland and Ireland had the highest mortality and countries from Latin America and Asia had the lowest mortality rates.
Africa
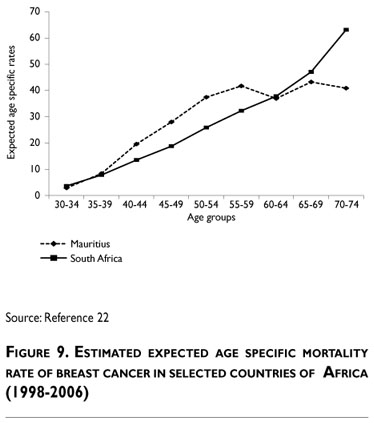
From WHO database, mortality rates for the period 1998-2005 are about 11 per 100 000 women for South Africa and Mauritius (Figure 8). There is lack of information on mortality for most of the countries in Africa. As the incidence rates are lower for breast cancer, it seems that mortality rates are 50% higher in relation to the incidence rates.

Age-specific mortality rates are higher in Mauritius than in SouthAfrica, except for the age group 70-74 which is higher in South Africa. Although the African population is young, the mortality increases in women over 50, identically to the western populations (Figure 9).
Asia
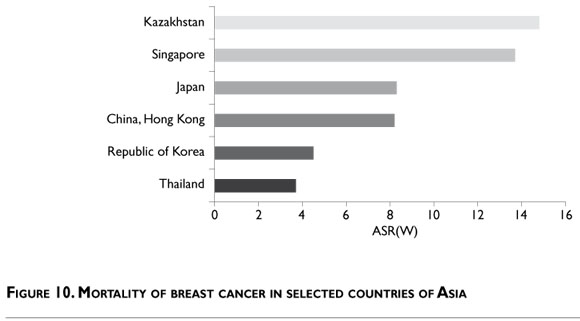
Mortality for breast cancer is lower in general and heterogeneous between the Asian countries. A recent analysis done by Katanoda et al, 2010, on 11 countriesduring the period 1990-2006 demonstrated that in three Asian countries/regions (Japan, Hong Kong and Korea) mortality was lower than in Western countries. Koreahad the lowest ASR among the three Asian countries/ regions. In Asia, an increasing trend was observed for the ASR in Japan and Korea, whereas the ASR in Hong Kong appeared to be slowly decreasing. After 1990, breast cancer mortality tended to decrease slightly in Hong Kong and Singapore except for women over 70. In Taiwan and Japan, in contrast, death rates from breast cancer increased throughout the entire study period. They rose more steeply in Taiwan, and after 1996 they began rising more rapidly in Japan than in Taiwan. The most rapid increase in breast cancer mortality, and for all age groups, was in Korea (Figure 10).23
Specific-age mortality burden in Asia has the highest impact in Israel based on WHO mortality data for the period 1998-2002, whereas Korea detains the lowest incidence rate by age group among these Asian countries. Singapore has rates comparable to Israel, and Japan has the intermediate rate for the same period (Figure 11).

North America
Breast cancer mortality is decreasing in USA among all races for the period 1972-2007 from 31 to 23 per 100 000 deaths in the last five years (the age-adjusted death rate was 24.0 per 100 000 women per year). These rates are based on patients who died between 2003 and 2007 in the US. The mortality rates are about 34 per 100 000 black women and about 25 per 100 000 white women in 2002.
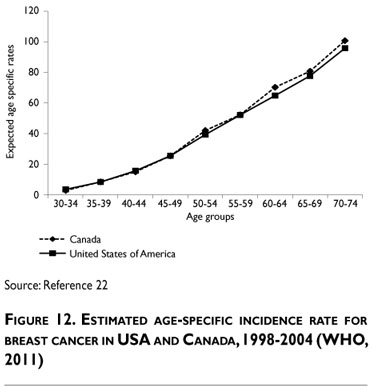
This data shows that mortality for black women in USA is higher than for white women. The median age at death from breast cancer in USA is 68, 20% of deaths being for the age group 45-64 (Figure 12).
Trends in mortality are significantly decreasing in USA in the last 10 years (http://seer.cancer.gov/faststats/).
Latin America
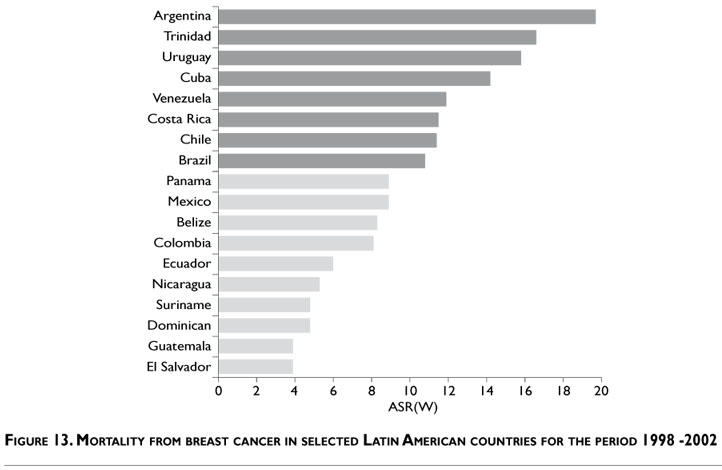
Mortality rates are about 20-10/100 000 in Latin American countries, the highest being in Barbados. Breast cancer mortality in Latin America is heterogeneous, being higher in Argentina and then in Trinidad and Tobago, which have two different patterns of population: Argentinean people descend more from European, whereas population of Trinidad is black. Mortality rates range from 5-20 per 100 000 in this continent but the rates are mostly about 5-12 per 100 000 (Figure 13).
Breast cancer mortality in Brazil is stable from 1980 to 2004, although the country doesn't have an organized screening program.24
In Caribbean, trend in Trinidad and Tobago during the last 35 years shows a pattern of mortality increase with increasing age. The mortality rate was considerably higher for the age groups over 50 than those below 50 years of age, both showing an upward trend over the 35-year old period.25
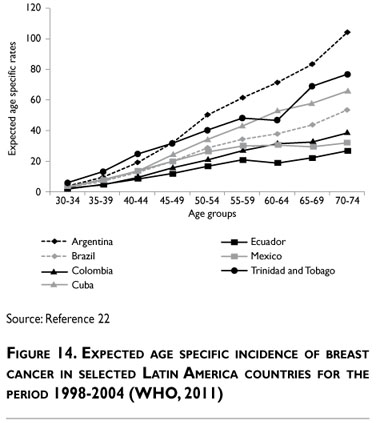
Regarding age-risk impact, it increases with age, being highest in Argentina and Trinidad and Tobago for women over 60. For the other countries, mortality is homogenous for women over 50 with an estimated risk of about 20-40 per 1000 000. The lowest mortality impact by age group is in Ecuador and Guatemala: less than 20 per 100 000 per age group (Figure 14).
Europe
Breast cancer mortality rates in Europe range from 7 to 25 per 100 000 women. The highest mortality rates are in Denmark, Netherland and Ireland. The lowest rates are in Spain, Bulgaria and Finland.
In Spain, mortality for breast has decreased for the period 1980 to 2007.26 From 2000 to 2004, the range of variation across Europe was relatively limited, i.e. between 25.9/100 000 in Denmark and 14.5/100 000 in Spain. In European countries, mortality rates have been substantially declining over the last two decades, whereas they have been stable or upwards in Russia and in most eastern European countries.
The largest EU countries (UK, Germany, France and Italy) had mortality rates between 18 and 20.5/100 000 and Russia of 17.3/100 000 (Figure 15).27
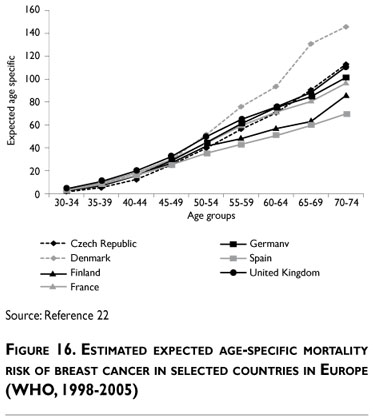
From 1998 to 2002, breast cancer mortality by age groups followed the same pattern as the incidence, being higher in postmenopausal women. The highest estimatedrates were in Denmark, Netherlands and UK (England and Wales) in women over 50. For other European countries as Spain, Portugal and Finland, the impact was lower in the same age group in comparison with Denmark, UK and Netherland. There are varied patterns in age group mortality within Europe (Figure 16).
Oceania
Data from Oceania shows an ASR(W) between 15-23 per 100 000 women for the period 1998-2002. There is no large variation between New Zeeland and Australia in the pattern of breast cancer mortality (Figure 17). However the estimated mortality byagegroupis higher in New Zeeland than in Australia for the same age group (Figure 18).


Final considerations
Breast cancer is the most common cancer in the world in women in this decade; however its incidence is decreasing in North America. In most of the countries in the world there is still a public health issue. In Africa there is a controversy regarding breast cancer incidence in premenopausal women having the worst prognosis, and further studies and information are needed to better understand the pattern of this tumor in Africa. Black women have high mortality even in developed countries as North America.
In Asia the breast cancer incidence rate is low and the mortality rate is high. The reason of this pattern in Asia is unknown.
Latin America has a heterogeneous pattern with high rates in South and in the Caribbean region and intermediate rates in Latin countries. Mortality is stable in most of these countries except in Trinidad and Tobago.
Europe has the highest incidence rates in the world and mortality is higher in Nordic countries as Denmark. The aging population in this continent is one of the major factors as the low fertility in most of the countries. Oceania has rates for incidence and mortality similar to those of the European continent.
A lot has been done to reduce the burden of breast cancer in the world as new treatment modalities, organizing screening programs which have improved the survival of the women diagnosed with breast cancer. The results are likely in developed countries but a lot needs to be done in developing countries to reduce mortality and incidence and to improve epidemiological information in the other populations.
Declaration of conflict of interests: The author declares not to have conflict of interests.
References
1. Ferlay J, Shin H-R, Bray F, Forman D, Mathers C, Parkin D. GLOBOCAN 2008: Cancer Incidence and Mortality Worldwide IARC Cancer Base, 1027-5614, No. 10. [web-site] 2010 [cited 2010]; v. 1.2: [Accessed 2010, July 12].Available from: http://globocan.iarc.fr/. [ Links ]
2. Launoy G. Epidemiology of cancers in France. Rev Prat 2010 20;60(2):178-182. [ Links ]
3. Jung KW,Won YJ, Park S, Kong HJ, Sung J, Shin HR, et al. Cancer statistics in Korea: incidence, mortality and survival in 2005. J Korean Med Sci 2009;24(6):995-1003. [ Links ]
4. Cao KJ, Fan QY, Liu YL, Huang R,Yin CZ, Ma GS, et al. [Cancer incidence and mortality in Guangzhou City from 2000 to 2002].Ai Zheng 2008;27(3):225-230. [ Links ]
5. Hery C, Ferlay J, Boniol M,Autier P. Quantification of changes in breast cancer incidence and mortality since 1990 in 35 countries with Caucasian-majority populations.Ann Oncol 2008;19(6):1187-1194. [ Links ]
6. Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al., eds. Cancer Incidence in Five Continents,Volume IX. IARC Scientific Publications No. 160. Lyon, France: International Agency for Research on Cancer, 2007. [ Links ]
7. Zanetti R,Tazi MA, Rosso S. New data tells us more about cancer incidence in North Africa. Eur J Cancer 2010;46(3):462-466. [ Links ]
8. Somdyala NI, Bradshaw D, Gelderblom WC, Parkin DM. Cancer incidence in a rural population of South Africa, 1998-2002. Int J Cancer 2010;127(10):2420-2429. [ Links ]
9. Huo D, Ikpatt F, Khramtsov A, Dangou JM, Nanda R, Dignam J, et al. Population differences in breast cancer: survey in indigenous African women reveals over-representation of triple-negative breast cancer. J Clin Oncol 2009;27(27):4515-4521. [ Links ]
10. Parkin DM, Nambooze S,Wabwire-Mangen F,Wabinga HR. Changing cancer incidence in Kampala, Uganda, 1991-2006. Int J Cancer 2010;126(5):1187-1195. [ Links ]
11. Ben Abdallah M, Zehani S, Maalej M, Hsairi M, Hechiche M, Ben Romdhane K, et al. [Breast cancer in Tunisia: epidemiologic characteristics and trends in incidence].Tunis Med 2009;87(7):417-425. [ Links ]
12. Sighoko D, Bah E, Haukka J, McCormack VA,Aka EP, Bourgeois D, et al. Population-based breast (female) and cervix cancer rates in the Gambia: evidence of ethnicity-related variations. Int J Cancer 2010;127(10):2248-2256. [ Links ]
13. Ferlay J, Parkin DM, Curado MP, Bray F, Edwards B, Shin HR, et al. Cancer Incidence in Five Continents,Volumes I to IX: IARC CancerBase No. 9 [Internet]. Lyon, France: International Agency for Research on Cancer, 2010. [Accessed 2011 July 31]. Available from: http://ci5.iarc.fr <http://ci5.iarc.fr/> [ Links ]
14. Registry NOfCPaCNCC. Chinese Cancer Registry Annual Report, 2009. Cancer Incidence and Mortality in Chinese Cancer Registration Areas in 2005. Beijing: Disease Prevention and Control Bureau, Ministry of Health, 2009. [ Links ]
15. Huang CS, Lin CH, Lu YS, Shen CY. Unique features of breast cancer in Asian women--breast cancer in Taiwan as an example. J Steroid Biochem Mol Biol 2010;118(4-5):300-303. [ Links ]
16. Leong SP, Shen ZZ, Liu TJ,Agarwal G,Tajima T, Paik NS, et al. Is breast cancer the same disease in Asian and Western countries? World J Surg 2010;34(10):2308-2324. [ Links ]
17. Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer 2010;46(4):765-781. [ Links ]
18. SEER Cancer Statistics Review, 1975-2007. National Cancer Institute. Bethesda; 2010 [ [ Links ]cited 2011]; [Accessed 2011 March 18]. Available from: http://seer.cancer.gov/csr/1975_2007/.
19. Fontenoy AM, Leux C, Delacour-Billon S,Allioux C, Frenel JS, Campone M, et al. Recent trends in breast cancer incidence rates in the Loire-Atlantique, France: a decline since 2003. Cancer Epidemiol 2010;34(3):238-243. [ Links ]
20. Bouee S, Grosclaude P,Alfonsi A, Florentin V, Clavel-Chapelon F, Fagnani F. [Projection of the incidence of breast cancer in France in 2018]. Bull Cancer 2010;97(3):293-299. [ Links ]
21. Lawes CM,Tukuitonga CF, Scragg RK.The epidemiology of breast cancer in Pacific women in New Zealand. N Z Med J 1999;112(1096):354-357. [ Links ]
22.WHO Mortality Database [database on the Internet]. WHO 2011 [cited 25/03/2011].Available from: http://www.who.int/whosis/mort/download/en/index.html <http://www.who.int/whosis/mort/download/en/index.html>.
23. Shin HR, Boniol M, Joubert C, Hery C, Haukka J,Autier P, et al. Secular trends in breast cancer mortality in five East Asian populations: Hong Kong, Japan, Korea, Singapore and Taiwan. Cancer Sci 2010;101(5):1241-1246. [ Links ]
24. Fonseca LA, Eluf-Neto J,Wunsch Filho V. [Cancer mortality trends in Brazilian state capitals, 1980-2004]. Rev Assoc Med Bras 2010;56(3):309-312. [ Links ]
25. Naraynsingh V, Hariharan S, Dan D, Bhola S, Nagee K.Trends in breast cancer mortality in Trinidad and Tobago--a 35-year study. Cancer Epidemiol 2010;34(1):20-23. [ Links ]
26. Cabanes A,Vidal E,Aragones N, Perez-Gomez B, Pollan M, Lope V, et al. Cancer mortality trends in Spain: 1980-2007.Ann Oncol 2010;21 Suppl 3:iii14-20. [ Links ]
27. La Vecchia C, Bosetti C, Lucchini F, Bertuccio P, Negri E, Boyle P, et al. Cancer mortality in Europe, 2000-2004, and an overview of trends since 1975.Ann Oncol 2010;21(6):1323-1360. [ Links ]
 Corresponding author:
Corresponding author:
María Paula Curado
International Prevention Research Institute (IPRI)
15, Chemin de Saquin, Espace Européen
69130, Ecully, France
E-mail: maria-paula.curado@i-pri.org
Accepted on: September 27, 2011


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}