










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkSalud Pública de México
versão impressa ISSN 0036-3634
Salud pública Méx vol.53 no.3 Cuernavaca Mai./Jun. 2011
ARTÍCULO ORIGINAL
Streptococcus pneumoniae serotypes isolated from the middle ear of Mexican children diagnosed with acute otitis media
Serotipificación de Streptococcus pneumoniae aislados de líquido de oído medio en niños mexicanos con diagnóstico de otitis media aguda.
Demóstenes Gómez-Barreto, MDI; Luz Elena Espinosa de los Monteros, PhDII; Claudia López-Enríquez, MDIII; Romeo Rodríguez Suarez, MDIV; Carlos de la Torre, MDI
IHospital Infantil de México Federico Gómez, México, DF. México
IIHospital General Dr. Manuel Gea González, México, DF. México
IIIHospital Español, Unidad de Enfermedades Infecciosas, México, DF. México
IVInstitutos Nacionales de Salud, México, DF. México
ABSTRACT
OBJECTIVE: The aim of this study was to identify the etiology and the serotypes of S. pneumoniae (Sp) in Mexican children with acute otitis media (AOM).
MATERIALS AND METHODS: The study includessamples frompatientsdiagnosed with AOM at the Federico Gomez Children's Hospital of Mexico (2002-2003),with positive culture for Sp bacteriologically confirmed in middle ear fluid obtained by tympanocentesis. All Sp were serotyped. A total of 138 samples from 135 children with AOM were included.
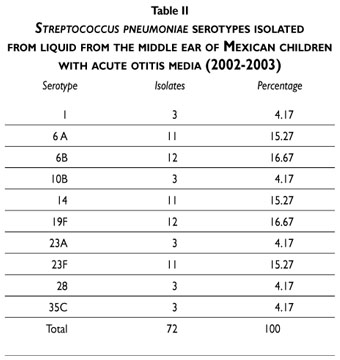
RESULTS: Sp was isolated in 72 samples from 70 children. Sixty (85.7%) were previously healthy and 10 (14.3%) were immunocompromised. The most common serotypes were 6B and 19F (16.67%), and 6 A, 14 and 23F (15.27%).
CONCLUSION: The distribution of serotypes among the children with AOM in the study is similar to that reported in developing cities, and 63.9% of the isolated serotypes are found to be included in the 7-Valent Pneumococcal Conjugate Vaccine (PCV), 68.1% in the 10-Valent PCV and 83.3% in 13-Valent PCV.
Key words: otitis media, Streptococcus pneumoniae, serotyping; Mexico
RESUMEN
OBJETIVO: Conocer la etiología y serotipos de S. pneumoniae (Sp) en niños mexicanos, con otitis media aguda (OMA).
MATERIAL Y MÉTODOS: Se incluyeron las muestras de pacientes con OMA del Hospital Infantil de México Federico Gómez (2002-2003), con cultivo positivo para Sp, (bacteriológicamente confirmados en el líquido del oído medio obtenido por timpanocentesis). Todos los Sp. fueron serotipificados. Se incluyeron 138 muestras de 135 niños con OMA.
RESULTADOS: Sp. se aisló en 72 muestras de 70 niños: 60 (85.7%) eran previamente sanos y 10 (14.3%) eran inmunocomprometidos. Los serotipos más frecuentes fueron 6B y 19F (16.67%), y 6 A, 14 y 23F (15.27%).
CONCLUSIONES: La distribución de los serotipos en niños con otitis media aguda fue similar a la reportada en ciudades en desarrollo y se observó que 63.9% de los serotipos aislados están incluidos en la vacuna conjugada 7-valente, 68.1% en la 10-valente y 83.3% en la 13-valente.
Palabras clave: otitis media, Streptococcus pneumoniae, serotipificación; México
Acute otitis media (AOM) is one of the most common infections in the world, and mainly affects children. The epidemiology of acute otitis media over the last decade has indicated a change in the course of the disease, with more children experiencing recurring episodes during their first year. Since this is one of the diseases for which antibiotics are most indicated, it has brought about changes in the susceptibility to antibiotics of the pathogenic bacteria involved, as well as changes in treatment strategies.1
The 7-valent pneumococcal conjugate vaccine (7-valent PCV) has shown its efficacy in preventing the specific Streptococcus pneumoniae serotypes that cause otitis, and reducing the resistance of respiratory pathogenic bacteria to antibiotics.2,3 Before the 7-valent PCV was given universally in the United States, around 7 000 000 cases of AOM caused by S. pneumoniae had been estimated.4
Due to its importance and epidemiological frequency, AOM is one of the infectious processes for which antimicrobials are most frequently prescribed, and sometimes incorrectly. This is considered to be the cause of increased anti-microbial resistance in many parts of the world.5 The pathogens that are the most common cause of AOM are Streptococcus pneumoniae (25-50%), Haemophilus influenzae (15-30%) and Moraxella catarrhalis (3-20%). Nevertheless, it was not possible to isolate any bacterial pathogen in 16% of cases or viral pathogen in 25% of cases.6,7
The leading bacterial causes of AOM in Mexico and worldwide are Streptococcus pneumoniae and Haemophilus influenza nontypable.8,9 Treating AOM caused by Streptococcus pneumoniae in children under the age of two has become complicated in Mexico and around the world due to decreased susceptibility to antibiotics and the increase in more virulent serotypes, such as those included in the 7-valent PCV.10 The availability of local epidemiological information about the S. pneumoniae serotypes that cause AOM is therefore needed.
This epidemiological approach is of great interest as there is evidence that preventive measures can be taken once the S. pneumoniae serotypes involved in AOM are known, particularly those contained in the vaccine.3,10 Therefore, the aim of this study was to identify the etiology and serotypes of Streptococcus pneumoniae that cause AOM in a selected group of Mexican children.
Material and Methods
This study was an open, observational, retrospective, cross-sectional study. Samples were included of patients diagnosed with AOM at the Federico Gomez Children's Hospital of Mexico between March 2002 and March 2003. The clinical characteristic of the patients selected was bacteriological confirmation using tympanocentesis to remove fluid from the middle ear in order to confirm the bacteriological diagnosis.
The patients were clinically evaluated by an otorhinolaryngology specialist and classified by the head of otorhinolaryngology. The tympanocentesis was performed with patients who needed a bacteriological diagnosis in order to identify the bacterial etiology and determine a specific treatment.
The procedure was performed by an otolaryngologist using microscopic vision. After the external auditory canal was cleaned, samples were taken using a centuria device. Informed consent from one of the parents of each patient was obtained before performing tympanocentesis. Patients excluded were those with a ruptured eardrum within 48 hours of performing tympanocentesis and those who had ventilation tubes and craniofacial deformations.
Samples taken from the middle ear were cultured in sheep blood agar at 5% and chocolate agar incubated at 37ºC for 24 hours in a CO2 atmosphere at 10%. Isolation of S.pneumoniae was identified based on colonial morphology microscopy, susceptibility to optoquine and solubility in bile.11 Serotyping was performed usingthe Quellung reaction with specific pneumococcal antiserums from the Statens Serum Institute (Copenhagen, Denmark). All isolations were typed according to group and factor based on Danish nomenclature.12
Results
Included were 138 samples from 135 patients diagnosed with AOM, and 135 bacterial isolations: 72 S. pneumoniae (52.2%), 44 H. influenzae nontypable (31.9%), 13 Moraxella catarrhalis (9.4%), two Staphylococcus aureus (1.4%), two Pseudomonas aeruginosa (1.4%), one E. coli (0.7%), one Streptococcus pyogenes (0.7%) and three samples without germs (2.2%).
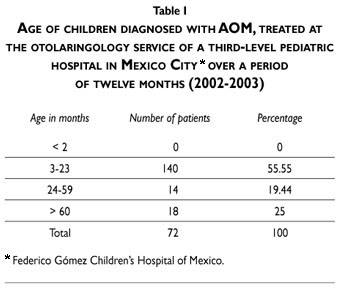
Of the 70 patients in which S. pneumoniae was isolated, 60 (85.7%) were previously healthy and 10 (14.3%) suffered from an underlying disease that made them immunocompromised. The average age of patients who had S. pneumonie isolated in their ear was 42.5 months with median of 22 months (range 5-109 months). Fifty five percent of patients were under 24 months (Table I). Two were diagnosed with human immunodeficiency virus (HIV) and 8 were diagnosed with acute lymphoblastic leukemia and treated with chemotherapy. The two patients with HIV presented recurrent otitis media on two occasions.
In terms of severity of the infection, of the total 72 cases of otitis, 64 (88.9%) episodes were classified as AOM, four (5.5%) as acute bilateral otitis, and four (5.5%) as recurrent otitis. The latter correspond to two samples from each of the two patients who presented two different episodes.
The serotypes identified in the S. pneumoniae isolates are shown in Table II. Four of those (6B, 14, 19Fand 23 F), which were found in 46 cases (63.9%) are contained in the 7-valent PCV, five (1, 6B, 14, 19F and 23 F), in 49 cases (68.1%), are in the 10-valent PCV and six (1, 6A, 6B, 14, 19F and 23F), in 60 cases (83.3%), are in the 13-valent PCV.
Discussion
AOM is one of the most common infections in the world, particularly among children under the age of 2 years. The bacterial pathogens in AOM that are most frequently isolated are S. pneumoniae, H. influenza nontypable,and M. catarrhalis, with S pneumoniae being that which is the leading cause of AOM and for which there is the least possibility of a spontaneous cure.13-14
S. pneumoniae is considered to be the more likely cause of complications such as spontaneous rupture of the eardrum and may even cause loss of hearing.15 In some developing countries, AOM and its complications may cause up to 50 000 deaths a year.16 Epidemiological surveillance studies show5,6,7 that before the 7-valent PCV vaccine was introduced, S. pneumoniae was the most common pathogen isolated from fluid in the middle ear of children with AOM (47.7-53% ).17
The most frequent S. pnenumoniae serotypes in our study are: 6B, 19 F, 14, 23F and 6A. It is well known the serotypes that cause AOM worldwide vary according to a number of factors, such as age, health and geographical location.18-22
A review of the most prevalent serotypes involved in AOM in various geographical areas, including the United States ofAmerica, indicate that the most frequent ones are 6 A, 6 B, 14, 19 A, 19 F and 23 F.18-22 Of these six serotypes, four (6 B, 19 F, 14 and 23 F) coincide with the data obtained from our study. When comparing these with AOM-related serotypes in other countries, such as Costa Rica23 and Argentina, there are major differences, particularly in Costa Rica where serotypes 3 and 19F are significant. In Argentina, serotype 14 represents 53.5% of total AOM cases, in contrast to 15.2% in this study.18 In addition, in Europe,24-26 the most common serotypes are 1, 3, 6, 9V, 14, and 23F, whereas in our study we found only three of these (6,14 and 23). These examples clearly show geographical differences in the prevalence of serotypes that cause AOM. Therefore, each country or geographic region needs to conduct active epidemiological surveillance of the S. pneumoniae serotypes that cause AOM.
One point of particular importance is that major changes have occurred in the pathogens that cause AOM, after the 7-valent PCV vaccine was introduced, such as a reduction in S. penumoniae and an increase in nontypable H. influenzae.27-30 Other studies have shown a decrease in the percentage of vaccine serotypes and an increase in non-vaccine serotypes (1,3, 6A, 7, 10, 11 A, 15A, 16, 19A, 20 22, 29, 31, 33 F, 35, 37, 38, 42 and nontypable serotypes).30-32 In patients vaccinated with two to four 7-valent PCV doses, the most commonly isolated serotypes causing AOM were 3, 18A and 19A.32
Serotype 19A has increased substantially as a carrier in invasive infections and in AOM. Korea, Israel and Mexico have found 19A serotypes as carriers and in invasive forms.33-35
The most common AOM Sp serotypes worldwide are 6A, 6B, 14, 19A, 19F and 23F, while serotype 3 is rare.36 A Finnish study provides evidence of AOM prevention using 7-valent PCV.3
In addition to the 7-valent PCV vaccine's protective factors, it provides a number of other benefits, including: reducing the number of consultations related to AOM, reducing the need to use ventilation tubes for recurrent otitis, lowering the resistance of bacteria to penicillin and other antibiotics and strengthening the herd effect –an indirect effect that has the greatest epidemiological impact.2,28,29,37
In a recent study in children associated with an insurance company and who received four doses of 7-valent PCV vaccine, consultations related to AOM decreased 42.7% and there was a reduction in antibiotic use.29
We found in our results that of all the S. pneumoniae serotypes isolated in the fluid of the middle ear, 63.9% were contained in the 7-valent PCV, 68.1% in the 10-valent PCV and 83.3% in the 13-valent PCV.
Our results could not be generalized to the entire Mexican population because in the study we only include a small group of children in a special population (Mexican children at a third level hospital, Children's Hospital of Mexico), from 2002 to 2003, before the universal 7-valent PCV was used in Mexico. Currently, there may now be new and different pneumococcal serotypes, therefore it is important to continue to conduct epidemiological studies.
These results highlight the need to use S. pneumoniaeconjugate vaccines universally, however, the regional epidemiology of predominant serotypes in AOM needs to be ascertained to develop recommendations suitable to each region. The importance of implementing epidemiological surveillance procedures should also be emphasized, so as to assess the impact and benefits of anti-pneumococcal vaccination.
Conclusions
Identifying the local epidemiology of Streptococcus pneumonaie serotypes associated with AOM is very important to developing the best prevention and treatment practices for pneumococcal otitis.
The only preventive action that may currently be taken against AOM caused by S. pneumoniae is the administration of S. pneumoniae conjugate vaccines.
Our results show that in a small group of Mexican children with AOM, 63.9% of S. pneumoniae serotypes identified as causing the disease are included in the 7-valent PCV vaccine.
Declaration of conflicts of interest: The authors declare that they have no conflict of interests.
References
1. Jacobs MR. Increasing antibiotic among otitis media pathogens and their susceptibility to oral agents base on pharmacodynamic parameters. Pediatr Infect Dis J 2000; 19: S47-56. [ Links ]
2. Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, et al. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Northern California Kaiser Permanente Vaccine Study Center Group. Pediatr Infect Dis J 2000;19(3):187-95. [ Links ]
3. Eskola J, Kilpi T, Palmut A, Jokinen J, Haapakoski J, Herva E, et al. Efficacy of pneumococcal conjugate vaccine against acute otitis media. N Engl J Med 2001; 344: 403-9. [ Links ]
4. Centers for Disease Control and Prevention. Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1997;46:1-24. [ Links ]
5. McCraken GH Jr.Treatment of acute otitis media in an era of increasing microbial resistance. Pediatr Infect Dis J 1998; 17:576-9. [ Links ]
6. Klein JO. Microbiologic efficacy of antibacterial drugs for acute otitis media. Pediatr Infect Dis J 1993;12: 973-5. [ Links ]
7. Teele DW, Klein JO, Word BM, Rosner BA, Starobin S, Earle R Jr, Ertel CS, Fisch G, Michaels R, Heppen R, Strause NP; Greater Boston Otitis Media Study Group. Antimicrobial prophylaxis for infants at risk for recurrent acute otitis media. Vaccine 2000; 19 Suppl 1:S140-3. [ Links ]
8. Rodríguez RS, Sánchez C, de la Torre GC. Bacteriology and the response to treatment using erythromycin – sulphametoxazol in children with acute otitis media. Bol Med Hosp Infant Mex 1987; 44: 728. [ Links ]
9. Owen J. Otitis media . N Engl J Med 2002; 347: 1169-74. [ Links ]
10. Hausdorff WP, Bryant J, Kloek C, Paradiso PR, Siber GR. The contribution of specific pneumococcal serogroups to different disease manifestations: implications for conjugate vaccine formulation and use: part II. Clin Infect Dis 2000; 30: 122-40. [ Links ]
11. Facklam, RR and Washington JA II. Streptococcus and related catalasenegative gram-positive cocci. In: Ballows A, Hauher WJ, Hermann KL, Isenberg HD, and Shadomy HJ (ed). Manual of clinical microbiology. 5th ed. Washington, DC: American Society for Microbiology, 1991: 238-257 [ Links ]
12. Sørensen UB.Typing of pneumococci by using 12 pooled antisera. J Clin Microbiol 1993; 31(8):2097-100. [ Links ]
13. Teele DW, Klein JO, Chase C, Menyuk, Rosner BA. Otitis media in infancy and intellectual ability, school achievement, speech, and language at age 7 years. Greater Boston Otitis Media Study Group. J Infect Dis 1990; 162(3): 685-94. [ Links ]
14. Erhardt W, Murphy M, Knirsch C. Establishing criteria for assessment of efficacy of antimicrobial agents in acute otitis media.Antimicrob Agents Chemother 2000 ;44(9):2590-2. [ Links ]
15. Leibovitz E, Serebro M, Givon-Lavi N, Greenberg D, Broides A, Leiberman A et al. Epidemiologic and microbiologic characteristics of culture-positive spontaneous otorrhea in children with acute otitis media. Pediatr Infect Dis J 2009;28(5):381-4 [ Links ]
16. Berman S. Otitis media in developing countries. Pediatrics 1995;96:126-31. [ Links ]
17. Block SL, Hendrick J, Harrison CJ,Tyler R, Smith A, Findlay R, Keegan E. Pneumococcal serotypes from acute otitis media in rural Kentucky. Pediatr Infect Dis J 2002; 9:859-965. [ Links ]
18. Hausdorff WP,Yorhers G, Dagan R, Kilpi T, Pelton SI, Cohen R, et al. Multinational Study of pneumococcal serotypes causing acute otitis media in children. Pediatr Infect Dis J 2002; 21: 1008-16. [ Links ]
19. Hausdorff WP, Bryant J, Kloek C, Paradiso PR, Siber GR. The contribution of specific pneumococcal serogroups to different disease manifestations: implications for conjugate vaccine formulation and use, part II. Clin Infect Dis 2000; 30: 122-40. [ Links ]
20. Dagan R, Givon, Lavi N, Shkolnik L,Yagupsky P, Fraser D. Acute otitis media caused by antibiotic-resistant Streptococcus pneumoniae in southern Israel: implication for immunizing with conjugate vaccines. J Infect Dis 2000;18: 1322-29. [ Links ]
21. Guevara S, Soley C,Arguedas A, Porat N, Dagan R. Seasonal distribution of otitis media pathogens among Costa Rican children. Pediatr Infect Dis J 2008; 27(1):12-6 [ Links ]
22. Rodgers GL,Arguedas A, Cohen R, Dagan R. Global serotype distribution among Steptococcus pneumoniae isolates causing otitis media in children: potential implications for pneumococcal conjugate vaccines. Vaccine 2009; 27: 3802-10. [ Links ]
23.Arguedas A, Dagan R, Guevara S, Porat N., Soley C, Pérez A, Brilla R. Middle era fluid Streptococcus pneumoniae serotype distribution in Costa Rican children with otitis media. Pediatr Infec Dis J 2005; 24: 631-34. [ Links ]
24. Prymula P, Peeters P, Chrobok V, Kriz P, Novakova E, Kohl I, et al. Pneumococcal capsular polysaccharides conjugated to protein D for prevention of acute otitis media caused by both Streptococcus pneumoniae and non- typable Haemophilus influenzae: a randomized double -blind efficacy study. Lancet 2006; 367: 270-78. [ Links ]
25. Kilpi T , Herva E, Kaijalainen T, Syrjânen R, Takala AK. Bacteriology of acute otitis media in a cohort of Finnish children followed for the first two years of life. Pediatr Infec Dis J 2001; 20: 654-62. [ Links ]
26. Gene A, Garcia-Garcia JJ, Domingo A, Wiemberg P, Palavacino E. Etiology of acute otitis media in children in hospital and sensitivity of the evolved microorganisms to antibiotics: Enferm Infect Microbiol Clin 2004; 22: 377-30. [ Links ]
27. Block SL, Hedrick J, Harrison CJ, Tyler R, Smith A, Findlay R, et al. Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. Pediatr Infect Dis J 2004;9:829-33. [ Links ]
28. Casey JR, Pichichero ME. Changes in frequency and pathogens causing acute otitis media in 1995 -2003. Pediatr Infect Dis J 2004;23:824-28. [ Links ]
29. Zhou F, Shefer A, Kong Y, Nuorti JP.Trends in acute otitis media – related health care utilization by privately insured young children in the United States, 1997-2004. Pediatrics 2008; 121: 253-60. [ Links ]
30. Pichichero ME, Casey JR. Emergence of multiresitant serotype 19A pneumococcal strain not included in the 7-valent conjugate vaccine as an otopathogen in children. JAMA 2007; 298:1772-1778. [ Links ]
31. Pai R, Moore MR, Pilishvili T, Gertz RE, Whitney CG, Beall B,. Active Bacterial Core Surveillance Team. Post vaccine genetic structure of Streptococcus pneumoniae serotype 19 A from children in the United States, J Infect Dis 2005. 192: 1988-95. [ Links ]
32. McEllistrem MC, Adams JM, Patel K, Mendelsohn AB, Kaplan SL, Bradley JS et al. Acute otitis media due to penicillin –nonsusceptible Streptococcus pneumoniae before and after the introduction of the pneumococcal conjugate vaccine. Clin Infec Dis 2005; 40: 1738-44. [ Links ]
33. Choi EH, Kim SH, Eun BW, Kim SJ, Kim NH, Lee J, et al. Streptococcus pneumoniae serotype 19A in children, South Korea. Emerg Infect Dis 2008;14(2):275-81. [ Links ]
34. Espinosa-de Los Monteros LE, Jiménez-Rojas V, Aguilar-Ituarte F, Cashat-Cruz M, Reyes-López A, Rodríguez-Suárez R, Kuri-Morales P, Tapia-Conyer R, Gómez-Barreto D. Streptococcus pneumoniae isolates in healthy children attending day-care centers in 12 states in Mexico. Salud Publica Mex 2007; 49(4): 249-55. [ Links ]
35. Gomez-Barreto D, Espinosa de los Monteros LE, Lopez-Enriquez C, Jimenez Rojas V, Rodriguez Suarez R. Invasive Pneumococcal Disease in a Third Level Pediatric Hospital in Mexico City: Epidemiological Characteristics and Mortality-Related Risk Factors. Salud Publica Mex 2010; 52 (5): 391-97. [ Links ]
36. Porat N, Soley C, Marengoleine MM, Grenber D, Givon-Levin, Trefler R, et al.An international serotype 3 clones causing pediatric and invasive infections in Israel, Costa Rica and Lithuania. Pediatr Infec Dis J 2008; 27: 709-12 [ Links ]
37. Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lynfield R et al.Active Bacterial Core Surveillance of the Emerging Infections Program Network. Decline in invasive pneumococcal disease after the introduction of protein polysaccharide conjugate vaccine. N Engl J Med 2003; 348: 1733-45. [ Links ]
 Solicitud de sobretiros:
Solicitud de sobretiros:
Dr. Demóstenes Gómez Barreto
Hospital Infantil de Mexico Federico Gómez
Calle Dr. Marquez 162, Col. Doctores, Mexico, DF
E-mail: dgbarreto30@hotmail.com
Received on: October 15, 2010
Accepted on: April 14, 2011

