










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.53 no.4 Cuernavaca jul./ago. 2011
ARTÍCULO ORIGINAL
Does food insecurity compromise maternal dietary Zinc or energy intake in favor of her child, in rural poor Mexican households?
¿En hogares rurales pobres de México, la inseguridad alimentaria compromete el consumo de zinc y energía de las madres en favor de sus hijos?
Karla Moreno-Tamayo, MSc,I; Teresita González de Cossío, PhD,II; Mario Flores-Aldana, PhD,II; Sonia Rodríguez-Ramírez, MSc,II; Luis Ortiz-Hernández, PhD.III
ICentro de Investigación en Evaluación y Encuestas, Instituto Nacional de Salud Pública. Cuernavaca, Morelos, México
IICentro de Investigación en Nutrición y Salud, Instituto Nacional de Salud Pública. Cuernavaca, Morelos, México
IIIUniversidad Autónoma Metropolitana, Unidad Xochimilco. México DF, México
ABSTACT
OBJECTIVE: To analyze quantitative indicators of food insecurity (FI), and estimate if FI modifies the association between maternal and child Zinc and energy intake as evidence for maternal dietary compromise in favor of her child.
MATERIAL AND METHODS: Cross-sectional study (n=2 563), data derived from baseline impact evaluation of the Mexican Programa de Apoyo Alimentario. Quantitative indicators of FI were:Household food storage, maize and/or bean production, food expenditure, and spatial access to food markets. We evaluated percentage adequacy of energy (PAE) and Zinc (PAZn) intake. Multiple linear regression model was fitted to estimate the association between maternal and child PAE and PAZn.
RESULTS: Child PAE and PAZn were positively associated with those of their mothers. None of the FI indicators modified the association between maternal and child PAE and PAZn.
CONCLUSIONS: No evidence of maternal dietary compromise in favor of her child was observed using four quantitative indicators of FI in central-southern rural Mexican househods.
Key words: food security; maternal diet; preschool child diet; rural Mexico
RESUMEN
OBJETIVO: Analizar indicadores cuantitativos de inseguridad alimentaria (IA) y estimar si IA modifica la asociación del consumo de energía y zinc en madres e hijos como evidencia del compromiso de la dieta materna a favor de su hijo.
MATERIAL Y MÉTODOS: Estudio transversal,información basal de la evaluación de impacto del Programa de Apoyo Alimentario. Indicadores de IA: reserva de alimentos en hogar, autoproducción maíz y/o frijol, porcentaje del gasto en alimentos y acceso físico a mercados de alimentos.Se calculó el porcentaje de adecuación del consumo energético (PAE) y Zinc (PAZn) (n=2 563 pares). Se estimó un modelo de regresión lineal ajustado por covariables.
RESULTADOS: El PAE y PAZn de madres e hijos se asoció positivamente. Ningún indicador de IA modificó la asociación entre PAE y PAZn materno con respecto a sus hijos.
CONCLUSIONES: Los indicadores de IA estudiados no modifican la relación entre la dieta de madres-hijos en hogares rurales de México.
Palabras claves: seguridad alimentaria; dieta de la madre; dieta del niño preescolar; México rural
In the World Food Summit of 1996 it was agreed upon that food security exists when all people, at all times, have physical and economic access to sufficient safe and nutritious food to meet their dietary needs and food preferences for a healthy and active life.1 Some adverse effects on health have been documented in individuals from food insecure households, such as changes in cognitive development, poor reproductive outcomes in women, physical deterioration and psychological distress.2 Frequently accepted dimensions of food security include food access, availability and utilization. Food insecurity affects the quantity and quality of food consumption and, through these, nutritional status and physical well-being.3,4 Because of the multi-dimensional nature of food insecurity, it may be measured in many forms and attention needs to be paid as to not oversimplify or misunderstand its core meaning.5 Initially, household food availability was used to assess the existence of food insecurity.4 Subsequently, important scales focusing on subjective experiences of hunger were developed. A common practice is to validate scales of subjective experiences, having the food inventories as standard.6,7 However, it has been agreed upon that there may not be a unique measurement of food security that would capture all its dimensions.8 Thus, food insecurity can and has been measured through different angles, some focusing in the actual physical problems of access of food within and around households, others on purchasing power and still others on the perceived effect of such limited access.
The Radimer/Cornell hunger scale was originally developed in the nineties to qualitatively estimate the prevalence of perceived hunger in a sample of poor New York State households. This scale identifies those experiencing hunger through a household member reported experience of food insecurity.3 Based on this questionnaire, on the "Community Childhood Hunger Identification Project" (CCHIP), and on other US sources of information on this topic,9 a Food Security Scale (FSS) was developed to estimate food insecurity prevalence in that country. This is a widely used questionnaire that focuses on the effect of limited resources on food acquisition and the consequent experiences of hunger at the household level.10
The 1996 World Food Summit Food Security description suggests that measurement of the different dimensions of food security in a given setting would document its state relative to the defined construct. As an example of this association between measures of perceived food insecurity and other direct measures of some of its quantitative dimensions, a Mexican study conducted in a rural isolated community in Sierra de Manantlán revealed that more than 90% of households experienced some level of food insecurity as measured by the FSS, and that this was negatively correlated with household food inventory and individual maternal diet variety.6 Other LatinAmerican countries have employed different indicators such as household food inventory,7 or the Basic Food Basket or the evaluation of internal adjustment strategies that poor households implement to cope with economic crisis in Venezuela.11 Again, as expected, these studies show that food diversity is compromised in food insecure household.6,11
Access to food has been estimated only recently in Mexico through a study representative of its rural areas.12 This study documented that constant access to food markets, especially those distributing fresh foods, is limited in rural areas and that this situation is especially critical for indigenous populations. This information suggest that measuring actual food access with indicators of presence, type and distance to food distribution points, considering transportation, may be critical in the estimation of food insecurity. Different dimensions of food security need to be assessed to obtain a more equilibrated image of particular populations, as had been suggested by Pinstrup-Andersen.13
In high income countries, a negative association has been reported between food insecurity and dietary quality in adult men and women.14,15 In the United States and Canada, vitamin, mineral and energy intake has been found to be lower in women living in households with food insecurity than in food-secure households(16-20) though this association was not observed for preschool children.16,18
It has been shown that each household member experiences food insecurity differently. Adults, especially women, suffer its negative impact before children do, a phenomenon that could be interpreted as a form of protection of the child food intake.3,17,21 Few studies have attempted to answer the question of whether mothers compromise their consumption to protect their children as the level of food insecurity rises. Compromised dietary consumption by mothers in favor of the children was documented in a study of single Canadian mothers, in which food insecurity occurred in 78% of households.22 The study found that women reduced their intake of seven vitamins and two minerals, whereas only reductions in folate and Zinc intake were observed in their children.
One can study this maternal dietary compromise in terms of dietary quantity, and energy would be the selected indicator; or in terms of dietary quality. The latter would need an element that singles out meaningful dietary quality. In Mexico, the 1999 National NutritionSurvey showed that Zn is highly deficient in the diet ofrural children and women.23 Its prevalence in rural areas was 24.7% in children < 2 years , 55.8% in children 3-4years, and 33.9% in women.23 Due to these findings, Zn has in fact been used, along with other key micronutrients, as a fortification element in national nutrition programs based on its potential to promote healthy growth.24,25 Programs currently using Zn as a fortifier include Oportunidades, which distributes a complementary micronutrient fortified food for young children, or Liconsa which distributes fortified milk to poor households with children <12y. Together these programs reachmore that 30 million households every day.26
The aim of this study was to evaluate a potential maternal dietary compromise (in quantity or quality as estimated by energy and Zn adequacy of intakes respectively) in favor of her preschool child, using ad-hoc developed quantitative indicators of food insecurity, in rural households in central-southern Mexico.
Material and Methods
Study design and sample
A cross-sectional study was carried-out using baseline information from the impact evaluation of the Mexican Programa de Apoyo Alimentario (PAL, "Food Assistance Program").27 The PAL is directed toward the poorest population in rural Mexico living in communities without schools and/or health centers. Due to these conditions, such communities are not eligible for the largest governmental Human Development Program Oportunidades. To evaluate the PAL, 208 communities with the same degree of poverty and development characteristics were randomly selected from eight states in central-southern Mexico (Campeche, Chiapas, Guerrero, Oaxaca, Quintana Roo, Tabasco, Veracruz and Yucatán). Thirty-three households were selected through a systematic random method within each community. Fieldwork was conducted from October 2003 to April 2004. A sample of 2 133 mothers aged 1249 years (who may have had more than one preschool child) and 2 563 non breastfeeding children aged 6-59 months was studied. In total, the sample analysis was composed by 2 133 mothers 20% of whom had two children in the study, so that there were 2 563 children, all with complete dietary information. The study was approved by the Biosecurity, Ethics and Research Commissions at the National Institute of Public Health (INSPfor its Spanish name) and written informed consent was obtained from mothers.
Data were collected by trained personnel who conducted one 24-hour dietary recall. When possible, food similar to that reported as consumed, was weighed at home. When not possible, weights were estimated using standard household measurements (e.g., glass, cup or spoon). Nutrient dietary content and adequacy of intake were calculated based on the dietary information28,29 using the nutrient composition database compiled by the INSP which is based on various sources.30 Information on whether or not the child was breastfed was available. Though we had information on frequency of breastfeeding, no milk consumption data was obtained. We considered we could not derive valid estimates of breast milk consumption so dietary energy could not be quantified for breastfed children. Thus breastfed children were excluded from the analysis.
Household-level food insecurity indicators
Our data set does not contain measures of perceived food security as estimated by the FSS. It does, however, contain quantitative measures of different components of food security as shown in Figure 1.
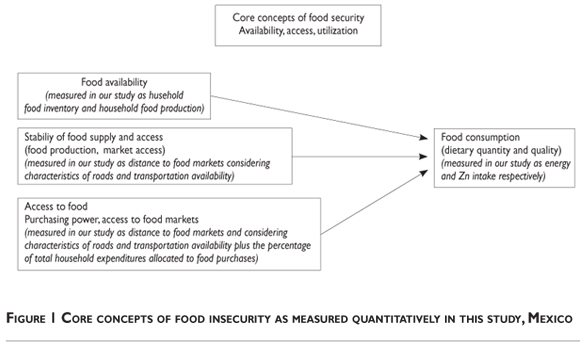
A household food availability indicator was developed based on a) food inventory and b) household food production. Afood access indicator was developed considering both a) economic and b) spatial access to local food markets.
Food availability indicator through a food inventory. a) We calculated the amount of food stored at home (in grams and by food groups) adjusted per adult equivalent (AE) using information on a household food inventory performed the day of the interview. Foods were classified into seven groups: 1) fruits and vegetables (e.g., onion, tomato, chard, avocado, zucchini, chayote, chili, lime, apple, banana, watermelon, carrot); 2) cereals and tubers (tortilla, oatmeal, amaranth, rice, maize flour, wheat flour, cookies, crackers, bread, pasta, potato, or yucca); 3) legumes (beans, lentils, chickpeas, or soy); 4) animal food sources (milk and dairy products, eggs, cheese, beef, chicken, pork, pork rinds, sardine, or tuna); 5) industrialized foods (pastries, sodas, chips, mayonnaise,instant soups, oil, sugar, powdered soft drinks, coffee, powdered or hard chocolate, jello, catsup, hot chili salsa), 6) nuts (sesame seeds, almonds, peanuts, walnuts, or pumpkin seeds) and 7) seasoning (garlic, basil, cumin, cinnamon, cloves, thyme, hibiscus flower, bay leaves, chamomile, oregano, pepper, or mint). Adult equivalent (AE) was estimated according to the dietary energy requirement for age, sex and physiological status of each household member. Energy for an adult was considered to be the equivalent of 597.5 kJ/d (2500 kcal/d recommended for an adult).29 Correlation between amounts of food group was estimated. To identify patterns across data and reduce it to one variable, principal component analysis was performed on data with 2 093 households with complete information. After varimax rotation, three factors with eigenvalues >1.0 were identified. Each factor was studied according to the percent of variance explained, its profile and interpretability (other solutions are available upon request). We chose to use items with factor loadings >0.331-33 based on the distribution of loadings within a factor an across factors, and retained the first factor which explained 25% of variance and was the most relevant (see Table II).

Food availability indicator through household food production b) Household food production was defined as a dichotomous variable based on whether or not the household consumed any amount of maize and/or beans produced by the household within the seven days prior to the interview. These two food items are the country's main staples, so that the consumption of either one may be considered at the root of the peasants' survival strategies and cultural preferences.34
Food access indicator: a) Economic access. This was measured using the percentage of total monthly householdexpenditure spent on food. Total estimated household expenditure included expenditure in the following items: food, transportation, cleaning products, health care, education, fuel, electricity, rent, clothes, and expenditure in special ceremonies. Information on these expenses were obtained on different time frames; i.e., weekly, monthly,annually; and calculated as monthly total expenditure
Food access indicator: b) Spatial access index developed based on: distance to food markets and time from home to market, using information of place of food purchases (local store, weekly local market, weekly produce market, regular or irregular produce vending trucks, street stallholder, local domestic production, supermarket or small grocery store) and traveling time (min) to the place of food purchases. The latter was estimated considering topographic conditions through travel time isochrones using the geographic information system ArcInfo Version 8.3 according to classifications for local land communication routes available at the time of the study.* Each food market spot calculated to be within 30 min from the household was assigned a score of 0.5; otherwise, a score of zero. The total points from spatial access food index were obtained and higher values were considered to reflect greater spatial access to food. The index was categorized on zero, one, and two or more close local food markets.
Diet quality and maternal compromise
We estimated maternal adequacy of energy and Zinc intake28,29 as a function of the adequacy of the child's intake adequacy. Using this approach, it is possible to evaluatewhether mothers compromised their dietary consumption in favor of her children. The study hypothesis is that as the severity of food insecurity increases, the consumption of the mother decreases relative to that of her child. The association between the mother's consumption and that of her child's would be negative, indicating the existence of a compromise on the part of the mother in the presence of food insecurity. We chose to analyze Zincas an indicator of dietary quality because is one of the most important nutrient to achieve adequate health and development of human capital in a population.25
Covariates
Children's and mothers' variables were included as covariates. The child sex, age and nutritional status were included. Three indicators of nutritional status were used: underweight, wasting and stunting, classified by the z-score values (< -2) of the weight-for-age (WAZ), weight-for-height (WHZ) and height-for-age (HAZ) indexes, respectively. The 2006 World Health Organization (WHO) international standards were used to construct the indices.35 Maternal age and marital, physiological and nutritional status were also covariables. In mothers aged <18 y, body mass index (BMI) was adjusted by cut-off points suggested by Cole.36 In adult mothers cut-off points suggested by the WHO37 were used. The following household covariables were included: head of household sex; indigenous condition (if at least one person in the household over 17 years spoke a native language); and percentage of household members <5 y (number of children <5 / total household members). Using information from type of floor, wall and ceiling construction material, number of rooms (not including kitchen or bathrooms), sanitation service, electricity, and possession of refrigerator, gas stove, television, radio, VCR, telephone and computer a socioeconomic index was determined. The index was generated by principal component analysis, which explained 43.6% of the variance in the first factor. The index was divided into tertiles: low, medium and high. Since it was detected that some households were registered in social programs (even if residing in communities where the programs did not formally operate), participation in social programs was considered by adding up the number of programs in which the members of the household were registered. This variable was dichotomized as none, and one or more. Some social programs had a specific nutritional components (nutritional supplement for children from Oportunidades, Free Tortilla, Milk Supply Program, Food Baskets and School Lunch) while others had different contents (cash transfer and scholarships from Oportunidades, transportation scholarships, Popular Health Insurance, Productive Options and Temporary Employment).
Statistical Analysis
Medians, inter-quartile ranges and frequencies of each variable were calculated. According to the scale of variables, the association among dependent, independent and covariables was evaluated using the Pearson, Spearman, point bi-serial or phi correlation coefficients.
The association between food insecurity and maternal adequacy of intake was estimated using a linear regression model for energy and another for Zinc, adjusting for covariates and for clustering effect to indicate that observations may be correlated. We did this because mothers in our sample may have had more than one child in the study, resulting in a lack of independence between siblings' data. We calculated our estimates with and without siblings in the sample, and did not find evidence that including siblings had an effect on our estimates. Therefore we adjusted for the clustering effect.
Maternal adequacy of intake was the outcome variable. We included interaction terms between each food insecurity indicator and child adequacy of intake to evaluate the potential different association between maternal and child intake depending on different levels of food the insecurity indicators. The resulting model is presented in Equation (1):

Where y is maternal adequacy of intake, b represents the regression coefficient term, Xi represents each food insecurity indicator, Z is the child adequacy of intake, is the interaction term, and  refers to the series of relevant covariables. Equation (1) illustrates the effect on maternal adequacy of intake per one-unit change in child adequacy of intake taking into account indicators of food insecurity. Interaction terms were not statistically significant so that Equation (1) became:
refers to the series of relevant covariables. Equation (1) illustrates the effect on maternal adequacy of intake per one-unit change in child adequacy of intake taking into account indicators of food insecurity. Interaction terms were not statistically significant so that Equation (1) became:

Statistical differences were considered when p<0.05. Data was processed using STATA/IC version 10.1.**
Results
Descriptive analysis
Table I presents child, maternal and household-level characteristics in the studied sample. Child and maternal median adequacies of energy intake were less than 100% (70.1% and 83.1% respectively). Median child adequacy of Zinc intake was 120.4%, whereas maternal was 77.2%. The prevalence of child wasting in these very poor communities was very low but stunting was high (0.9 and 19.9% respectively). Prevalence of maternal underweight was low. However, their prevalence of excess weight was quite high; more than half of the mothers were overweight or obese (56.4%). Twenty percent of the households were considered indigenous and approximately 40% participated in some social program.
Descriptive analysis of the food insecurity indicators developed in this study is shown in Table II. The industrialized food group was the most frequent in the households (366g/AE), followed by cereals and tubers (232.1g/AE), and finally legumes (198.1g/AE). Through the principal component analysis, legumes, cereals and tubers showed the greater and most positive correlation factor loadings. On the other hand, animal food products had negative correlation. Approximately 40% of this population produced their own maize and or beans which they consumed the week prior to the interview. Median household maize and beans production was 2695g/AE. More than half (54.9%) of the total household expenditure was on food. Around three quarters (74.5%) of households had access to food markets from at least one source located less than 30 minutes away.
Bivariate associations
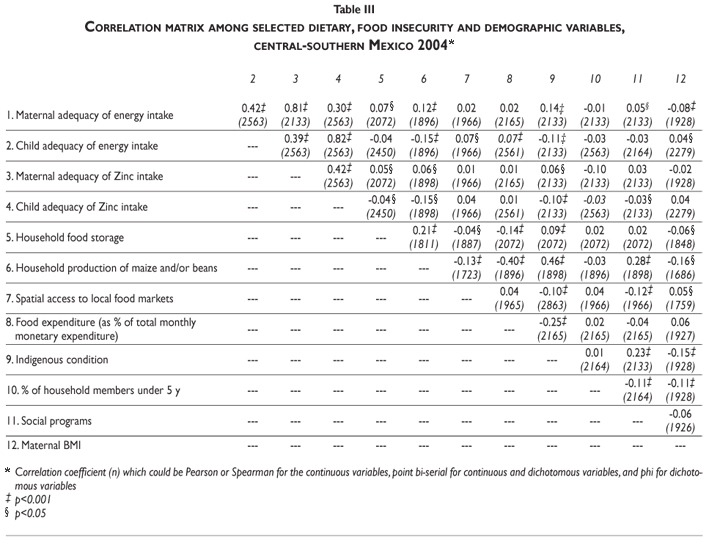
Table III shows a correlation matrix among selected dietary, food security and demographics variables. Household food production of maize and/or beans had a positive correlation with household storage but a negative one with food expenditure (as % of total monthly monetary expenditure) and with spatial access to local food markets. For mothers, household food storage and production of maize and/or beans showed a positive correlation with their own adequacy of energy and Zinc intake. Indigenous household condition showed positive correlation with maternal adequacy of energy and Zinc intake, household production of maize and/or beans, household food storage and with participation in social programs. It was negatively correlated with spatial access to local food markets, food expenditure (as % of total monthly monetary expenditure), and child adequacy of energy and Zinc intake.
Maternal and child adequacy of intake
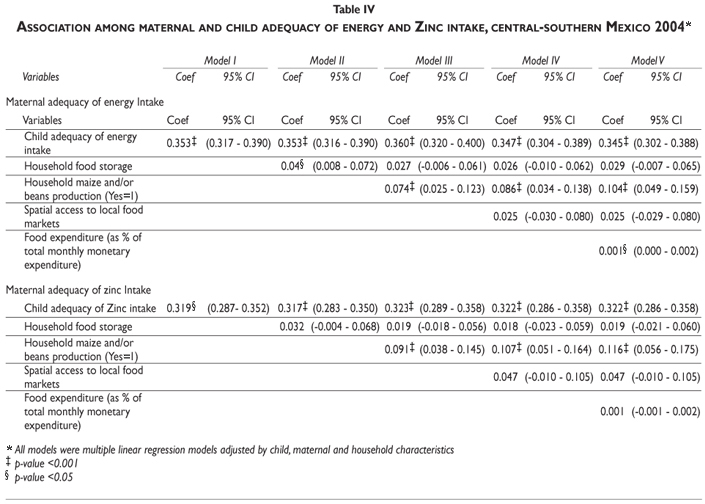
The association between maternal and child adequacy of energy and Zinc intake is showed in Table IV. Five models were estimated. Model I presents the association adjusted by child, maternal and household characteristics without food insecurity indicators. Subsequent models examine the relationship when food insecurity indicators were added, as described next. Model II included food household storage, model III was model II plus household production of maize and/or beans, model IV was model III with the addition of spatial access to local food markets and model V was model IV plus the variable that indicated food expenditure (as % of total monthly monetary expenditure). Both energy and Zinc child adequacies were positively associated with maternal adequacy in all models (p<0.001). Model II shows that food household storage was associated positively with maternal adequacy of energy (p<0.05)but not with adequacy of Zinc intake (p>0.05). The association was not significant after adjustment for the other food insecurity indicators. Household production of maize and/or beans was positively associated with maternal adequacy of energy and Zinc intake (p<0.001)and the magnitude increased by adding all the food insecurity indicators.
Food expenditure (as a percentage of total household monthly monetary expenditure) was positively associated with maternal adequacy of energy intake (p<0.05) but not with adequacy of Zinc intake (p>0.05).Lastly, spatial access to local food markets was not associated with maternal adequacies of intake (p>0.05).
Table V shows regression models fitted to determine the presence of maternal diet compromise in favor of her child. Other variables statistically associated with maternal adequacy of energy intake were an indigenous condition (p<0.001) and whether the mothers were breastfeeding (p<0.05). On the other hand, there was a negative association between maternal adequacy and social programs (p<0.001); with mothers being single, divorced or widowed (p<0.001), and their BMI (p<0.05).
The adequacy of Zinc intake was examined using an independent final multivariate regression model (Table V). Maternal adequacy of Zinc intake was positively associated with household production of maize and/or beans and with the indigenous condition of the household. Child age had a positive association with maternal Zinc intake. Breastfeeding was negatively associated with the adequacy of Zinc intake; being single, divorced or widowed mothers was negatively associated with both adequacies of intakes.
Discussion
Our study sought to evaluate whether mothers compromised their dietary consumption in favor of their child's consumption in the presence of food insecurity. We measured food insecurity with quantitative indicators of food production, access, household availability and purchasing power and found no evidence that maternal dietary adequacy of intake was compromised in favor of her child, in neither quantity nor quality as measured by dietary energy and Zinc intake, as indicators of food insecurity varied.
The conceptual framework of food insecurity suggests that adults, and especially mothers, tend to compromise their consumption in favor of that of their young children.3,17,38 With data from poor rural areas in the Mexican central-southern region, our analysis did not support this hypothesis. Through our developed indicators of the availability of and access to food (both physical and economic access), we studied two quantitative dimensions of food insecurity and their association with Zn adequacy intake as an indicator of dietary quality of rural Mexican mothers and that of their preschool children. For both energy and Zinc, larger values of adequacy of dietary intake in children were positively associated with a greater adequacy of maternal dietary intake; and, this association was not modified by the dimensions of food insecurity. Since our hypothesis was that maternal adequacy of intake would be compromised, we would expect that variations in the dimensions of food insecurity could affect or modify the associations between mother-child dietary intakes. This did not occur.
Some evidence from North America report different results from ours when using indicators of perceived food insecurity. In a rural community in New York state, women experiencing food insecurity reported low consumption of potassium, fiber and vitamin C, while the rest of the family maintained optimal consumption.3 More evidence from North America pointed that, more generally women reporting perceived food insecurity, reduced their consumption of energy, magnesium, and vitamins A, E, C and B6; this association, however, was not found in preschool children.16,18 McIntyre followed a group of low-income Canadian women on a weekly basis for one month.22 This period was considered to cover times when a household's economic resources to purchase food would range from high to low. It was found that over the one-month period studied, mothers compromised their consumption in favor of their children, as indicated by the mean adequacy of dietary intake for the mothers being lower than that of their children, particularly energy, vitamin A, folate, Zinc, calcium and iron. In general, adequacy of dietary intake in the mothers was low and was shown to decrease over time. However, this study did not differentiate according to household food insecurity status, although roughly 80% reported experienced it.
The foods that were key indicators of food insecurity were maize and beans, both commonly foods present in household storage and production. This is because both foods constitute the basic diet of the population in rural Mexico. Maize and beans are likely to be produced primarily as a form of subsistence, with the priority of meeting the nutritional needs of the household. Excess production is used to generate income in order to meet other needs.39 We found that the dimensions of food insecurity related to adequacy of energy and Zinc intake in the mother were household production of maize and beans and the percentage of food expenditure, although it only had a slight association with adequacy of energy intake. The fact that energy adequacy is positively associated with this indicator of food security, by no means intends to imply that the more energy mothers –or any family member– consumes, the better. The aim in nutrition policies must be to improve dietary quality while recommending a prudent energy intake; especially in a country as Mexico where two thirds of the adult population is overweight or obese.40
Since consumption is strongly associated with income level and the family's physical access to different products, the availability of foods does not guarantee food security for the household. The Mexican National Committee for the Evaluation of Social Development Policy revealed that in rural areas in Mexico, 31.8% ofindividuals did not have enough income to meet their nutritional needs.41 It is known that poor households spend a large portion of their income on food. This study observed that households in this study typically spent more than half of their expenses on the acquisition of food; higher than the 41% reported for rural Mexico in 2004.42
The strategies used and decisions made withinhouseholds when facing a scarcity of food, are not known with certainty. However there were households with available foods which were not a source of bioavailable micronutrients (i.e., industrialized low-priced food items) which provided poor variety to the diet. On the other hand, our results suggest that when availability of and access to food is scarce, this population turns to household food production: 40% of households consumed household production of maize and/or beans. A study in Sierra de Manantlán,6 a rural Mexican community with little socioeconomic variability, found that 90% of households experienced some degree of food insecurity, this negatively correlated with the availability in the household of fruits, vegetables andfoods from animal origin, including dairy products. It was found that when faced with scarcity or limitations,households depended on foods which they produced themselves.
In contrast to what we expected, the spatial access to local food markets was not associated with the outcome, although the coefficients were always positive. This indicator provides information about location stores (<30 minutes); however it may be not the best to describe the potential access to a variety of food items and their characteristics (number, type, size, price).
The evidence indicates that households experiencing food insecurity typically receive assistance in orderto reduce their vulnerability.7,18,22,43-47 Our study findsthat participation in social programs is negatively associated with adequacy of energy intake in mothers and, although not statistically significant, the coefficient for adequacy of Zinc intake was also negative.This suggests that participation in social programs is an indicator of poverty, and that therefore these households have a greater probability of experiencing foodinsecurity.
The findings of our study are important because particularly they respond to the need to study the gender aspects of food insecurity in rural and marginalized areas in Mexico. Traditionally, the study of the association between food insecurity and diet has been conducted in high-income countries using nationally representative surveys,16,18 in urban zones with scarce resources19,20,22 and in rural communities.3 In Latin America, the understanding of this phenomenon is just beginning;6,7,11,43,48 and this work contributes to that understanding.
A potential limitation of this study may be that dietary information was collected only from mothers and their preschool children, which made it impossible to study the intra-household distribution in-depth. It is known that the nature of a compromised diet varies between populations because it depends on availability, access, and the way in which food is distributed within the family.17,38 Another potential limitation in our study is that dietary information obtained was provided by the mother who may have responded thinking it was a way to evaluate her ability as the caretaker or the one responsible for her family's nutrition; this could result in over-reporting the consumption of the child and underreporting that of the mother. If this were the case, this would indeed obscure the very compromise we are evaluating. However, we have no basis to assume mothers in the more food insecure households of our sample, would underreport their child's diet while over reporting theirs. Regarding external validity of our study, communities' random selection and large sample sizes allow for generalization of the findings to rural communities in southern Mexico, but only to those non-breastfeeding mother-child pairs.
The mother being single, divorced or widowed was negatively associated with the adequacy of her energy and Zinc intake. It may be that not having a partner results in having more limited resources or less financial security with which to face situations within the household, and that this is directly reflected in decreased adequacy of dietary intake. Single and divorced mothers are found to have a more vulnerable health status, and with respect to diet, it has been documented that they consume less fruits and vegetables.49,50
The physiological demand for nutrients in lactating women51 was evident in this study, as lactation was found to be negatively associated with adequacy of Zinc intake. In our study we found that BMI was negatively associated with energy adequacy of intake. We evaluated our estimates including BMI as a covariate. We also stratified by maternal obesity but did not find significant changes in the estimate, its magnitude, direction or p value. The potential error due to underestimation of maternal dietary intake may be debilitating our estimated association, possibly bringing it towards the null value.52
The mothers in indigenous households, independently of other factors, may have better practices withregard to choosing the quantity and quality of food they consume (reflected by the positive and statistically significant association with the coefficients for energy and Zinc, respectively). However, they are only meetingthree quarters of the nutritional requirement (>70%). This data are of concern because women in rural areas have a predominant dietary pattern consisting of maize and its derivatives, wheat and its derivatives, and beans and legumes,53 all of which have low bioavailability for micronutrients. Regardless, the finding that women in indigenous households have higher adequacy of dietary intake suggests that something is occurring for those women. This could be studied in the future so as to clarify the processes that occur within these households.
We analyzed the relationship of a quantitative indicator of food insecurity with the diet of mothers and children in poor southern rural communities in Mexico. We found that in the present of food insecurity, maternal diet is not compromised in favor of that of their children, in terms of either quantity (adequacy of energy intake) or quality (adequacy of Zinc intake). With the assumption that maternal dietary consumption is related to that of the other household members, particularly children, we observed that child adequacy of dietary intake, household production of maize and/or beans, and indigenous household condition, were all associated with a higher maternal adequacy of energy and Zinc intake. The design of this analysis was cross-sectional. In the future, it may be meaningful to explore the relationship between food insecurity and a maternal compromised diet mother in favor her children through time, and not only on a cross sectional study. This could aid in answering the question of whether such a strategy is used by adults in households with food insecurity, and especially by mothers, compromising their own consumption to protect their children.
Acknowledgements
The authors wish to thank the generous and insightful corrections of their anonymous reviewers. With their help, this document was considerably improved.
Declaration of conflict of interests: The autors declare that they have no conflict of interests.
References
1. FAO. Declaration on world food security. Rome:World Food Summit, FAO, 1996. [ Links ]
2. Holben DH. Position of the American Dietetic Association: food insecurity and hunger in the United States. J Am Diet Assoc 2006 Mar;106(3):446-458. [ Links ]
3. Radimer KL, Olson CM, Campbell CC. Development of indicators to assess hunger. J Nutr 1990;120 Suppl 11:1544-1548. [ Links ]
4. Pelletier DL, Olson CM, Frongillo E. Inseguridad alimentaria, hambre y desnutrición. In: Bowman BA, Russel RM, editors. Conocimientos actuales sobre nutrición.Washington, DC: ILSI, OPS, OMS, 2003;762-775. [ Links ]
5. Renzaho AM, Mellor D. Food security measurement in cultural pluralism: missing the point or conceptual misunderstanding? Nutrition 2010;26(1):1-9. [ Links ]
6. Melgar-Quiñonez H, Zubieta AC,Valdez E,Whitelaw BLK. Validación de un instrumento para vigilar la inseguridad alimentaria en la Sierra de Manantlán, Jalisco. Salud Publica Mex 2005;47(6):413-422. [ Links ]
7. Hackett M, Zubieta AC, Hernandez K, Melgar-Quinonez H. Food insecurity and household food supplies in rural Ecuador.Arch Latinoam Nutr 2007;57(1):10-17. [ Links ]
8. The Food and Agriculture Organization of the United Nations. Measurement and assessment of food deprivation and under-nutrition. Proceedings of the International Scientific Symposium. June 26-28, 2002; Rome, Italy. FAO; 2002. [ Links ]
9. Frongillo EA, Jr. Rauschenbach BS, Olson CM, Kendall A, Colmenares AG. Questionnaire-based measures are valid for the identification of rural households with hunger and food insecurity. J Nutr 1997;127(5):699-705. [ Links ]
10. Hamilton WL, Cook JT,Thompson WW, Buron L, Frongillo EA, Olson C, et al. Household food security in the United Sates in 1995.Technical report of the food security measurement project.Alexandria,VA: U.S. Department of Agriculture, Food Consumer Service, 1997. [ Links ]
11. Lorenzana P, Bernal J, Mercado C. Inseguridad Alimentaria y experiencias de hambre en hogares venezolanos menos privilegiados. Rev Esp Nutr Comunitaria 2003;9(3):138-143. [ Links ]
12. Consejo Nacional de Evaluación de la Política de Desarrollo Social. Dimensiones de la seguridad alimentaria: Evaluación Estratégica de Nutrición y Abasto. México; CONEVAL: 2010. [accessed: 2011, 5, 30]. Available in: http://www.coneval.gob.mx/cmsconeval/rw/resource/coneval/home/Evaluacion%20de%20Nutricion%20y%20Abasto%202010.pdf?view=true. [ Links ]
13. Pinstrup-Andersen P. Food Security: Definition and Measurement. Food Security 2009;1:5-7. [ Links ]
14. Champagne CM, Casey PH, Connell CL, Stuff JE, Gossett JM, Harsha DW, et al. Poverty and food intake in rural America: diet quality is lower in food insecure adults in the Mississippi Delta. J Am Diet Assoc 2007;107(11):1886-1894. [ Links ]
15. Glanville NT, McIntyre L. Diet quality of Atlantic families headed by single mothers. Can J Diet Pract Res 2006;67(1):28-35. [ Links ]
16. Cristofar S, Basiotis PP. Dietary intakes and selected characteristics of women ages 19-50 years and their children ages 1-5 years by reported perception of food sufficiency. J Nutr Educ 1992;24(2):53-58. [ Links ]
17. Kendall A, Olson CM, Frongillo EA, Jr. Relationship of hunger and food insecurity to food availability and consumption. J Am Diet Assoc 1996;96(10):1019-24; quiz 25-6. [ Links ]
18. Rose D, Oliveira V. Nutrient intakes of individuals from food-insufficient households in the United States. Am J Public Health 1997;87(12):1956-61. [ Links ]
19. Tarasuk V, McIntyre L, Li J. Low-income women's dietary intakes are sensitive to the depletion of household resources in one month. J Nutr. 2007;137(8):1980-1987. [ Links ]
20. Tarasuk VS, Beaton GH.Women's dietary intakes in the context of household food insecurity. J Nutr 1999;129(3):672-679. [ Links ]
21. Coates J, Frongillo EA, Rogers BL,Webb P,Wilde PE, Houser R. Commonalities in the experience of household food insecurity across cultures: what are measures missing? J Nutr 2006;136:1438S-1448S. [ Links ]
22. McIntyre L, Glanville N, Raine K, Dayle J,Anderson B, Battaglia N. Do low-income lone mothers compromise their nutrition to feed their children? CMAJ 2003;168(6):686-691. [ Links ]
23. Villalpando S, Garcia-Guerra A, Ramirez-Silva CI, Mejia-Rodriguez F, Matute G, Shamah-Levy T, et al. Iron, zinc and iodide status in Mexican children under 12 years and women 12-49 years of age.A probabilistic national survey. Salud Publica Mex 2003;45 Suppl 4:S520-S529. [ Links ]
24. Brown KH, Peerson JM, Rivera J,Allen LH. Effect of supplemental zinc on the growth and serum zinc concentrations of prepubertal children: a meta-analysis of randomized controlled trials.Am J Clin Nutr 2002;75(6):1062-1071. [ Links ]
25. Bhutta ZA,Ahmed T, Black RE, Cousens S, Dewey K, Giugliani E, et al. What works? Interventions for maternal and child undernutrition and survival. Lancet. 2008 Feb 2;371(9610):417-440. [ Links ]
26. Leroy JL, Rodríguez S, Marini A, González de Cossío T. Impacto de la política social en el estado de nutrición, dieta y gasto en alimentos. In: González de Cossío T, Rivera Dommarco J, López Acevedo G, Rubio Soto GM, eds. Nutrición y pobreza Política basada en evidencia. México: Banco Mundial y Secretaria de Desarrrollo Social 2008:133-148. [ Links ]
27. Leroy JL, Gadsden P, Rodriguez-Ramirez S, de Cossio TG. Cash and in-kind transfers in poor rural communities in Mexico increase household fruit, vegetable, and micronutrient consumption but also lead to excess energy consumption. J Nutr 2010;140(3):612-617. [ Links ]
28. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K,Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon,Vanadium, and Zinc.Washington, DC: Institute of Medicine, National Academy of Sciences, 2001. [ Links ]
29. Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington, DC: Institute of Medicine, National Academy of Sciences, 2002. [ Links ]
30. Safdie M, Barquera S, Porcayo M, Rodríguez S, Ramírez C, Rivera J, et al. Bases de datos del valor nutritivo de los alimentos. Cuernavaca, México: Instituto Nacional de Salud Pública, 2002. [ Links ]
31. Brown T. Confirmatory factor analysis for applied research. New York: The Guilford Press, 2006. [ Links ]
32. Gorsuch R. Factor analysis. Second edition. New Jersey: Lawrence Erlbaum Associates, Inc 1983. [ Links ]
33. Kachigan S. Factor Analysis. In: Kachigan S, ed. Multivariate statistical analysis A conceptual introduction Second edition. New York: Radius Press, 1991:236-260. [ Links ]
34. Long-Solís J,Vargas LA. Food Culture in Mexico. Greenwood Press, 2005. [ Links ]
35. WHO, Multicentre, Growth, Reference, Study, Group.WHO Child Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva:World Health Organization, 2006. [ Links ]
36. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000;320(7244):1240-1243. [ Links ]
37. World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee.Technical Report Series No. 854. Geneva, 1995. [ Links ]
38. Nord M,Andrews M, Carlson S. Household Food Security in the United States, 2005. United States Department of Agriculture, Economic Research Service, 2006. [ Links ]
39. León A, Guzmán E. Papel de la alimentación en la reproducción y el desarrollo del campesinado. In: Espinosa L, ed. Sector agropecuario y alternativas comunitarias de seguridad alimentaria y nutrición en México. México: UAM, CECIPROC, INNSZ, Plaza y Valdés, 1999:267-286. [ Links ]
40. Barquera S, Campos-Nonato I, Hernandez-Barrera L, Flores M, Durazo-Arvizu R, Kanter R, et al. Obesity and central adiposity in Mexican adults: results from the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex 2009;51 Suppl 4:S595-S603. [ Links ]
41. Consejo Nacional de Evaluación de la Política de Desarrollo Social. Reporta Coneval cifras actualizadas de pobreza por ingresos 2008. Comunicado de prensa. Mexico city: Coneval, 2009:18. [ Links ]
42. Servicio de Información y Estadística Agroalimentaria y Pesquera (SIAP) Secretaría de Agricultura, Ganadería, Desarrollo Rural, Pesca y Alimentación. Comportamiento del gasto de los hogares en alimentos en el sector rural 2000-2004. Mexico city: Sagarpa, 2006. [ Links ]
43. Bernal J, Lorenzana P. Predictores de la seguridad alimentaria en hogares de escasos recursos en Venezuela: comparación entre región central y andina. Interciencia 2003;28(1):15-20. [ Links ]
44. Jones SJ, Frongillo EA.The modifying effects of Food Stamp Program participation on the relation between food insecurity and weight change in women. J Nutr 2006;136(4):1091-1094. [ Links ]
45. Kaiser LL, Melgar-Quinonez H,Townsend MS, Nicholson Y, Fujii ML, Martin AC, et al. Food insecurity and food supplies in Latino households with young children. J Nutr Educ Behav 2003;35(3):148-153. [ Links ]
46. Olson CM. Nutrition and health outcomes associated with food insecurity and hunger. J Nutr 1999;129(2S Suppl):521S-524S. [ Links ]
47. Wilde PE. Measuring the effect of food stamps on food insecurity and hunger: research and policy considerations. J Nutr 2007;137(2):307-310. [ Links ]
48. Lorenzana P, Danjur D. La adaptación y validación de una escala de seguridad alimentaria en una comunidad de Caracas,Venezuela.Arch Latinoamer Nutr 2000;50(4):334-340. [ Links ]
49. Elfhag K, Rasmussen F. Food consumption, eating behaviour and self-esteem among single v. married and cohabiting mothers and their 12-yearold children. Public Health Nutr 2008;11(9):934-939. [ Links ]
50. Macintyre S.The effects of family position and status on health. Soc Sci Med 1992;35(4):453-464. [ Links ]
51. Food and Nutrition Board. Nutrition During Lactation.Washington, DC: Institute of Medicine, National Academy of Sciences 1991. [ Links ]
52. Campirano F, Barquera S, Hass JD,Téllez-Rojo M, Rivera-Dommarco J. Estimación del sub-reporte de energía en mujeres mexicanas obesas y no obesas: análisis de la Segunda Encuesta Nacional de Nutrición. In: Barquera S, ed.Aspectos de Nutrición y Alimentación en México. Cuernavaca, México: Instituto Nacional de Salud Pública 2003:24-33. [ Links ]
53. Flores M, Rodríguez S, Barquera S,Villalpando S, Rivera J. Dietary patterns, non-communicable chronic diseases, and C-reactive protein in Mexican women. Experimental Biology 2005;Abstract 839.1. [ Links ]
 Correspondence author:
Correspondence author:
Teresita González de Cossío
Instituto Nacional de Salud Pública
Av. Universidad 655
Col. Santa María Ahuacatitlán
62100 Cuernavaca, Morelos, México
E-mail: tgonzale@insp.mx
Received on: February 2011
Accepted on: July 2011
* González D, Santos R, Gutiérrez JP, González-Cossío T. Índice de Disponibilidad de Alimentos en la Localidad. In press 2004.
** StataCorp. 2007. Stata Statistical Software: Release 10. CollegeStation, TX: StataCorp LP.


{kind=link}
{kind=link}
{kind=link}
{kind=link}