










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud Pública de México
versión impresa ISSN 0036-3634
Salud pública Méx vol.51 supl.2 Cuernavaca ene. 2009
ARTÍCULO DE REVISIÓN
Global trends in breast cancer incidence and mortality
Cáncer de mama en el mundo
Peggy L. Porter, MD
Divisions of Human Biology and Public Health Sciences. Fred Hutchinson Cancer Research Center. Department of Pathology. University of Washington. Seattle WA, USA
ABSTRACT
This review highlights the increasing incidence of breast cancer world-wide and the increasing burden of breast cancer deaths experienced by lower-income countries. The causes of increasing incidence have been attributed to changes in the prevalence of reproductive risk factors, lifestyle changes, and genetic and biological differences between ethnic and racial groups. All these factors may contribute, but data linking etiological factors to increased risk in developing countries is lacking. The challenge for lower-income countries is developing effective strategies to reverse the trend of increasing mortality. Down-staging of breast cancer by early detection is a promising long-term strategy for preventing disease-related deaths but it is difficult to make the economic investment required to carry out broad screening programs. Successful strategies for addressing the growing breast cancer burden will therefore take political will, reliable data, public and medical community awareness, and partnerships between community advocates, governments, non-governmental organizations and biotechnology.
Key words: breast neoplasms; world health; incidence; mortality
RESUMEN
Se destaca el aumento en la incidencia de cáncer de mama (CaMa) en el mundo y la creciente carga de muertes por la enfermedad en países en desarrollo. El aumento en la incidencia se atribuye a cambios en la prevalencia de factores de riesgo reproductivo, estilo de vida, y a diferencias biológicas entre grupos étnicos y raciales. Sin embargo, aún faltan datos que relacionen los factores etiológicos al incremento en el riesgo en países en desarrollo. El desafío es generar estrategias efectivas que reviertan la tendencia en la mortalidad. La detección en etapas más tempranas es una estrategia prometedora de largo plazo pero la inversión necesaria para los programas de tamizaje es muy alta. Las estrategias exitosas para hacer frente a la creciente carga de CaMa deben tener voluntad política, evidencia confiable, reconocimiento de la comunidad pública y médica; y la suma de esfuerzos entre activistas de la comunidad, gobierno, organizaciones no-gubernamentales y biotecnología.
Palabras clave: neoplasias de mama; salud mundial; incidencia; mortalidad
Breast cancer is the most common cancer of women in the United States and affluent European countries.1 Low- and middle-resource countries have historically reported lower rates of breast cancer than high-resource countries. However, over the past twenty to thirty years, data support a trend of increasing incidence and mortality from breast cancer in lower resource countries. Of the over million new cases of breast cancer that will be diagnosed worldwide in 2009, low- and middle-resource countries will be burdened with 45% of breast cancer cases and 55% of breast cancer-related deaths.2-4 This review will highlight the challenges presented by the global increase in breast cancer incidence and mortality and discuss some of the current thinking about reasons for this increase and approaches to address the rising mortality from breast cancer in low and middle income countries.
Breast cancer incidence worldwide
It should be noted at the outset of any discussion of global trends in cancer that the limited data available for many countries is a hindrance to truly understanding the complexity of the global breast cancer burden. Incidence figures are based on data from small geographic areas that are often pooled and extrapolated to large regions. Reported rates may reflect only the women who are easiest to reach or who have the highest standard of living. Thus, current global figures cannot truly reflect the underlying economic and cultural diversity driving increased incidence and related mortality.
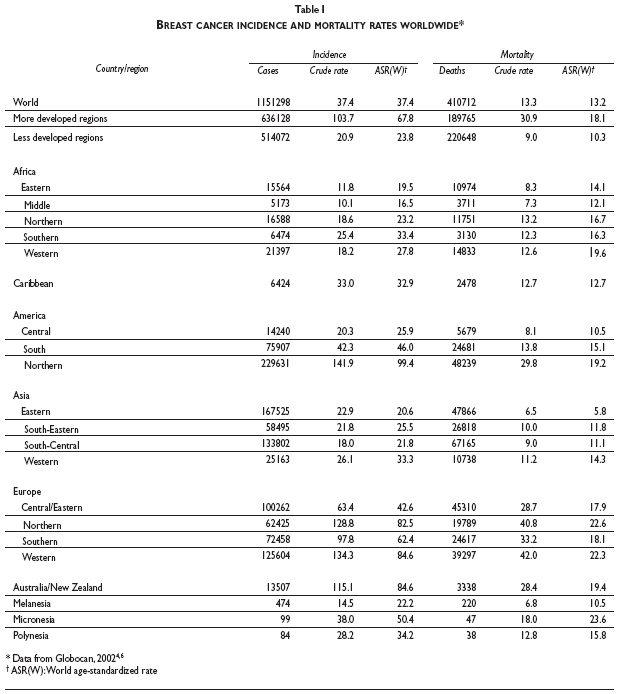
Breast cancer incidence is highest in the more-developed regions of the world, in urban populations, and in Caucasian women. The Globocan database for 2002, indicates that the age-standardized rate (ASR) of breast cancer incidence is 67.8 per 100000 in more-developed regions (Europe, Australia, New Zealand, North America and Japan) compared with 23.8 per 100000 in less-developed regions (Africa, Central America, South America, all regions of Asia except Japan, the Caribbean, Melanesia, Micronesia and Polynesia).4 The highest incidence (ASR) occurs in North America (99.4 per 100000) and the lowest in Asia (22.1) and Africa (23.4) (Table I). When analyzed by country income (determined by World Bank data for 2006), mean values for breast cancer incidence are highest for groups of countries with the highest gross domestic product (GDP) per capita and a high percent urban population.5
Breast cancer incidence varies widely within regions and countries, likely due to differences in racial and ethnic make-up, health resources, and lifestyle patterns. Incidence in largely rural and black sub-Saharan Africa (16.5 per 100000), for instance, is half that of South Africa (33.5 per 100000), which has a higher proportion of urban white women.6 In China, the 1993-1997 incidence of breast cancer in urban Shanghai was 27.2 per 100000 compared with 11.2 per 100000 in the more rural Qidong county.7,8 In Korea there was an almost two-fold difference in incidence between Seoul (20.8 per 100000) and more rural Kanghwa county (12.7 per 100000).8
The wide differences in global incidence rates and resources have led to diverse approaches to breast cancer control. In the West, high rates and abundant resources have resulted in intense laboratory and clinical research as well as aggressive screening programs and abundant treatment trials. In resource-poor countries with low rates, the ability and incentive to mount large efforts to address breast cancer have been lacking. However, the perspective on breast cancer control in lower income countries is changing because of the clear trend of steeply increasing incidence largely affecting countries with historically low rates of breast cancer.9 In Asia; Japan, Singapore, and Korea have reported doubled or tripled incidence over the past 40 years and China's urban registries documented a 50% increase in the years between 1972 and 1994.10 India similarly reported increased incidence in urban Bombay (Mumbai) from 1978 to 1997 (20.5 to 31.5 per 100000).8 In Africa, trends in breast cancer incidence are difficult to evaluate, given the general lack of large registries and accurate population data. However, local registry efforts in Uganda, reported increased incidence from 11.7 in 1960 to 23.4 in 2002.11 Some Latin American countries have also reported increasing incidence: in Cali, Colombia rates increased from 32.2 in 1983 to 44.4 in 1997. However, in Costa Rica, which has one of Latin America's only national registries, the rate has remained fairly constant at around 30 per 100000.8,12
Risk factor distribution and breast cancer incidence
Reproductive factors that increase breast cancer risk include a long menstrual history (early menarche and late menopause), never having children, having one's first child after age 30, never breastfeeding, being overweight or obese after menopause, use of postmenopausal hormone therapy (specifically, combined estrogen and progestin therapy), physical inactivity, and consumption of one or more alcoholic beverages per day.13
In affluent Western countries, women have relatively high social status, delay childbearing, have relatively few children and, until recently, commonly used hormone-replacement therapy. These reproductive risk factors, which are primarily associated with an increased risk of postmenopausal breast cancer, are postulated as the reason for the higher rates of post-menopausal breast cancer seen in high resource countries compared with lower resource countries.4 What is still unclear is the relationship of these reproductive risk factors to increasing incidence rates in younger women in developing countries. Many countries with rapidly increasing rates of breast cancer, including Asian and Latin American countries, report an earlier peak of breast cancer than Western countries.4 In Hong Kong, a recent study found that the percentage of Chinese women with breast cancer younger than 40 years old was 17.6 (compared with around 6% in US Caucasians) and that the mean age at menarche was lower and the age at first live birth was higher in Chinese women under age 40 compared with Chinese women over age 40.14 As has been reported in U.S. women, the younger Chinese women presented with more advanced disease and more aggressive tumor characteristics than the older Chinese women.14 It is becoming increasingly important to understand how breast cancer in young women is influenced by the accepted reproductive risk factors and determine if there are other more relevant risk factors that may be related to breast cancer incidence in countries with rapidly increasing rates in young women.
Even though the risks associated with diet, obesity, and exercise are not consistent between studies in the US and Europe, these factors are often cited as the cause of the increasing breast-cancer rates in developing countries. Migration studies that have revealed increases in breast-cancer incidence following migration from low-incidence countries to higher-incidence countries support the role of lifestyle changes in altering breast cancer risk, but it is difficult to pinpoint the individual contributing factors.15 High fat intake, low vegetable intake, and low soy intake have all been implicated, but the data have not been consistent or conclusive. In one of the largest nutritional studies of women in Shanghai China, an aggregate "meat-sweet" diet was associated with only a modest increased risk of breast cancer compared with a more traditional vegetable-rich diet.16 Risk of postmenopausal (but not premenopausal) breast cancer is increased among obese women, and physical exercise probably decreases the risk of postmenopausal breast cancer.17 Early age at menarche, another important reproductive risk factor for breast cancer, is associated with higher caloric intake, exercise and body mass profile and it is apparent that a trend toward decreasing age at menarche will affect breast cancer rates in lower-resource countries as diet and exercise patterns change.18-20 It will be important to understand these early life habits to completely understand the underlying causes of world-wide increasing breast cancer incidence.
Mortality from breast cancer
The worldwide ASR for mortality from breast cancer between 1993 to 2001 was 13.2 per 100000, ranging from 8.8 in Asia to 19.7 in Europe.4 The rate in 'more developed' countries was 18.1 compared with 10.4 in 'less developed' countries (Table I). The higher overall mortality rate in high resource countries reflects the high incidence of the disease in many of those countries. However, the burden of deaths due to breast cancer in lower resource countries is disproportionately high. Although the ratio of the mortality rate to incidence rate (MR:IR) world-wide is 0.35, it varies widely and ranges from a high of 0.69 in Africa to a low of 0.19 in North America.
High mortality rates in low resource countries are primarily due to late-stage disease presentation. For example, the high MR:IR ratio in Africa to a large degree reflects the high proportion of women in many African countries who present with late-stage cancer. In sub-Saharan African countries, small studies indicate that up to 90% of women present with stage III or VI disease, many with large tumors (median of 10 cm) and clinically apparent lymph node metastases.21 These late-stage tumors can not be treated successfully in the most optimal setting.
Inadequate health care systems also contribute to high mortality rates. There are no examples of universal breast cancer screening in low resource countries that could down-stage breast cancer diagnoses. In addition, there are typically only a few hospitals that can administer radiotherapy and chemotherapy and very few trained oncologists (Nigeria, for instance, has approximately 100 oncologists for a population of 140 million).5 National expenditure on health care overall inversely correlates with mortality from breast cancer, but there are exceptions.5 In Cuba, health expenditure is only moderate but mortality remains lower than that in the US (2004 ASR 14.2 and 15.6 respectively) where per capita health care spending is the highest in the world.5,22 Sweden also spends less on health care as a percent of GDP than the US, but maintains a similar mortality rate (2004 ASR 15.6). Given these kinds of exceptions, it is important that not only the total health expenditure but the distribution of that expenditure into effective private or public systems be considered when judging approaches to reducing the burden of breast cancer.
Biological differences in breast cancer worldwide
Although disparities in mortality can be attributed largely to limited screening and awareness of breast cancer leading to late stage disease, and to marginal health care, there are also ongoing efforts to understand the genetic and biologic differences that might affect disease outcomes in lower-resource countries. The presence or absence of estrogen-receptor (ER) expression in breast tumors is central to their behavior and treatment. In the US, postmenopausal onset and hormone-replacement therapy are risk factors for ER-positive breast cancer and ER-negative breast cancer is associated with both young age at diagnosis and black race.23,24 These relationships might predict a higher burden of ER-negative breast cancer in lower-resource African countries where younger average age at onset, limited use of hormone-replacement therapy, and black race predominate but, since ER testing is a luxury in most developing countries, data are lacking to address this possibility. The incidence curves by age at diagnosis of ER-negative and ER-positive breast cancer are similar to the incidence curves of low- and high-incidence rate countries, respectively, and it has been suggested that this indicates differences in breast cancer biology between the high-incidence and low-incidence populations.4 Rather than differences in biology, it is also possible that the lack of active screening programs in lower-resource countries results in the diagnosis of a higher percentage of ER-negative tumors, since mammography tends to identify the smaller ER-positive tumors.25,26
The need for global data about genetic and biologic influences on breast cancer is supported by recent small studies in black American women revealing a higher frequency of ER negative and the aggressive "triple-negative" tumors (tumors that don't express ER, progesterone receptor, or the oncogene c-erbB2/HER2) than that among white women.23,27-29 In white women, such tumors are associated with inherited mutations in the breast-cancer gene BRCA1, and genetic determinants in African women may predispose them to high-risk tumors. Although cancer-predisposing BRCA1 and BRCA2 founder mutations occur at high frequencies in various populations (such as Ashkenazi Jews), significant differences in mutation rates between races have not been demonstrated. However, there appear to be differences in the spectrum of BRCA-1 and BRCA-2 mutations, as well as the rates of BRCA variants of unknown significance between Caucasian, African and Asian women.30-33 Although there are currently not enough data to assess how these differences in inherited mutations might explain differences in incidence and mortality, there is a growing need to elucidate the genetic and biologic contributions to breast-cancer risk for women of all racial and ethnic backgrounds.
Approaches to reducing breast cancer incidence and mortality
Although progress in slowing the rate of increasing incidence would be desirable, the increasing prevalence of lifestyle habits that accompany improving economic conditions -delayed childbearing, lower parity, reduced breast-feeding, and a sedentary workplace- are expected to continue to drive up breast cancer incidence rates in lower and middle resource countries in the coming decades. The most important task will be to alter the trend of increasing mortality that will accompany the increasing rate. The strategies that have been most effective in predominantly Caucasian, affluent populations have been early detection through mammography, targeted hormonal and anti-HER2 therapies, and improvements in chemotherapy. The common presentation of breast cancer at advanced stage in lower income countries is undoubtedly one of the main reasons for high mortality rates; metastatic disease is not treated successfully in countries with the highest resources. Down staging of breast cancer by early detection is seen as one of the most promising long-term strategies for preventing disease-related deaths but it is difficult for many countries to make the economic investment required to carry out broad screening programs. The lowest cost screening modality, breast self exam (BSE), can find individual tumors and increase awareness and acceptance of breast health in the population but does not appear to lower mortality from the disease.34 Clinical breast exam (CBE) can improve detection of early stage cancers and clinical follow-up within the health care system35 and efforts are being made in many countries to train medical personnel to conduct high quality CBE. Full-scale mammography screening has been successful in reducing mortality in developed countries,36 but this requires considerable human, health system and technical resources. It is likely that a combined introduction of BSE, CBE and mammographic screening as is possible for an increasing proportion of the population, will be the most feasible course of action for lower resource countries. The multinational group involved in the Breast Health Global Initiative have incorporated economic and cultural information into guidelines to help plan just such country-specific breast cancer early detection strategies in lower-resource countries with different racial, ethnic, and cultural makeup.37
It is clear that breast cancer will be an increasing burden in many countries and there will have to be a redirection of health resources to diagnose, treat and monitor the growing numbers of women who are affected by the disease. This will take political will, reliable data and cancer registries, public and medical community awareness, and partnerships between advocates, government, foundations and NGOs, and biotechnology companies. These partnerships can provide the incentives and the means to make crucial advances in lowering the unacceptable burden of mortality in lower resource countries.
References
1. American Cancer Society. Cancer Facts & Figures 2008. Atlanta: American Cancer Society, 2008. [ Links ]
2. Global Cancer Facts & Figures 2007. Atlanta, GA: American Cancer Society, 2007. [ Links ]
3. Curado M, Edwards B, Shin H, Storm H, Ferlay J, Heanue M, et al., editors. Cancer incidence in five continents, vol. IX. Lyon, France: IARC, 2007.
4. Kamangar F, Dores G, Anderson W. Patterns of cancer incidence, mortality, and prevalence across five continents: Defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24(14):2137-2150. [ Links ]
5. Igene H. Global health inequalities and breast cancer: an impending public health problem for developing countries. Breast J. 2008;14:428-434. [ Links ]
6. Ferlay J, Bray F, Pisani P. Globocan 2002: Cancer Incidence, mortality and prevalence worldwide. Lyon, France: IARC Press, 2002. [ Links ]
7. Chen J-G, Zhu J, Parkin D, Zhang Y-H, Lu J-H, Zhu Y-R, et al. Trends in the incidence of cancer in Qidong, China, 1978-2002 Int J Cancer. 2006;119:1447-1454. [ Links ]
8. Parkin D, Whelan S, Ferlay J, Storm H. Cancer incidence in five continents, vol. I to VIII Lyon, France: IARC CancerBase, 2005. [ Links ]
9. Parkin DM, Muir C, Whelan SI. Cancer Incidence in 5 continents. Lyon, France: IARC Scientific Publications, 1992. [ Links ]
10. Jin F, Devesa S, Chow W-H, Zheng W, Ji B-T, Fraumeni J, et al. Cancer incidence trends in urban Shanghai, 1972-1994: An update. Int J Cancer. 1999;83:435-440. [ Links ]
11. Parkin D, Sitas F, Chirenje M, Stein L, Abratt R, Wabinga H. Part I: Cancer in indigenous Africans--burden, distribution, and trends. Lancet Oncol 2008;9:683-692. [ Links ]
12. Secretaría de Salud. Sistema Único de Información para la Vigilancia Epidemiologica. Anuarios de Morbilidad. 2000-2006. 2006. México, DF: Secretaría de Salud. Dirección General de Epidemiología, 2007. [ Links ]
13. Key T, Verkasalo P, Banks E. Epidemiology of breast cancer. Lancet Oncol 2001;2:133-140. [ Links ]
14. Kwong A, Cheung P, Chan S, Lau S. Breast cancer in Chinese women younger than age 40: Are they different from their older counterparts? World J Surg. Epub. 2008. [ Links ]
15. Ziegler R, Hoover R, Pike M, Hildesheim A, Nomura A, West D, et al. Migration patterns and breast cancer risk in Asian-American women. JNCI. 1993;85(22):1819-1827. [ Links ]
16. Cui X, Dai D, Tseng M, Shu X-O, Gao Y-T, Zheng W. Dietary patterns and breast cancer risk in the Shanghai Breast Cancer Study. Cancer Epidemiol Biomarkers Prev 2007;16:1443-1448. [ Links ]
17. AICR. World Cancer Research Fund/American Institute for Cancer Research. Food, nutrition, physical activity, and the prevention of cancer: A Global perspective. Washington D.C.: American Institute for Cancer Research; 2007. [ Links ]
18. Hoel D, Wakabayashi T, Pike M. Secular trends in the distributions of the breast cancer risk factors -menarche, first birth, menopause, and weight- in Hiroshima and Nagasaki, Japan. Am J Epidemiol. 1983;118:78-89. [ Links ]
19. Koprowski C, Ross R, Mack W, Henderson B, Bernstein L. Diet, body size and menarche in a multiethnic cohort. Br J Cancer. 1999;79:1907-1911. [ Links ]
20. Meyer F, Moisan J, Marcoux D, Bouchard C. Dietary and physical determinants of menarche. Epidemiology 1990;1:377-381. [ Links ]
21. Fregene A, Newman L. Breast cancer in sub-Saharan Africa: How does it relate to breast cancer in African-American women? Cancer 2005;103:1540-1550. [ Links ]
22. World Health Organization, mortality database. Available in: http://www.who.int/whosis/whosis/. Accessed on: December 2008. [ Links ]
23. Carey L, Perou C, Livasy C, Dressler L, Cowan D, Conway K, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006;295:2492-2502. [ Links ]
24. Porter P, Malone K, Heagerty P, Alexander G, Gatti L, Firpo E, et al. Expression of cell-cycle regulators p27Kip1 and cyclin E, alone and in combination, correlate with survival in young breast cancer patients. Nature Medicine 1997;3(2):222-225. [ Links ]
25. Narod S, Dube M. Biologic characteristics of interval and screen-detected breast cancers. JNCI 2001;93:151-152. [ Links ]
26. Porter P, El-Bastawissi A, Mandelson M, Lin M, Khalid N, Watney E, et al. Breast tumor characteristics as predictors of mammographic detection: Comparison of interval-and screen-detected cancers. J Natl Cancer Inst 1999;91(23):2020-2028. [ Links ]
27. Lund M, Trivers K, Porter P, Coates R, Leyland-Jones B, Brawley O, et al. Race and triple negative threats to breast cancer survival: a population-based study in Atlanta, GA. Breast Cancer Res Treat. Epub. 2008. [ Links ]
28. Porter P, Lund M, Lin M, Yuan X, Liff J, Flagg E, et al. Racial differences in expression of cell cycle regulatory proteins in breast cancer: Study of young African American and white women in Atlanta. Cancer 2004;100(12):2533-2542. [ Links ]
29. Rakha E, Reis-Filho J, Ellis I. Basal-like breast cancer: A critical review. J Clin Oncol 2008;26:2568-2581. [ Links ]
30. John E, Miron A, Gong G, Phipps A, Felberg A, Li F, et al. Prevalence of pathogenic BRCA1 mutation carriers in 5 US racial/ethnic groups. JAMA 2007;298:2869-2876. [ Links ]
31. Liede A, Narod S. Hereditary breast and ovarian cancer in Asia: genetic epidemiology of BRCA1 and BRCA2. Hum Mutat 2002;20:413-424. [ Links ]
32. Olopade O, Fackenthal J, Dunston G, Tainsky M, Collins F, Whitfield-Broome C. Breast cancer genetics in African Americans. Cancer 2003;97(1 Suppl):236-245.
33. Rashid M, Zaidi A, Torres D, Sultan F, Benner A, Naqvi B, et al. Prevalence of BRCA1 and BRCA2 mutations in Pakistani breast and ovarian cancer patients. Int J Cancer 2006;119:2832-2839. [ Links ]
34. Thomas D, Gao D, Ray R, Wang W, Allison C, Chen F, et al. Randomized trial of breast self-examination in Shanghai: Final results. JNCI 2002;94:1445-1457. [ Links ]
35. Okonkwo Q, Draisma G, der Kinderen A, Brown M, de Koning H. Breast cancer screening policies in developing countries: a cost-effectiveness analysis for India. J Natl Cancer Inst 2008;100:1290-1300. [ Links ]
36. Cronin K, Feuer E, Clarke L, Plevritis S. Impact of adjuvant therapy and mammography on US mortality from 1975 to 2000: Comparison of mortality results from the CISNET Breast Cancer Base Case Analysis In: JNCI, editor. The impact of mammography and adjuvant therapy on US breast cancer mortality (1975-2000): Collective results from the Cancer Intervention and Surveillance Modeling Network: J Natl Cancer Inst Monogr 2006:112-121. [ Links ]
37. Anderson B. Guidelines for international breast health and cancer control-implementation. Cancer 2008;113(S8):2215-2371. [ Links ]
 Address reprint requests to:
Address reprint requests to:
Peggy L. Porter, M.D.
Fred Hutchinson Cancer Research Center
1100 Fairview Ave N, Seattle WA 98109, USA
E-mail: pporter@fhcrc.org
Received on: November 24, 2008
Accepted on: December 16, 2008


{kind=link}