










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.51 supl.2 Cuernavaca ene. 2009
ENSAYO
Breast cancer: why link early detection to reproductive health interventions in developing countries?
Cáncer de mama: ¿por qué integrar la detección temprana con las intervenciones en salud reproductiva en países en vías de desarrollo?
Felicia Knaul, PhDI; Flavia Bustreo, MDII; Eugene Ha, MAIII; Ana Langer, MDIV
ICancer de mama: Tómatelo a Pecho y Observatorio de la Salud. Instituto Carso de la Salud y Fundación Mexicana para la Salud. México DF, México
IIPartnership for Maternal Newborn and Child Health (PMNCH), The Secretariat hosted by WHO, Geneva, Switzerland
IIIObservatorio de la Salud. Fundación Mexicana para la Salud. Mexico DF, Mexico
IVEngenderhealth; New York, NY, USA
ABSTRACT
Breast cancer has not been sufficiently integrated into broader efforts either on maternal and child, or reproductive health and this presents an opportunity to strengthen early detection. The analysis is based on global breast cancer statistics and a bibliographic review of key global programs and strategies to promote women´s health in the developing world. Breast cancer is a leading cause of cancer deaths in all regions of the developing world and is striking many women during the reproductive phase. There is an opportunity to increase awareness among women and undertake clinical examination to detect breast cancer by linking to existing health interventions related to reproductive and maternal and child health in developing countries. These synergies should be tested and evaluated in developing countries to identify the potential impact on early detection and on reducing the proportion of cases that are found in more advanced stages.
Key words: breast cancer; reproductive health; reproductive cancers; maternal and child health
RESUMEN
Los esfuerzos para integrar el tema de cáncer de mama a los programas dedicados a la salud materna e infantil y a la salud reproductiva han sido insuficientes. Esto representa una oportunidad para fortalecer la detección temprana del cáncer de mama. El análisis se basa en las estadísticas disponibles mundialmente y una revisión bibliográfica sobre los programas claves para promover la salud de la mujer en países en vías de desarrollo. El cáncer de mama es una de las principales causas de muerte por tumores cancerígenos en todas las regiones del mundo en vías de desarrollo y ataca a muchas mujeres durante su etapa reproductiva. Vincular las intervenciones relacionadas con la salud materno-infantil y reproductiva con el cáncer de mama constituye una oportunidad para concientizar a las mujeres y llevar a cabo examen clínico de mama. La posibilidad de aprovechar estas sinergias para impulsar la detección y así reducir la proporción de casos identificados en fases tardías, debe ser probada y evaluada en países en desarrollo.
Palabras clave: cáncer de mama; salud reproductiva; cánceres de la reproducción; salud materna-infantil
Women, and particularly poor women, in the developing world face a double burden in health that parallels the epidemiological transition.1 There is an ongoing battle with problems associated with underdevelopment and lack of access to basic health services which are primarily related to reproduction, nutrition and communicable diseases. At the same time, women, as well as their countries and health systems, are facing new and emerging challenges associated with chronic illness and non-communicable diseases.
Breast cancer is an emerging challenge on the horizon and is fast becoming a new frontier for women's health in the developing world. While the health problems of underdevelopment are clearly concentrated among the poor, breast cancer is affecting adult women of all economic levels and in both pre- and post-menopausal stages of life.
Thus, poor women face a double burden -they are still exposed to, and dying from, the diseases and health problems of underdevelopment, and at the same time are increasingly facing high rates of chronic illnesses associated with changing lifestyles and disease patterns. The health burden of poor women is painfully illustrated by the concentration of persistent maternal mortality,2 high HIV/AIDS prevalence rates,3 and cervical and breast cancer4,5 among women of reproductive age.
The magnitude of the threat to women's health in developing countries from breast cancer is largely unknown. Breast cancer is often mistakenly deemed a disease of high-income countries and wealthy women. Recent evidence shows that breast cancer is on the rise as a cause of mortality among both pre- and post-menopausal women and already represents a major threat to women's health. Due to misconceptions and lack of knowledge, breast cancer has not been sufficiently integrated into broader efforts either on maternal and child health, or on reproductive health. This provides an important opportunity to strengthen efforts to promote early detection and treatment of breast cancer that have been largely ignored to date. The purpose of this article is to bring attention to these opportunities to impact on the health of women by reducing the number of breast cancer deaths and extending life-expectancy after diagnosis.
This research is based on a bibliographic review of evidence on key global programs and strategies to promote women's health in the developing world. We reviewed the most recent available data on incidence and mortality from breast cancer worldwide, and what is known of risk factors and preventive strategies. We further explored the extent to which existing global efforts to improve women's health are integrating early detection and treatment of breast cancer.
It is important to note that global statistics from developing countries, particularly on incidence, are deficient. We make use of the best available data, but note the limitations of this information and the importance of establishing and promoting cancer registries in developing countries.
Health and health care for women are extremely inequitably distributed both between and within countries. Further, excess morbidity and mortality among women in developing countries is the manifestation of a significant social injustice in a globalized world where poor women are marginalized and continue to be denied the health care they need.
Maternal mortality clearly falls into the realm of a health problem associated with poverty and underdevelopment. Twenty years after the launch of the Safe Motherhood Initiative more than 500000 women still lose their life every year in childbirth.6 Maternal deaths are not uniformly distributed across the world and are strongly associated with underdevelopment. The highest obstetric risk is observed in Sub-Saharan Africa, the poorest region of the world. On average globally, the risk of a woman dying as a result of pregnancy or childbirth during her lifetime is about one in six in the poorest countries compared with one in 30000 in Northern Europe.7 Cross-country comparisons are equally startling: in 2005, the maternal mortality ratio was estimated at 2100 per 100000 live births in Sierra Leone and only 3 per 100000 live births in Sweden.6 Most importantly, the vast majority of maternal deaths in the developing world occurs among the poorest women, and could be prevented with access to the basic elements of safe motherhood, such as access to family planning, skilled attendance at birth and emergency obstetric care in case of complications.8
Reproductive cancers and reproductive health
Cervical cancer provides an important contrast to breast cancer and lies somewhere in the middle of the spectrum of the women's health and epidemiological transitions. It may increasingly be considered a disease associated with poverty and lack of access to preventive services. It is a cancer, and thus falls into the realm of chronic illness, but it is now known to be associated with transmission of a virus, can be detected and treated with low-cost procedures in pre-cancerous stages, and is preventable with a vaccine.9 Increasingly, cervical cancer is being seen as a disease of underdevelopment and associated with poverty and lack of access to appropriate reproductive health services.
By contrast, early detection of breast cancer is costly and in the best case scenario is detected while still localized in the breast.10 The causes of the worldwide increase are largely unknown and many are likely associated with genetic factors and pre-disposition which are costly and difficult to identify.4,11 At this point in time, primary prevention (in the sense of removing a risk factor and thus preventing the onset of the disease) of breast cancer is not possible and early detection requires advanced medical technology such as mammography.10 Treatment is also costly, particularly when the disease is detected in advanced stages - as occurs in the majority of cases identified in developing countries according to available evidence.5
Many of the factors that have been identified as reducing the risk of breast cancer are associated with reproductive and maternal and child health. Most importantly, existing literature suggests that breast-feeding protects women from breast cancer. For example, a comprehensive study published by the American Institute for Cancer Research12 found that the most convincing preventive and protective measure against breast cancer is breast-feeding. Research from Mexico is consistent with this finding.13
Recent research reviews, including the World Cancer Report,14 suggest that after the genetic correlation with the breast cancer, reproductive health-related risk factors -early age at menarche, late age at menopause, and first, full-term pregnancy after age 30, as well as hormone replacement therapy (HRT)- are important factors associated with an increased risk of breast cancer.15-21
Finally, diet and nutrition during a woman's life affect physical conditions and hormonal levels, and influence the process of breast development, as well as the timing of puberty and menopause.12 The extensive study by the American Institute for Cancer Research, Food, Nutrition, Physical Activity, and the Prevention of Cancer12 states that adult weight gain is probably a risk factor for postmenopausal breast cancer. A study on height and weight change in Brazil concluded that "obesity at the time of diagnosis and weight gain since youth increase the risk of breast cancer among postmenopausal women." 22
The burden of breast cancer in developing countries
Recent evidence shows that in middle-income developing countries, breast cancer is replacing cervical cancer as the number one cause of death among women from malignant tumors.5 Almost half of the breast cancer cases that are detected annually are found in low- and middle-income countries.4 Further, given the lack of access and treatment in developing countries, a higher percentage of women with breast cancer die from the disease. Low and middle-income countries account for 55% of breast cancer deaths. There is also a gradient by region related to the level of economic development: in North America the ratio of mortality to incidence is less than 0.2, in Latin America and the Caribbean it is 0.35, and in Africa the ratio is almost 0.7.4,23
As compared to cervical cancer, breast cancer accounts for a greater proportion of both deaths and Disability Adjusted Life Years (DALYs) lost, on aggregate, for both low and middle income countries and high income countries (Figure 1).24,25 As a share of all cancers, breast cancer accounts for 6.4% of DALYs and 7.4% of deaths on average in lower-income regions, as compared to 7.5% and 9.7% in high-income countries. Cervical cancer accounts for 4.4% of deaths and 5.1% of DALYs in lower income countries, and for a much lower share in high-income countries -only 0.8% and 1.2% respectively.
The absolute mortality figures also illustrate these important differences across regions by income level. According to these data, in low and middle income countries a higher total number of deaths occur with 317000 women reported as dying from breast cancer as compared to 218000 deaths from cervical cancer. In high-income countries, 155000 deaths are reported from breast cancer and much fewer -17000- from cervical cancer.
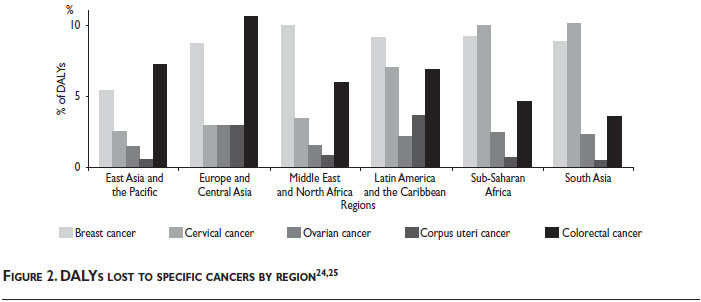
Breast cancer accounts for a large proportion of cancer-related morbidity and mortality in all regions of the developing world.24 As shown in figure 2,24,25 as a proportion of all DALYs lost to cancer, breast cancer exceeds cervical and ovarian cancer in all developing world regions except the poorest: sub-Saharan Africa and South Asia.5 In all cases, the proportion of DALYs lost is substantially higher than from ovarian or uterine cancer. Further, the figures for breast cancer also exceed colorectal cancer in all but Europe and Central Asia and East Asia and the Pacific. In Europe and Central Asia, as well as the Middle East and North Africa, breast cancer accounts for three to four times more DALYs lost than cervical cancer, and twice as many in East Asia and the Pacific. In Latin America and the Caribbean, DALYs lost from breast cancer also exceed cervical although the gap is not as large. Even in the poorest parts of the world -South Asia and sub-Saharan Africa- the proportion of DALYs lost from breast cancer is not very different to cervical cancer. The figures are approximately 10% for cervical and 9% for breast cancer. The findings are similar comparing mortality across regions.
Available data suggest that a large proportion of cases of breast cancer in developing countries are detected in pre-menopausal women. Estimates from Globocan for 2002 (based on registries and projections), suggest that in more than half of the countries of Latin America and the Caribbean, 50% of cases and 40% of deaths occur in women below age 54 (Figure 3). Further, there is some evidence that breast cancer is occurring at earlier ages on average than in developed countries, although an appropriate explanation for this phenomenon remains to be found.26
In the case of Mexico, breast cancer is the second cause of death among women aged 30 to 54 and as of 2006, more women die of breast than cervical cancer. Further, only 5-10% of cases are detected in the earliest stages (0-1) and less than 20% of women aged 40-69 report having had an annual mammogram or breast clinical exam.5
Mexico is one of the few, and possibly only, developing country that offers financial protection in health for women diagnosed with breast cancer. As of 2007, either through the Seguro Popular Program or the social security institutes, any woman diagnosed is entitled to a full range of services free of charge. This does not mean, however, that the majority of women actually have access to these services. Even the process of diagnosis can be costly and present an important barrier - mammogram with biopsy and pathology can easily cost the equivalent of 2 to 3 months of minimum wage (US$ 200-300). Estimates of average costs of treatment per patient-year in the Mexican Institute of Social Security (without accounting for institutional fixed costs like bed days) are in the range of US$ 20000-30000 (approximately $280 000 Mexican pesos calculated for 2005).27
Discussion
The data presented above show that breast cancer is becoming a pressing priority for women's health in the developing world. Informing women about their health and empowering them to take it in their hands is only a first step especially in the case of breast cancer where primary prevention is not possible. Affording treatment and effective early detection for women in poor countries remain significant challenges.
Still, it is not realistic to assume that developing countries can move to offering all women aged 40 and over mammography with on-going follow-up in the short term, and perhaps even medium term. Developing countries must place more emphasis on early detection and reduce the proportion and number of cases diagnosed in stages 3-4. This must be undertaken in the face of limited resources -financial, technological and human. Screening and early detection strategies must take into account the backlog of undetected cancers, the high proportion of cases identified in the latest stages of the disease and the lack of access to human and technological resources. While there is substantial evidence to suggest that breast self-examination is not effective in reducing mortality in populations where most cases are detected in the earliest stages of the disease,24,28,29 there is practically no evidence available for developing countries where detection often occurs in stages 3-4. A first step is to detect stage 1-2 tumors that are often palpable, especially to trained professionals. This can improve life expectancy if appropriate treatment is available. Thus, screening through self- and clinical breast examination should be considered useful, if second-best, options that require evaluations for developing countries while the infrastructure and human resources required for mammography are being extended.24
Current efforts to improve other areas of women's health provide a number of opportunities for reaching out to young women with messages about breast cancer. Antenatal care visits, as well as contacts with the health system around family planning and child care, offer an invaluable opportunity to provide information on breast cancer to women of reproductive age. Not doing this represents an important missed opportunity to address women's comprehensive needs and illustrates the limitations of vertical programs and the lack of integration with community health and other horizontal initiatives.
Linking information on early detection of breast cancer to interventions for reproductive and maternal and child health may provide an important opportunity to reach younger women. Coverage of child vaccination and antenatal care are among the highest of all health interventions. The analysis of the interventions needed to improve maternal mortality in 68 countries, which account for 97% of maternal and child deaths in the world, shows that 80% of women receive one antenatal visit or more. The figures are similar for measles vaccination. Although coverage is much lower for post-natal visits, a significant proportion of women -approximately 25%, are also reached (figure 4).30,31 Further, although coverage is much lower for skilled birth attendance and post-natal visits, a significant proportion of women are also reached.30
Current WHO guidelines suggest that good antenatal care needs to do more than just deal with the complications of pregnancy. The 2005 WHO report "Make every mother and child count" identifies three important opportunities during antenatal care that should not be missed.32 First, antenatal consultations should offer an opportunity to promote healthy lifestyles that improve long-term health outcomes for the woman, her unborn child, and possibly her family. The promotion of family planning is the foremost example of this and can have a positive impact on contraceptive use after birth. Second, antenatal care provides an opportunity to establish a birth plan. Third, the antenatal care consultation is an opportunity to prepare mothers for parenting and for what will happen after the birth. Women and their families can learn how to improve their health and seek help when appropriate, and, most importantly, how to take care of the newborn child. To date, no explicit linkage has been made with the prevention and early detection of breast cancer.33
The question that must be asked and tested in the field is not ´whether´ but rather ´how´ information about and interventions for the early detection of breast cancer -self-examination, annual breast clinical exams, regular mammography after age 40 and careful follow-up from an earlier age of women with family history- can be presented and communicated as part of these types of health care contacts. Initiatives to link these interventions should be tested and evaluated, both in terms of their impact on early detection of breast cancer and on reproductive and maternal and child health.
The idea of linking breast cancer detection to antenatal care, and more generally to reproductive and to maternal and child health interventions is an interesting example of the diagonal approach to the organization of health services.34,35 In this case, the vertical approach focusing on a specific disease -breast cancer, is linked to the horizontal approaches of maternal and child and reproductive health interventions.
Conclusions
During the last two decades, women's health has received increased attention from the international community. A little over 20 years ago, the Safe Motherhood Initiative was launched giving more visibility and attracting new resources to efforts to reduce maternal morbidity and mortality, which, until then, were problems that had been largely ignored.36 Almost 15 years ago, in 1994, the International Conference on Population and Development (ICPD) was held in Cairo. In this forum, 179 countries endorsed the adoption of a broad and comprehensive definition of sexual and reproductive health and rights, and committed to increase the resources for programs that would meet these needs. Many years after these historical milestones, maternal and reproductive health agendas are far from finished. 37
Fifteen years after ICPD, not enough progress has been made on some of the core issues in the Cairo agenda, such as family planning. Official Development Assistance has declined while the need for contraception has increased dramatically. There are an estimated 350 million women and men around the world who want to use family planning but don't have access to it.38 At the same time, other women's health issues included in the Cairo paradigmatic and visionary definition of reproductive health have not yet received the attention and resources that are required to address them in developing countries.
Such is the case of reproductive cancers and, especially, breast cancer, an obvious reproductive health issue, considering the demonstrated or likely associations with age of menarche10,15 and at first birth, number of pregnancies, duration of breastfeeding,12,13 use of hormonal contraception and of hormonal replacement therapy,18 as well as the early age at onset in the developing world.
In spite of the evidence on the heavy burden of the disease for adult women, breast cancer has not been recognized as a priority in most low and middle income countries and has not, therefore, received the attention it deserves from the international and national reproductive and maternal health communities.39 As a result, important opportunities to inform women about their own health and the risk of breast cancer are currently being missed in the developing world. We suggest that explicit linkages should be made with antenatal care, child and maternal health, and family planning to use these contacts to provide valuable information to women.
The large number of cases of breast cancer that are diagnosed among pre-menopausal women, the number of identifiable risk factors associated with reproduction, the high mortality rates among young women, and problem of late detection, suggest the importance of reaching out to young women with messages and interventions for early detection of breast cancer. This is especially relevant for many developing countries where the progress of economic development, demographic and epidemiologic transition are associated with increasing risk factors for breast cancer such as a higher age of first pregnancy.
To date, the vast majority of developing countries, with few exceptions, are unable to make breast cancer treatment available to women. As was done in the case of HIV/AIDS, it is time to challenge the unethical assumption, and the often fatal fact, that poor women cannot access cancer treatment.
Acknowledgements
We are grateful for the financial support received from the Carso Health Institute through the program Breast Cancer: Tómatelo a Pecho (Take it to Heart) and the Latin America and Caribbean Health Observatory, and the Council on Competitiveness and Health of the Mexican Health Foundation. We also thank two anonymous reviewers and Peggy Porter, Jennifer Requejo, Sonya Rabeneck, Henrik Axelson, and Carmen Elisa Florez for valuable comments; Ben Anderson of the Breast Health Global Initiative for several valuable conversations on detection strategies in developing countries; and Hector Arreola, Rebeca Moreno and Sonia Ortega for their contributions to the development of the paper. The authors take full responsibility for the views expressed in this article.
References
1. Frenk J, Bobadilla JL, Sepúlveda J, et al. Health transition in middle-income countries: New challenges for health care. Health Policy and Planning 1989;(4):29-39. [ Links ]
2. Starrs A. Safe motherhood initiative: 20 years and counting. The Lancet, Maternal Survival series; 2006; [ Links ] 2-4.
3. UNAIDS: 2008 Report on the global AIDS epidemic. Geneva, UNAIDS, 2008. [ Links ]
4. Porter P. Westernizing women's risk? Breast cancer in lower-income countries. N Engl J Med 2008;358: 213-216. [ Links ]
5. Knaul FM, Nigenda G, Lozano R, Arreola-Ornelas H, Langer A, Frenk J. Cáncer de mama en México: Una prioridad apremiante. Salud Publica Mex 2009;51:supl. [ Links ] 2
6. Hill K, Thomas K, AbouZahr C, Walker N, Say L, Inoue M, et al. and on behalf of the Maternal Mortality Working Group. Estimates of maternal mortality worldwide between 1990 and 2005: an assessment of available data. The Lancet 2007; 370(9595):1311-1319. [ Links ]
7. Ronsmans C, Graham W. Maternal mortality: who, when, where, and why. The Lancet 2006; 368(9542): 1189-1200. [ Links ]
8. Campbell OMR, Graham WJ and on behalf of the Lancet Maternal Survival Series steering group. Strategies for reducing maternal mortality: getting on with what works. The Lancet 2006; 368 (9543): 1284-1299 [ Links ]
9. Saslow D, Castle P, Cox JT, Davey D, Einstein M, Ferris D, et al. American Cancer Society Guideline for Human Papillomavirus (HPV) Vaccine Use to Prevent Cervical Cancer and Its Precursors. CA Cancer J Clin 2007;57;7-28. [ Links ]
10. American Cancer Society. Breast Cancer Facts & Figures 2007-2008. Atlanta: American Cancer Society, Inc. 2008. Available at: www.cancer.org/downloads/STT/BCFF-Final.pdf>. Accessed 25 July 2008. [ Links ]
11. Hidalgo-Miranda A, Jimenez-Sanchez G. Bases Genómicas del Cáncer de Mama: Avances hacia la medicina personalizada. Salud Publica Mex 2009;51: supl [ Links ]2.
12. World Cancer Research Fund / American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. Washington, DC: AICR, 2007. Ch. 7 Cancers: Breast. 289-295.
13. López-Carrillo L, Bravo-Alvarado J, Poblano-Verastegui O, Ortega Altamirano D., Reproductive determinants of breast cancer in Mexican women. Ann N Y Acad Sci 1997; 837:537-50. [ Links ]
14. World Health Organization (WHO). World Cancer Report. Stewart B, Kleihues P (eds.) International Agency for Research on Cancer; 2003. [ Links ]
15. McPherson K, Steel C M, Dixon JM. ABC of Breast Diseases: Breast cancer - epidemiology, risk factors, and genetics. BMJ 2000; 321. [ Links ]
16. Tehard B, Kaaks R, Clael-Chapelon F. Body Silhouette, menstrual function at adolescence and breast cancer risk in the E3N cohort study. Br J Cancer 2005; 92: 2042-2048. [ Links ]
17. Rosales E, Sordia L, Vazquez J, Iglesias JL, Morales A, Castañeda M, et al, Breast cancer in menopausal women with hormonal replacement therapy. International Congress Series 2004; 1271:414-416. [ Links ]
18. Chen CL, Weiss N, Newcomb P, et al. Hormone Replacement Therapy in Relation to Breast Cancer. JAMA 2002; 287 (6): 734-741. [ Links ]
19. Weiss L, Burkman R, Cushing-Haugen K, Voigt L, Simon M, Daling J, et al. Hormone Replacement Therapy Regimens and Breast Cancer Risk. Obstet Gynecol 2002; 100 (6):1148-1158. [ Links ]
20. Gapstur S, Morrow M, Sellers T. Hormone Replacement Therapy and Risk of Breast Cancer With a Favorable Histology: Results of the Iowa Women's Health Study. JAMA 1999; 281(22):2091-2097. [ Links ]
21. Bernstein J, López-Carrillo L, Wang L, Epidemiology of Her-2/neu and P53 in breast cancer. Salud Publica Mex 1999; 41: suppl 2:114-123. [ Links ]
22. de Vasconcelos AB, Azevedo e Silva Mendonça G, Sichieri R. Height, weight, weight change and risk of breast cancer in Rio de Janeiro, Brazil. Sao Paulo Med J 2001; 119(2): 62-6. [ Links ]
23. International Agency for Research on Cancer (IARC). OMS Globocan 2002. Available at: www.iarc.fr. [ Links ]
24. Brown ML, Goldie SJ, et al. Health service interventions for cancer control in developing countries. New York: Oxford University Press/World Bank 2006;569-589. [ Links ]
25. Lopez AD, Matheres CD, Ezzati M, Jamison DT, Murray CJL, (eds.) Global Burden of Disease and Risk Factors. New York: Oxford University Press; 2006;45-93.
26. Rodríguez-Cuevas S, Macías C, Labastida S. Cáncer de mama en México: ¿enfermedad de mujeres jóvenes? Ginecol Obstet Mex 2000:68. [ Links ]
27. Knaul FM, Arreola-Ornelas H, Velázquez E, Dorantes J, Méndez O, Ávila-Burgos L, El costo de la atención médica del cáncer mamario: el caso del Instituto Mexicano del Seguro Social. Salud Publica Mex 2009;51: supl 2:286-295. [ Links ]
28. Groot MT, Baltussen R, Uyl-de Groot CA, Anderson BO, Hortobágyi GN. Cost and health effects of breast cancer interventions in epidemiologically different regions of Africa, North America and Asia. The Breast Journal, 2006; 12: suppl. 1, S81-S90. [ Links ]
29. Thomas DB, Gao DL, Ray RM, et al. Randomized trial of breast self-examination in Shanghai: final results. J Natl Cancer Inst 2002; 94:1445-1447. [ Links ]
30. Countdown Coverage Writing Group and on behalf of the Countdown to 2015 Core Group. Countdown to 2015 for maternal, newborn, and child survival: the 2008 report on tracking coverage of interventions. The Lancet 2008; 371(9620): 1247-1258. [ Links ]
31. Bryce J, Requejo J, and the 2008 Countdown working group. Tracking progress in maternal, newborn, and child survival: the 2008 report. Available at: <http://www.countdown2015mnch.org> [ Links ]
32. The World Health Report 2005 - make every mother and child count. WHO, Geneva, Switzerland. [ Links ]
33. Antenatal care in developing countries. Promises, achievements and missed opportunities. WHO and United Nations Children's Fund. Geneva, World Health Organization, 2003. [ Links ]
34. Frenk J. Bridging the divide: global lessons from evidence-based health policy in Mexico. Lancet 2006; 368: 954-61. [ Links ]
35. Sepúlveda J, Bustreo F, Tapia R, Rivera J, Lozano R, Oláiz G, et al. Improvement of child survival in Mexico: the diagonal approach. The Lancet 2006; 368: 2017-27. [ Links ]
36. Starrs A. Preventing the tragedy of maternal deaths: a report on the Internatioal Safe Motherhood conference. Nairobi, Kenya, February 1987. Washington, DC: World Bank, 1987.
37. Report of the International Conference on Population and Development - Programme of Action (Cairo, 5-13 September 1994), A/CONF.171/13: Report of the ICPD (94/10/18), UN Population Division, Department of Economic and Social Affairs. Available at <http://www.un.org/popin/icpd/conference/offeng/poa.html> [ Links ]
38. Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A, Innis J. Family planning: the unfinished agenda. The Lancet 2006. Sexual and Reproductive Health series 2006; 47-64. [ Links ]
39. Berer M. Reproductive Cancers: high burden of disease, low level of priority. Reproductive Health Matters 2008;16(32):4-8. [ Links ]
 Address reprint requests to:
Address reprint requests to:
Felicia Marie Knaul
Fundación Mexicana para la Salud
Periférico Sur, 4809, Col. El Arenal Tepepan
Tlalpan, 14610, México, D.F
E-mail:fknaul@funsalud.org.mx
Received on: Novermber 26, 2008
Accepted on: December 17, 2008


{kind=link}
{kind=link}
{kind=link}
{kind=link}