











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Chronic kidney disease (CKD) is one of the disease entities causing the greatest economic and social burden in Mexico1. The main cause of CKD in the world is diabetes mellitus (DM). In underdeveloped countries, the frequency of CKD of "unknown origin" is increasing in young adults. In 2020, the incidence of end-stage renal disease (ESRD) in the United States was estimated in 374.8 cases per million/population (pmp), with a prevalence of 2,242 cases pmp2. Although there are no registries in Mexico that can be used to conduct an epidemiological analysis of CKD, in 2018 the state of Aguascalientes created a CKD registry that reported a prevalence of 1,883 pmp and those patients on replacement therapy, placing this entity in the ninth position in the world2. Unlike reports on global observations, the most frequent cause of ESRD is of "unknown origin," followed by DM. Its prevalence is highest in the 30-40-year-old age group, and 70% of cases were classified as renal disease of "unknown origin"3,4. Based on these observations, in 2020, we conducted CKD screening in the state of Aguascalientes; 513 adolescents were included, and the prevalence of persistent albuminuria (pA) was 3.7% (95% CI 2.1-5.3), a much higher value than that reported internationally (1.9%)5-8.
The histological and clinical characteristics of the adolescents with pA in Aguascalientes, reported by Díaz et al. in 2022, suggest that oligonephrony may be associated with environmental factors and genetic predisposition5,9. Fibrosis, either in the glomerular space or in the tubulo-interstitium, is the histological hallmark of CKD. The development of fibrosis is triggered by the incursion of inflammatory cells and cytokines that locally increase fibroblasts and the release of growth factors, that is, transforming growth factor-β and connective tissue growth factor, that lead to the loss of nephrons and promote the epithelial-mesenchymal transition10.
TFG-β and proteinuria are markers of CKD progression but they reflect late functional changes more than early structural kidney abnormalities and may also vary depending on the patient's sex, age, race, muscle mass, and metabolism, among other factors11. The scarcity of minimally invasive sensitive and specific markers for the timely detection and prediction of CKD course has led to current intense research on possible markers, using urine as the ideal source12.
We have recently identified in our laboratory a promising CKD biomarker, SerpinA3 (alpha-1-antichymotrypsin). SerpinA3 is a member of the serine protease inhibitor superfamily. Cathepsin G is the main protease target of SerpinA3; it is expressed in neutrophil azurophilic granules and increases in inflammatory processes, although its role in the kidney is not clear13. We have previously shown that uSerpinA3 levels increase in animals and patients with CKD of various etiologies, and that in experimental CKD, increases in uSerpinA3 precede fibrosis and renal dysfunction, suggesting that it could potentially detect CKD in a timely manner. In the same context, we have shown that heat-shock protein-72 (HSP-72) is a reliable biomarker in the detection of acute kidney injury, since it significantly increases in urine (uHSP72) up to 48 h before serum creatinine increases or urinary output decreases14.
Urinary podocalyxin (PCX) is a transmembrane protein located at the apical surface of glomerular podocytes, and it is the main component of the glomerular basement membrane. PCX plays an important role in normal glomerular development and in podocyte architecture; furthermore, several authors have reported that PCX is released from injured podocytes into urine and can be detected in patients with direct podocyte injury and thus, it facilitates the detection of several glomerular diseases15,16. Finally, nephrin, a protein encoded by the NPHS1 gene, is a key structural molecule of the slit diaphragm of podocytes, whose function hinges on its interaction with the actin cytoskeleton. It has been identified as a potential biomarker of podocyte injury, and it appears before the development of clinically significant microalbuminuria. Some studies have suggested that podocyte dysfunction may correlate with the number of podocytes in urine and an abnormal expression of nephrin in renal tissue, and therefore, may be associated with renal dysfunction15,17. Both markers correlate with renal parameters such as microalbuminuria, serum creatinine, and the estimated glomerular filtration rate, and may therefore become biomarkers in the early detection of CKD18.
The high prevalence of CKD of unknown origin in young adults in Aguascalientes, Mexico, and the high incidence of early CKD (G1A2) in adolescents encouraged the search for non-invasive strategies that can detect CKD in early stages and delay its progression into full-blown ESRD. Our work has the hypothesis that the presence of albuminuria and its persistence will condition a higher expression of SerpinaA3 and Hsp72 and a lower presence of nephrin and PCX. Hence, the aim of this study was to identify the presence of potential biomarkers of early renal injury in patients with pACR, and that coincide with the characteristic nephropathy profile that prevails in this entity.
METHODS
Participant selection and group assignment
This is a cross-sectional, analytical, and comparative study. Study participants were classified into four groups (negative control, isolated albuminuria, pA, and positive control). The selection of the first three groups was based on the results of CKD screening among adolescents between the ages of 10 and 17, and without a previous history of CKD, in the municipality of Calvillo (Aguascalientes, Mexico)5. We obtained the first morning urine and peripheral blood serum to determine the albumin-creatinine ratio (ACR), and estimated the GFR with Schwartz equation. Patients with an ACR < 30 mg/g were classified as negative controls, those with an ACR≥30 mg/g were programmed to repeat the laboratory tests. In the second sample, after a median of 5 months interquartile range (IQR 0.36-5.3), patients with an ACR < 30 mg/g were classified as isolated ACR (iACR), while those with an ACR≥30 mg/g were assigned to the pACR group. The positive control group included patients with established glomerular disease confirmed by biopsy, and they were recruited from the Centenario Hospital Miguel Hidalgo glomerulopathy consult. This study is based on the guidelines of the STROBE statement (Fig. 1; Supplementary data, material 1 and material 2).

Urinary biomarker evaluation method
We obtained kidney function tests. Peripheral blood samples were collected after a 12 h. overnight fast. The serum was separated and stored at −80°C until tested. The first morning urine was collected and stored in Eppendorf™ tubes in the same conditions for subsequent processing and evaluation.
The analyzed urine biomarkers were determined by Western blot and enzyme-linked immunosorbent assay (ELISA). SerpinA3 was analyzed by electrophoresis with a denaturing acrylamide gel at 8.5% and 10 µL of urine. The proteins were transferred to a pre-balanced polyvinylidene difluoride membrane (Millipore) with a 1× transfer buffer (190 mM glycine, 2 mM Tris Base, 0.1% SDS) in a trans-blot turbo system (BioRad) for 90 min, and with a TBS blocking buffer at 5%. After blocking, the membranes were incubated with the primary anti-SerpinA3/alpha-1-antichymotrypsin antibody (1:1000, ProteinTech®, 55480-I-AP) overnight at 4°C. They were subsequently incubated with the secondary HRP-coupled anti-rabbit antibody (1:5000, SIGMA®, A-0545) for 90 min. The same procedure was used to determine the presence of HSP-72, but with an anti-h/m/rHSP70 (1:2500, R&D®, MAB1663) primary antibody and an HRP-coupled anti-mouse (1:2000, Jackson®, 115-035-174) secondary antibody. Proteins were detected with an improved chemiluminescence kit. Optical density values were corrected for serum creatinine levels, as previously reported19.
We obtained specific ELISA kits for PCX and nephrin analyses (PCX #MBS765311-96, ELISA kit; MyBioSource®) – (Nephrin [NPHN] #MBS2021869-96, ELISA kit MyBioSource®), and read the values of the proteins with an ELISA reader (Multiskan FC Thermo Scientific™), following the manufacturer's instructions.
The study was conducted in accordance with the principles of the Declaration of Helsinki. The nature of the study and all possible risks was explained to all participants and they signed the required consent form. The Institutional Research and Ethics Committee of the Centenario Hospital Miguel Hidalgo approved the study on October 7, 2020 (approval number: 2020-E-30).
Statistical analysis
Data are presented as the mean and standard deviation or the median and IQR depending on the distribution of the variables. The distribution was evaluated with the Kolmogorov–Smirnov test. Dichotomic and ordinal variables were expressed as relative and absolute frequencies. Differences between groups were analyzed by ANOVA or with the Kruskal–Wallis test, and comparisons were analyzed with the post hoc Dunn or Tukey tests. Group characteristics were also compared with the Mann–Whitney U-test for independent variables. We used the SPSS Statistics v.26 software (IBM, EE.UU.). p < 0.05 was considered significant.
RESULTS
Between February 2020 and April 2021, we recruited 91 patients. Sixty-six patients detected in the CKD screening process were classified as follows: negative control (n = 25), iACR (n = 22), and pACR (n = 19). Twenty-five cases with biopsy-confirmed glomerular disease were assigned to the positive control group.
Clinical patient characterization
The median age of the study population was 19.3 ± 12.7 years and the sex proportion was almost the same (females, 49.4%). The most significant differences were found between the positive control group and the other groups (body mass index, creatinine, and GFR) (Table 1). The pACR group had an average age of 12.9 (± 1.1) years with a greater proportion of females (n = 11, 57.9 %). Only two patients in the pACR group had a GFR below 90 mL/min/1.73m2 (42 and 85 mL/min/1.73m2).
Table 1 Comparison of somatometric and biochemical characteristics between classification groups
| Characteristic, m (±SD) | Total (n = 91) | Negative control (n = 25) | Isolated albuminuria (n = 22) | Persistent albuminuria (n = 19) | Positive control (n = 25) | p-value |
|---|---|---|---|---|---|---|
| Age (years) | 19 (12.7) | 13.2 (1.1) | 13.9 (1.4) | 12.9 (1.1) | 35.0 (15.7) | < 0.001 |
| Female sex, n (%) | 45 (49.5) | 8 (32) | 11 (50) | 11 (57.9) | 15 (60) | 0.200 |
| Weight (kg) | 57.8 ± 16.1 | 58.2 ± 10.7 | 49.5 ± 13.9 | 48.6 ± 14.2 | 72.1 ± 14.4 | < 0.001 |
| Height (cm) | 160.7 ± 9.0 | 161.0 ± 7.0 | 160.5 ± 10.0 | 156.8 ± 8.9 | 163.7 ± 9.3 | 0.098 |
| BMI (kg/m2) | 22.1 ± 4.9 | 22.3 ± 3.5 | 19.0 ± 3.7 | 19.3 ± 3.6 | 26.8 ± 4.3 | < 0.001 |
| Abdominal circumference (cm) | 77.5 ± 10.8 | 81.5 ± 8.9 | 73.8 ± 10.8 | 72.7 ± 12.3 | 0.027 | |
| SBP (mmHg) | 119.6 ± 14.5 | 124.8 ± 18.5 | 117.6 ± 12.1 | 118.3 ± 12.7 | 117.3 ± 12.5 | 0.231 |
| DBP (mmHg) | 74.8 ± 9.8 | 78.9 ± 8.5 | 72.8 ± 10.8 | 74.4 ± 10.1 | 72.6 ± 9.3 | 0.088 |
| Serum creatinine (mg/dL) | 0.8 ± 0.6 | 0.6 ± 0.0 | 0.5 ± 0.1 | 0.6 ± 0.2 | 1.5 ± 0.8 | < 0.001 |
| GFR (mL/min/1.73m2) | 102.1 ± 35.5 | 110.8 ± 14.3 | 118.8 ± 38.1 | 113.4 ± 25.1 | 65.7 ± 32.6 | < 0.001 |
| Urine creatinine (mg/dL) | 179.4 ± 242.8 | 123.1 ± 69.1 | 128.7 ± 89.1 | 150.7 ± 154.4 | 486.4 ± 539.2 | 0.813 |
| Albumin to creatinine ratio (mg/g), median (IQR) | 19.5 (10.5–50.6) | 11.0 (8.2–20.1) | 14.6 (11.1–26.4) | 48.9 (40.0–71.0) | 478.5 (101.7–972.8) | < 0.001 |
Data shown as means and standard deviation (n = 91 total). Statistical analysis with ANOVA or Kruskal Wallis tests according to distribution. p < 0.05 was considered significant. m: mean; SD: standard deviation; kg: kilogram; cm: centimeters; SBP: systolic blood pressure; DBP: diastolic blood pressure; GFR: glomerular filtration rate; mmHg: millimeters of mercury; mL: milliliters; mg: milligrams; dL: deciliter; g: grams.
Complementary studies were performed only in patients with some degree of albuminuria. Among the biochemical characteristics that were significantly different between groups were BUN, urea, creatinine, uric acid, cholesterol, triglycerides, and serum albumin (p < 0.001), which have already been reported in previous studies5 (Table 2).
Table 2 Comparison of biochemical characteristics between albuminuria groups
| Characteristic, m (±SD) | Total (n = 66) | Isolated albuminuria (n = 22) | Persistent albuminuria (n = 19) | Positive control (n = 25) | p-value |
|---|---|---|---|---|---|
| Glucose (mg/dL) | 97.0 ± 11.3 | 96.4 ± 6.9 | 97.9 ± 5.1 | 96.6 ± 17.1 | 0.266 |
| Serum BUN (mg/dL) | 17.0 ± 10.8 | 11.5 ± 3.1 | 11.6 ± 4.3 | 26.1 ± 12.7 | < 0.001 |
| Serum urea (mg/dL) | 36.6 ± 23.2 | 24.6 ± 6.8 | 24.8 ± 9.3 | 56.4 ± 26.7 | < 0.001 |
| Serum uric acid (mg/dL) | 5.5 ± 1.6 | 4.9 ± 0.9 | 5.0 ± 1.6 | 6.9 ± 1.8 | 0.002 |
| Total cholesterol (mg/dL) | 171.5 ± 61.8 | 143.8 ± 21.9 | 147.3 ± 30.3 | 218.0 ± 79.0 | < 0.001 |
| Triglycerides (mg/dL) | 138.7 ± 97.6 | 93.2 ± 29.8 | 120.1 ± 56.2 | 196.2 ± 134.7 | < 0.001 |
| Serum albumin (g/dL) | 4.5 ± 0.7 | 4.8 ± 0.2 | 4.8 ± 0.2 | 3.6 ± 1.0 | < 0.001 |
| Sodium (mmol/L) | 139.8 ± 3.4 | 140.2 ± 2.1 | 140.6 ± 2.4 | 137.9 ± 5.7 | 0.560 |
| Potassium (mmol/L) | 4.3 ± 0.4 | 4.3 ± 0.3 | 4.3 ± 0.4 | 4.2 ± 0.3 | 0.934 |
| Chlorine (mmol/L) | 106.1 ± 5.7 | 107.1 ± 8.3 | 105.1 ± 2.6 | 106.3 ± 4.6 | 0.375 |
| Phosphorus (mg/dL) | 4.4 ± 0.7 | 4.5 ± 0.8 | 4.3 ± 0.8 | 4.0 ± 0.5 | 0.282 |
| Magnesium (mg/dL) | 1.9 ± 0.2 | 1.9 ± 0.3 | 1.9 ± 0.1 | 2.0 ± 0.1 | 0.382 |
| Calcium (mg/dL) | 9.7 ± 0.5 | 9.9 ± 0.2 | 9.9 ± 0.2 | 9.0 ± 0.8 | 0.001 |
| Urine volume (mL) | 1280.2 ± 824.1 | 1038.2 ± 482.7 | 944.3 ± 454.0 | 2334.4 ± 1013.9 | < 0.001 |
| Hemoglobin (g/dL) | 14.3 ± 2.0 | 15.2 ± 0.9 | 14.8 ± 1.0 | 13.2 ± 2.7 | 0.034 |
| Hematocrit (%) | 42.3 ± 5.2 | 44.5 ± 2.4 | 43.6 ± 2.7 | 39.5 ± 7.0 | 0.027 |
| Leukocytes (×103/uL) | 7.2 ± 2.2 | 7.1 ± 1.2 | 6.4 ± 2.0 | 7.9 ± 2.7 | 0.050 |
| Platelets (×103/uL) | 276.4 ± 65.5 | 290.8 ± 71.8 | 286.5 ± 57.4 | 256.7 ± 64.5 | 0.374 |
Data shown as means and standard deviation (n = 66 total). Statistical analysis with ANOVA or Kruskal Wallis tests according to distribution. p < 0.05 was considered significant. m: mean SD: standard deviation; BUN: ureic nitrogen; mL: milliliters; mg: milligrams; dL: deciliter; g: grams.
Renal biopsy
Of the total number of patients with pACR (n = 19) with indication for renal biopsy, only 18 of them gave their consent. The mean number of glomeruli obtained per biopsy was 16 (IQR 13–20); 33.3% (n = 6) had mesangial proliferation, 11.1% (n = 2) had glomerulosclerosis, 100% (n = 18) had glomerulomegaly, and there was absence of renal fibrosis in 94.4% (n = 17). Electron microscopy was performed in biopsies of 17 patients. The most relevant findings were effacement of the podocyte process in 100% (n = 15) of the patients and degeneration of microvilli in 80% (n = 12) of them (Table 3, Supplementary data 3).
Table 3 Histopathological characteristics by light and electron microscopy of kidney biopsies in the persistent albuminuria group
| Characteristic | n (%) |
|---|---|
| Number of glomeruli, med (IQR) | 16 (13-20) |
| Glomerular size µm, med (IQR) | 170 (163-177) |
| Mesangial proliferation | 6 (33.3) |
| Glomerulomegaly | 18 (100) |
| Glomerulosclerosis | 2 (11.1) |
| Fibrosis | |
| 0% | 17 (94.4) |
| 15% | 1 (5.5) |
| Prominence of podocytes | 4 (22.2) |
| Resorption proteins | 5 (27.7) |
| Tubulitis | 1 (5.5) |
| Electron microscopy | (n = 15) |
| Podocyte process effacement | 15 (100%) |
| Percentage of podocyte effacement, med (IQR) | 30 (30-35) |
| Microvillous degeneration | 12 (80) |
| Increase in podocyte organelles | 5 (33.3) |
Data shown in frequencies and percentages (n = 18 total). IQR: Interquartile range; med: median; n: number.
SerpinA3
The densitometric analysis corrected for urinary creatinine showed a statistically significant difference in urinary protein excretion between groups (p < 0.001). Protein expression was significantly higher in the positive control group than in negative controls (0.70 ng/mL vs. 0.08 ng/mL, p < 0.001), and in the iACR group (0.19 ng/mL, p = 0.005). Likewise, we found greater SerpinA3 urinary excretion in patients with pACR, a very different value than that found in the negative control group (0.08 vs. 0.25 ng/mL, p = 0.037) (Fig. 2A).

Figure 2 Biomarkers of tubulointerstitial injury. (A) Urinary excretion of SerpinA3 quantified by WB in each classification group, and corrected for urinary creatinine. Significant difference between the positive control and negative control groups (p < 0.001), positive control and isolated albuminuria (p = 0.005), and negative control and persistent albuminuria (p = 0.037). (B) Urinary excretion of HSP-72 quantified by WB in each classification group, and corrected for urinary creatinine. Significant difference between the negative control and positive controls (p = 0.027). Statistical analysis with the Kruskal-Wallis and the post hoc Dunn test. A p < 0.05 value was considered significant. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
HSP-72
We also observed an increase in urinary excretion of HSP72 in the positive control group when compared with the negative control group (1.4 vs. 0.2 ng/mL, p = 0.027). There was no significant difference between the pACR group and the negative control group (0.7 vs. 0.2 ng/mL, p = 0.477) (Fig. 2B).
PCX
Data analysis revealed variability in urinary PCX levels according to the group classification, as well as a statistically significant difference (p = 0.028) due to lower concentrations in the positive control group. Patients in the positive control groups excreted less urinary PCX than those in the iACR group (105.1 vs. 186.9 ng/mL, p = 0.017), but the difference between the negative controls and the pACR patients was not significant (152.5 vs. 162.0 ng/mL, p = 0.999) (Fig. 3A).
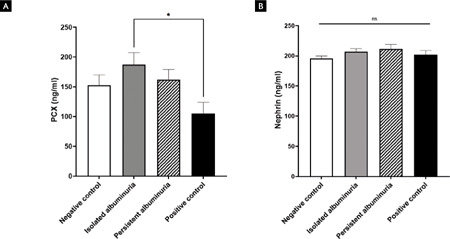
Figure 3 Biomarkers of podocyte injury. (A) Podocalyxin urinary levels quantified by sandwich ELISA in each classification group. Significant difference between the positive control group and the isolated albuminuria group (p = 0.017). (B) Urinary Nephrin levels quantified by sandwich ELISA in each classification group. No significant differences were found between groups (p = 0.432). Statistical analysis with ANOVA or Kruskal-Wallis test according to their distribution, and with post hoc Dunn or Tukey test. A value of p < 0.05 was considered significant. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
Nephrin
Finally, the urinary excretion of nephrin was no different between all study groups (p = 0.432) (Fig. 3B).
DISCUSSION
This study showed that SerpinA3 was the only possible biomarker associated with pA, while HSP-72, PCX, and nephrin were not significantly associated. The usefulness of a biomarker of kidney injury is directly related with the type of injury and the objectively injured area20. Therefore, it is important to take into account that the group of adolescent patients with pA was recruited in a region with a high prevalence of CKD of unknown origin; that is, the triggering factor remains to be elucidated. The histological characteristics suggest that oligonephrony may be the primary cause, a hypothesis that is supported by the observed glomerulomegaly, the decrease in kidney volume by ultrasound, the partial fusion of the podocyte processes, and the absence of fibrosis reported by Díaz et al.5 Oligonephrony may also be secondary to nephrogenesis abnormalities or to the loss of nephrons as a result of any post-natal pathological process. In this group of patients, the absence of fibrosis and inflammation suggests that its origin may be pre-natal.
Oligonephrony is a common finding in all nephropathies, and glomerular hyperfiltration is the pathogenic mechanism leading to kidney function impairment21. Structurally, this hyperfiltration is the result of disrupted vascular tone in afferent and efferent arterioles. Several factors, be they endocrine (renin-angiotensin system, aldosterone, and glucagon), vasoactive peptides (prostaglandins and vasopressin), and mediators of tubulo-glomerular feedback, are necessary to adequately maintain renal plasma flow and glomerular filtration22,23. Pharmacologic actions applied to this axis have proven to preserve and protect kidney function, mainly as a result, in a great measure, of a decrease in glomerular pressure24-27. Prematurity is the most studied process that can trigger congenital oligonephrony (not significant in Aguascalientes)5; it can lead to hyperfiltration, glomerulomegaly, albuminuria, and secondary focal and segmental glomerulosclerosis resulting in histologically evident CKD28. The follow-up of an adult patient cohort (mean age, 23.1 years) was recently reported: one group had a history of prematurity, and the authors studied their copeptin levels, plasma renin activity, and aldosterone concentration as possible glomerular hyperfiltration markers. Cases with a history of prematurity had decreased kidney volumes and increased albuminuria. Copeptin was the only marker that was significantly associated with this group of patients. Copeptin is a vasopressin surrogate and could also be a potential biomarker of hyperfiltration in these patients29.
There are very few reports on kidney injury markers in the early phases of kidney injury in which only microalbuminuria is detected. SerpinA3 has been associated with multiple physiopathological processes (e.g., inflammation and fibrosis)30. The role of SerpinA3u in this group of patients has not been studied. Although pA is a clear manifestation of chronicity, albumin excretion per se and the neuro-humoral mechanisms associated with glomerular hyperfiltration, promote inflammatory injury to podocytes21,31,32. In a murine focal and segmental glomerulosclerosis model, SerpinA1 and SerpinA3 were found to be overexpressed in the extracellular matrix, suggesting their possible physiopathogenic role in podocyte injury in this primary entity33. We also recently demonstrated that SerpinA3 relocates from the cytoplasm to the apical tubular membrane (ATM) in CKD, so it appears to be secreted into the luminal space in a physiopathological sense. We also showed that the expression and secretion of SerpinA3 increase in HEK-293 cells after transfection with a SerpinA3 clone tagged with FLAG and exposed to H2O2, or in cases of starvation34. These overall results suggest that the presence of SerpinA3 in urine reflects a physiopathological state that could, in turn, mirror incipient kidney injury.
Although our group reported no fibrosis in the kidney biopsies, the presence of uSerpinA3 may be a manifestation of this protein's role in glomerular hypertension. SerpinA3 has also been reported to play an important role in the renin-angiotensin-aldosterone system. One of the main functions of SerpinA3 is the regulation of inflammation by inhibiting cathepsin G in neutrophils, and mastocyte chymase in the kidney; it assumes a putative inhibitory function of the angiotensin-converting enzyme, thus precluding the conversion of angiotensin I to active angiotensin II. Surprisingly, increased levels of the angiotensin-converting enzyme have been detected in the serum of patients lacking this protein33,35. Regardless, the specific role of SerpinA3 in renal physiopathology remains unknown. We encourage investigators to continue in-depth research on this variable, for a more thorough understanding of this molecule and its potential applications30.
The main limitation of this study is its exploratory nature and the lack of a standardized quantification method to measure the biomarkers. Therefore, subsequent studies with complementary methods and more controlled patient's scenarios are necessary to clarify the potential role of the SerpinA3 protein expression quantification values that could represent an alternative diagnostic tool for early stages that may prevent irreversible kidney damage. At this moment, it is difficult to know whether the difference in SerpinA3 values between groups is sufficient for it to be used as a biomarker. This decreases its clinical applicability for now. It should be mentioned that we tested two different commercial ELISA kits to detect Serpin-A3; their sensitivity was low and there was great variability between tests, even when using the same sample.
The study's main strength lies on the fact that this is the first study searching for CKD biomarkers in this population. Although the nephropathy described in Aguascalientes has not been previously reported throughout the country, Mexico has a large disease burden due to CKD that may be explained by this newly described entity. It is therefore fundamental to create a national CKD registry and characterize its main etiologies, to establish whether the phenomenon that we have detected in Aguascalientes is local or has a nationwide presence.
We found that uSerpinA3 is a possible marker associated with pA in adolescents from Aguascalientes. The role of SerpinA3 as a mechanism of injury in this entity should be clarified in future studies, as well as its usefulness as a marker of incipient renal injury.

