










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.53 no.4 Cuernavaca jul./ago. 2011
ARTÍCULO ORIGINAL
Demand for care and nosocomial infection rate during the first influenza AH1N1 2009 virus outbreak at a referral hospital in Mexico City
Demanda asistencial y tasa de infección nosocomial durante el primer brote de influenza AH1N1 2009 en un hospital de referencia en la Ciudad de México
Rogelio Pérez-Padilla, MD,I; Rosario Fernández, MPH,I; Cecilia García-Sancho, MD, PhD,I; Francisco Franco-Marina, MD, MPH,I; Edgar Mondragón, MD,I; Patricia Volkow, MD,II
IInstituto Nacional de Enfermedades Respiratorias. México, DF, México
IIInstituto Nacional de Cancerología. México, DF, México
ABSTRACT
OBJECTIVE: Comparison of routine hospital indicators (consults at the Emergency Room (ER) and hospital admissions) during the 2009 pandemic of the influenza AH1N1 virus at the national referral hospital for respiratory diseases in Mexico City.
MATERIAL AND METHODS: The outbreak was from April to mid-May 2009 and two control periods were used:2009 (before and after the outbreak),and during April-May from 2007 and 2008.
RESULTS: During the outbreak total consultation at the ER increased six times compared with the 2007-2008 control period and 11 times compared with the 2009 control period. Pneumonia- or influenza-related ER consultations increased 23.2 and 15.3%, respectively. The rate of nosocomial infection during the outbreak was 13.6 and that of nosocomial pneumonia was 6 per/100 hospital discharges, a two-fold and three-fold increase compared to the control periods respectively.
CONCLUSIONS: During the outbreak,mean severity of admitted patients increased,with a rise in in-hospital mortality and nosocomial infections rate, including nosocomial pneumonia.
Key words: influenza A virus, H1N1 subtype; hospital care; 2009 pandemic influenza AH1N1; Mexico
RESUMEN
OBJETIVO: Comparación de indicadores hospitalarios de rutina (consultas de urgencia, admisiones hospitalarias etc.) durante la pandemia de influenzaAH1N1 2009 en un hospital de referencia para enfermedades respiratorias de la Ciudad de México.
MATERIAL Y MÉTODOS: El brote se consideró de abril a la mitad de mayo de 2009 y se comparó con dos periodos control: el de 2009 (antes y después del brote), y durante abril y mayo de 2007 y 2008.
RESULTADOS: Durante el brote las consultas de urgencia crecieron seis veces comparadas con el periodo control 2007-2008 y 11 veces contra el periodo control de 2009. Las consultas por neumonía o influenza incrementaron 23.2 y 15.3% comparadas contra los periodos control, respectivamente. La tasa de infección nosocomial durante el brote fue de 13.6 y la de neumonía nosocomial de 6.0 por 100 egresos hospitalarios, el doble y el triple de la documentada en los periodos control respectivamente.
CONCLUSIONES: Durante el brote, la gravedad promedio de los pacientes hospitalizados se incrementó, desencadenando un aumento en la mortalidad hospitalaria y en la tasa de infecciones nosocomiales, incluyendo la de neumonía nosocomial.
Palabras clave: Subtipo H1N1 del Virus de la Influenza A; atención hospitalaria; influenza pandémica AH1N1 2009; México
In April 2009, an outbreak of influenza occurred in Mexico. Among the strains detected during the epidemic, there was a novel pandemic influenza A strain (H1N1), an assortment of swine, avian, and human lineages.1-4 After a few weeks, the World Health Organization (WHO) declared a level 6 pandemic influenza alert for this, the first XXI Century influenza pandemic.5
Hospitals in Mexico City received an unusually high number of very sick patients with respiratory failure and high mortality, in addition to patients with pneumonia not requiring mechanical ventilation.6 But all of these patients overloaded referral hospitals. This manuscript aims to describe the increase in medical demand and hospitalizations during the epidemic outbreak of influenza in April and May 2009 at a referral hospital for respiratory diseases in Mexico City, the type of diagnosis associated with the outbreak, and the difficulties experienced. This may aid in understanding the demand for health care services and contribute to better preparation of hospitals for a new outbreak of influenza, or even for other epidemic respiratory diseases.
Material and Methods
This report was determined to be exempt from the requirement for institutional review since it was conducted as part of a public health investigation into retrospective data. INER is the Mexican National Institute of Respiratory Diseases, a national tertiary-care and research center devoted to respiratory diseases. The 178-bed facility provides clinical services primarily for the uninsured population of Mexico City and neighboring states. The influenza outbreak period was defined as the period between April 1 and May 15, 2009. A full health alert in Mexico was issued on April 23, 2009, with all schools and public activities suspended until May 6, 2009. The number of Emergency room (ER) visits, hospitalizations, and other hospital indicators during the outbreak period were compared with two control periods. The first control period comprised April 1 to May 15, 2007 and 2008; hospital indicators for this period are an average of those observed during these two years. The second control period covered 22 days prior to April 1, 2009 (March 10-31) and 23 days after May 15, 2009 (May 16 to June 7), both also totaling 45 days. We reviewed daily hospital statistics and administrative data, and compared outbreak and control periods.
For the ER, information was abstracted on the number of ER consultations, both in general and for specific diagnoses made by the consulting physician and coded according to the 10th Revision of the International Classification of Diseases (ICD-10), including community-acquired pneumonia-influenza (P-I) or influenza-like illness (ICD-10 codes J09-J18), upper respiratory tract infections (ICD-10 codes J00-J06), and acute respiratory failure and other respiratory diseases (ICD-10 codes J95J98, and J99.8). We also analyzed the number of patients admitted to the ER and the mortality observed during the three compared periods.
For hospitalized patients, we analyzed the hospital discharge database to obtain the number of hospitalized patients in each compared period and the number of deaths observed both in general and for patients with the discharge diagnosis of community-acquired Pneumonia-influenza (ICD-10 codes J09-J18). Finally, we obtained the number of nosocomial infections of any type and of nosocomial pneumonias during the compared periods. Our analysis of P-I and other respiratory infections is based on diagnoses by the physician, whether or not the patient had a positive test for H1N1 2009 infection, by a real-time Reverse-transcriptase-Polymerasechain reaction (RT-PCR) test performed in accordance with published guidelines from the U.S. Centers for Disease Control and Prevention (CDC).7 The analysis compared the number of events during the period of the outbreak and each control period (2007-2008) and 2009. Incidence rates of consultations, emergency room admissions and deaths from all causes were calculated and compared using incidence rate ratios. Proportions were compared using Chi-square test. The same analysis was done for indicators of hospitalization. Data analysis was conducted with STATA statistical software.*
Results
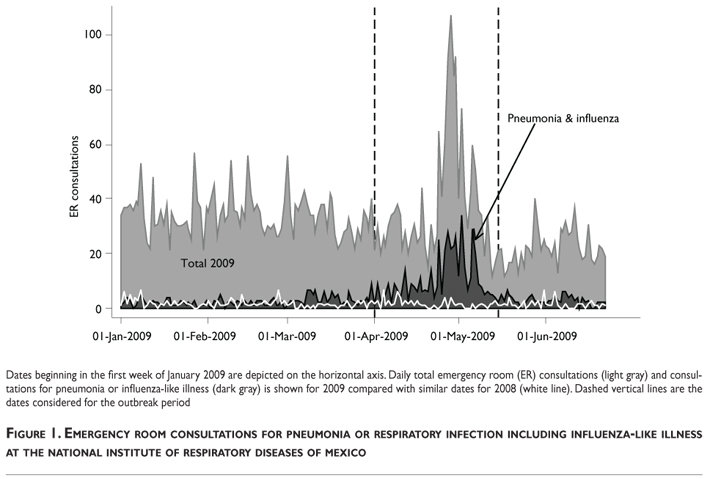
Figure 1 shows the total daily number of ER consultations (upper line) and the number of consultations with a diagnosis of pneumonia or influenza. Amild increase in ER consultations for pneumonia-influenza was observed during March, but rose especially on April 23, when the Mexican Epidemiological Emergency Alert was issued.During the outbreak, the proportion of pneumonia- or influenza-associated consultations increased from an average of 4.8% in the 2007-2008 period to an average of 28% (Table 1) (Figure 2). By May 1, total number of consultations had returned to baseline, but percentage of consultations due to pneumonia-influenza remained high for at least 2 additional weeks. Daily number of ER consultations, number of consultations attributed to pneumonia, influenza or to influenza-like illness (ILI) by the ER physician and the number of patients admitted to the hospital with the discharge diagnosis of P-I increased during the outbreak.

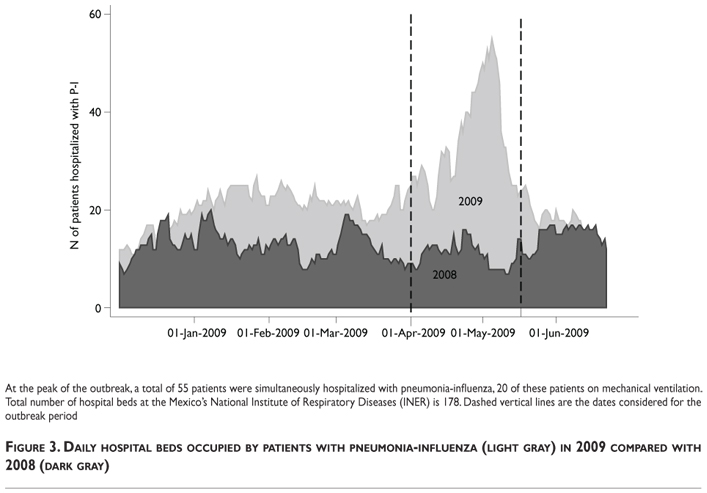
The outbreak period included 137 hospital admissions for P-I in 45 days compared with 50 in the 2009 control period and 29 in the 2007-2008 control period (Table 1). Figure 3 depicts the number of hospital beds occupied by day by patients with pneumonia and ILI. During the outbreak, we reached a maximum of 45 hospital-admitted patients with ILI and pneumonia, with 13 of these with endotracheal-tube mechanical ventilation. This was an impressive surge in the number of patients, as can be observed when compared with 2009 (p=0.03). During January and February 2009, more patients were hospitalized with pneumonia-influenza than during the corresponding months of 2007-2008 (P=0.03).
Nearly all of the patients (83.8%) cared for at INER reside in the Mexico City metropolitan area, and the proportion persisted in patients with P-I and did not change significantly during the compared periods.
The nosocomial infection rate (13.6 per 100 hospital discharges) and the nosocomial pneumonia rate (6.0 per 100 hospital discharges) during the outbreak doubled those in the control periods (6.2, 8.1, and 1.9, 2.4 per 100 hospital discharges, respectively) (Table 1).
The in-hospital mortality rate for all admitted patients during the outbreak was 12.8%, versus 9.4% in 20072008 control period (p=0.1) but not significantly higher than that of the 2009 control period (9.4% versus 10.2%, p=0.6). The fatality rate for P-I during the outbreak was 21.2%, lower, but not significantly different from, the control periods at 38 (p=0.05) and 34% (p=0.07), respectively. Daily number of ER consultations (total, and P-I-related), hospital admissions and deaths for P-I, and the percentage of P-I-associated ER consultations and admissions increased significantly during the epidemic period compared with control periods (Table 1).
Discussion
The April-May 2009 influenza H1N1 epidemic resulted in an increased demand for hospitals able to receive patients with respiratory failure, such as the respiratory-diseases referral center source for this report. Patients with pneumonia and ILI require more care and infection control precautions than the more frequently observed patients with non-infectious chronic diseases, even during disease exacerbation. In addition, patients with ILI were often young and previously healthy, generating a great emotional impact on their families, but youth is a good prognosis sign for survival and rehabilitation compared with pneumonias occurring in older age with comorbidities from influenza like illness in control periods.
The number of hospital beds for patients with ILI and pneumonia was increased progressively by deferring elective surgical procedures and related consultations. Consequently, the average severity of admitted patients increased, with patients under mechanical ventilation being situated outside of the customary areas, i.e., intensive care unit (ICU); ER, and recovery room. Patients with P-I admitted to the hospital required isolation, standard and respiratory precautions,and one third of these, mechanical ventilation, with many more invasive interventions than patients usually admitted to non-critical areas. Patients on mechanical ventilation outside the ICU lacked specialized nursing to care for critically ill patients, at least on some shifts. Despite much higher compliance with hand washing and disinfection and use of face masks, hospital coats,and gloves, overall hospital mortality increased, as well as the rate of nosocomial infections. Compared to non-pandemic periods, case-fatality for pneumonia was slightly lower although non-statistically significant, maybe because the average age of patients with pneumonia during the pandemic was much younger[mean, ±standard deviation 44(±21.4), 66 (±27.5) and 50.7(±25.0) for pandemic period versus non-pandemic periods, respectively].
The burden of the epidemic was produced by all patients with ILI and pneumonia, and not only by the fraction of patients who tested positive for the novel H1N1 virus, who were the only patients counted officially by the WHO and in many countries. During the epidemic's peak, some patients did not provide a respiratory secretions sample for testing, or the sample provided was of poor quality or delayed. Our patients arrived at the ER on average 6 days after symptoms initiation,6 compared with 3 days in hospitalized patients reported in the U.S. by the CDC.8 On the other hand patients who tested negative for the pandemic H1N1 virus were similar in number than those who tested positive, and both were part of the same epidemic6 and in need of hospital care. Counting only confirmed cases produces an underestimation of the epidemic's extension and severity. It is known that up to 3.8 times more deaths may be attributable to an influenza epidemic than deaths certified as influenza or pneumonia.9 Some of these deaths are certified as cardiovascular or cerebrovascular,9 common causes of death in the population. At our hospital, we found no increase in pulmonary thromboembolism during the epidemic, but we do not often receive patients with other cardiovascular events, such as acute myocardial infarction or cerebrovascular accidents, because there are other hospitals specialized in cardiac and neurologic diseases in the city.
During the influenza outbreak, the total number of ER consultations increased, as well as the proportion of influenza-and pneumonia-related consultations (Figure 2). We found no increase in asthmatic crises or chronic obstructive pulmonary disease (COPD) exacerbations, nor an increase in visits of patients for other respiratory problems, except for upper airway infections, respiratory failure, and P-I. In hospitalized patients, the pattern was similar: an increase in admissions for P-I, but not for other diseases.
During the outbreak, a key part of the hospital response was the increase in beds for patients with respiratory failure who required mechanical ventilation. The hospital was obliged to convert a 30-bed ward for influenza treatment, including beds for mechanical ventilation. Having beds and ventilators comprises only one part of the requirements: also essential are trained personnel for all shifts, as well as medicines, protective equipment, and general supplies. Each of these requirements resulted in a bottleneck throughout the outbreak at different times. It is clear to us that during an influenza epidemic, one priority is to assign ICU beds to patients with influenza by halting elective surgery, because trained personnel, equipment, and supplies must accompany these standard beds. As a second step, and after displacing as many ICU beds as possible for patients with influenza, there follows expanding the number of beds with mechanical ventilators outside of the ICU, providing that we are able to resolve shortages in personnel, equipment, and supplies. Collaboration among neighboring hospitals provided aid in their receiving a small number of patients, although this procedure was questioned by the patients' relatives and was difficult to implement. Transfer of patients with influenza was difficult because they were frequently hemodynamically unstable and required vasoactive drugs and high respiratory pressures.
Our hospital had pandemic influenza plans in place since 2006 and in October 2008 we enacted a pandemic simulation drill only 6 months prior to the real pandemic, although the latter was not H5N1-associated. These preparations were helpful, but real exposure to the pandemic demanded a day-to-day awareness of unmet needs in medical supplies and drugs that built up a much more complete plan, which was again tested during the pandemic's second wave, which began in September 2009 and which doubled the initial demand for health care services produced during the first wave described herein. For this second wave oseltamivir was readily available, the personnel had acquired experience, and supplies were adequate and although the load of patients was bigger, the preparation for this second wave was better and the clinical care of these cases was almost routine.
In conclusion, the April-May 2009 outbreak of the influenza pandemic was accompanied by a large rise in the need for beds for patients on mechanical ventilation with trained proper personnel and supplies. The load was formed by pandemic H1N1-positive patients, as well as by those who were negative or not tested, all of them part of the same epidemic, which was significantly underestimated by counting only pandemic H1N1-positive patients. The nosocomial infection rate in this period increased probably due to the presence of a larger number of patients on mechanical ventilation and dialysis procedures.
Acknowledgments
The INER Working Group on Influenza also comprises: Ariel Corrales, Jair Rodríguez, Miriam Barrales, Lilian Reveles, Miguel Ángel Sánchez-Mecatl, David Ibarra, Lilia E. León, Teresita Gutiérrez, and Daniel Rodríguez-Parga (emergency room), Édgar Bautista, Cristina Aguilar, Fidel Rocha, Ismael Serna, Víctor Huízar, Benjamín Castañeda, and José Guadalupe García (intensive care), José Luis Sandoval, Rafael Hernández, Fernando Flores, Carlos Espinoza, Alejandra Ramírez, and Jorge Morales (influenza ward), Francisco Quiñones, Eduardo Sada, Gustavo Reyes-Terán, Javier Romo, and Christopher Ormsby (infectious diseases), Alejandra Osorio and Édgar Sevilla (hospital epidemiology), Alejandro Alejandre (pediatric pulmonology), Sergio Rodríguez-Filigrana, Verónica Sosa and Jorge Chavarría (medical management), Andrés Hernández, Anjarath Higuera, Jazmín Godínez-Zavala, and Leticia Martínez (epidemiology), Lilia Damián (nursing department), Rogelio García-Torrentera (respiratory care), Roberto Sotelo and Luis Felipe Alba (chest imaging), María Eugenia Vázquez and Erika Peña (pathology), Moisés Selman-Lama, María Eugenia Manjarrez, and Joaquín Zúñiga (research unit), and Jorge Salas (teaching).
Declaration of conflict of interests: The authors declare that they have no conflict of interests.
References
1. CDC. Update: infections with a swine-origin influenza A (H1N1) virus-United States and other countries, April 28, 2009. MMWR Morb Mortal Wkly Rep 2009; 58:431-433. [ Links ]
2. CDC. Swine Influenza A (H1N1) infection in two children--Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep 2009; 58:400-402. [ Links ]
3. CDC. Update: swine influenza A (H1N1) infections--California and Texas,April 2009. MMWR Morb Mortal Wkly Rep 2009; 58:435-437. [ Links ]
4. Dawood FS, Jain S, Finelli L, et al. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med 2009; 360:2605-2615. [ Links ]
5. WHO. Pandemic Influenza, 2009. [ Links ]
6. Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med 2009; 361:680-689. [ Links ]
7. CDC. CDC protocol of realtime RTPCR for swine influenza A (H1N1). Geneva: World Health Organization, 2009. [ Links ]
8. Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients with 2009 H1N1 influenza in the United States,April-June 2009. N Engl J Med 2009; 361:1935-1944. [ Links ]
9. Simonsen L, Clarke MJ,Williamson GD, et al. The impact of influenza epidemics on mortality: introducing a severity index.Am J Public Health 1997; 87:1944-1950. [ Links ]
 Correspondence author:
Correspondence author:
Dra. Patricia Volkow
Instituto Nacional de Cancerología (INCan)
Av. San Fernando 22, col. Sección XVI. 4080
Tlalpan1 México, DF, México
E-mail pvolkowf@gmail.com
Received on: November 2010
Accepted on: August 2011
* StataCorp. Stata statistical software: Release 9.0 College Station, TX,USA: Stata Corporation; 2005.


{kind=link}
{kind=link}
{kind=link}