











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
One of the most common arrhythmias associated with acute coronary syndrome (ACS) is new-onset atrial fibrillation (NOAF)1. In the context of ST-elevation myocardial infarction (STEMI), NOAF is observed in the range of 6-21%2. In individuals with STEMI, NOAF has been attributed to worse outcomes, including cerebrovascular accident, heart failure, as well as increased risk of short-term mortality3. Hence, identifying individuals with STEMI who are at high risk of developing atrial fibrillation (AF) are imperative.
Inflammation and oxidative stress have essential roles in the pathogenesis of AF4. Serum albumin, the most abundant protein in human serum, serves a number of physiological functions5. Decreased synthesis and increased catabolism of serum albumin have been related with an exacerbated inflammatory response6. Low serum albumin levels were also related with the development of AF and stroke7. Serum uric acid (UA), an end product of purine catabolism, on the other hand, increases the risk of atherosclerosis and plays a critical role in the formation of coronary artery disease (CAD)8. Furthermore, elevated serum UA levels are related to endothelial dysfunction and elevated inflammatory response9.
The uric acid/albumin ratio (UAR) is a novel index, which has recently been developed as a marker of inflammation and oxidative stress. The UAR has been demonstrated to have a good prognostic value in predicting STEMI patients’ clinical outcomes10. It has also been linked to the extent of CAD in ACS patients11. Furthermore, UAR has been shown to be a strong predictor of short-term mortality in patients with acute renal failure12. To the best of our knowledge, in the literature, there is a lack of studies supporting the association between UAR and the development of NOAF in STEMI patients treated with primary percutaneous coronary intervention (pPCI). In fact, we presumed that incorporating UA and albumin into a single index, defined as UAR, might better predict NOAF in STEMI patients than either UA or albumin. As the next step, we investigated the role of UAR in predicting the development of NOAF in individuals with STEMI treated through pPCI.
METHODS
STEMI was diagnosed by assessing symptoms and electrocardiographic data in accordance with the current guidelines’ recommendations for STEMI clinical definition13. We solely included consecutive STEMI patients treated with pPCI in this cross-sectional study conducted at a tertiary facility between January 2014 and January 2020. Patients with paroxysmal, persistent, long-standing persistent, or permanent AF, those on hemodialysis or with end-stage renal disease, those being treated for an active infection, with rheumatic and connective tissue disorders, those treated with inotrope treatment, and those with moderate-to-severe valvular heart disease were excluded from the analysis. Furthermore, patients with missing records were not included in the study. Medications recorded at the time of admission were evaluated for any influence on UA or serum albumin levels. None of the patients included in the study had gout, thyroid problems, or were on UA-lowering medication. The attending physician evaluated the patient’s clinical presentation, including heart rate and Killip class, at the time of admission. Each patient’s medical history regarding cardiovascular risk factors was obtained. The current investigation was designed in accordance with the Helsinki Declaration, and it was authorized by the Ethics Committee (decision no. = 2022/03-01).
An electrocardiogram was utilized to confirm AF if no P-waves, abnormal R-R intervals, or coarse or fine fibrillation waves were present for at least 30 s14. NOAF was defined as AF diagnosed after hospitalization in patients with no previous records of AF or atrial flutter. Blood samples were drawn from the antecubital vein before heparin administration or the commencement of the reperfusion process. All hematological measurements were made using an autoanalyzer. All of the patients’ plasma levels of creatinine, troponin I, triglycerides, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were measured using an automated chemistry analyzer. The serum UA and albumin concentrations were assessed using Roche Diagnostics Cobas 8000 c502 analyzer (Roche Holding AG, Basel, Switzerland) within 24 h following admission. The normal range for UA was 0-7.06 mg/dL, while the normal range for serum albumin was 3.5-5.2 g/dL. UAR was calculated by dividing serum UA (mg/dL) by serum albumin (g/dL).
Transthoracic echocardiography was completed between 12 and 24 h after admission to the hospital. The left ventricular (LV) ejection fraction was quantified after coronary intervention using a modified Simpson’s technique15. The left atrial volume index (LAVI) was calculated in the apical 4 and 2 chamber views at the end of systole using the biplane area-length approach indexed by body surface area16. All patients underwent coronary angiography using either the femoral or radial routes. Anticoagulant and antiplatelet medications were given in accordance with the current STEMI guideline recommendations.
Statistical analysis
R-software v. 4.0.2 (R statistical software, Institute for Statistics and Mathematics, Vienna, Austria) was used for all statistical analyses. The normality of distribution was assessed using the Kolmogorov–Smirnov test. The continuous variables with normal distribution were denoted as mean (SD), and variables with non-normal distribution were denoted as median (interquartile range). The categorical data were reported with the numbers and percentages. The χ2 test or Fisher’s exact test was used for comparison of categorical variables between the groups, as appropriate. The independent sample t-test or Mann–Whitney U-test was used for the comparisons of continuous variables. Univariable logistic regression analysis was used to detect the association of variables with the presence of NOAF. A multivariable logistic regression analysis was conducted with those variables detected as statistically significant in univariable logistic regression analysis. Firth’s penalized likelihood logistic regression was used for avoiding overfitting and overestimation in the multivariable model. For multicollinearity, variance inflation factor > 3 and tolerance (< 0.1) values were checked. Receiver operating characteristics (ROC) analysis was used to compare the discrimination abilities of variables for patients with and without NOAF. p < 0.05 was accepted as statistically significant for all analyses.
RESULTS
This analysis included 1484 STEMI patients, 69.6% of male and 31.4% of female. Following pPCI, 119 (8%) STEMI patients experienced NOAF. Table 1 depicts the baseline characteristics and past treatments of all participants based on the presence or absence of NOAF. The frequency of hypertension and diabetes was significantly different between individuals who had NOAF and those who did not. On admission, patients with NOAF had a higher Killip class status. Patients with NOAF showed a lower LV ejection fraction and a higher LAVI on echocardiography. Prior therapies, except for angiotensin-converting enzyme inhibitors/angiotensinogen receptor blockers (ACE inh/ARBs), were equivalent in NOAF and non-NOAF patients.
Table 1. Demographic, echocardiographic features and prior drugs of patients with and without new-onset AF
| New-onset AF (−), (n = 1365) | New-onset AF (+), (n = 119) | p value | |
|---|---|---|---|
| Age, years | 64.0 (56.0-71.0) |
68.0 (59.0-77.0) |
0.001 |
| Male gender, n (%) | 944 (69.2) |
90 (75.6) |
0.171 |
| BMI, kg/m2 | 28.3 (4.08) |
28.7 (3.33) |
0.225 |
| Risk factors | |||
| Hypertension, n (%) | 530 (38.8) |
69 (58.0) |
< 0.001 |
| Diabetes mellitus, n (%) | 282 (20.7) |
38 (31.9) |
0.006 |
| Previous CAD, n (%) |
581 (42.6) |
45 (37.8) |
0.363 |
| Family history of CAD, n (%) | 642 (47.0) |
62 (52.1) |
0.334 |
| Cigarette smoking, n (%) | 463 (33.9) |
50 (42.0) |
0.093 |
| On admission | |||
| Heart rate, min | 85.0 (78.0-95.0) |
88.0 (79.0-94.0) |
0.124 |
| Killip status > II, n (%) | 231 (16.9) |
38 (31.9) |
< 0.001 |
| Echocardiography data | |||
| LVEF, % | 45.7 (8.39) |
39.4 (4.96) |
< 0.001 |
| LAVI, mL/m2 | 26.5 (24.4-28.6) |
27.4 (25.6-29.5) |
0.001 |
| LVMI, g/m2 | 98.2 (23.8) |
103 (26.9) |
0.060 |
| Previous drug use, n (%) | |||
| Aspirin | 714 (52.3) |
54 (45.4) |
0.175 |
| Antiplatelet | 401 (29.4) |
29 (24.4) |
0.294 |
| Beta-blockers | 628 (46.0) |
64 (53.8) |
0.125 |
| Ca channel blockers | 208 (15.2) |
26 (21.8) |
0.077 |
| Statin | 215 (15.8) |
18 (15.1) |
0.961 |
| ACE inh/ARBs | 514 (37.7) |
64 (53.8) |
0.001 |
Continuous variables are presented as median (interquartile range) or mean (SD), nominal variables presented as frequency (%).
AF: atrial fibrillation; CAD: coronary artery disease; LVEF: left ventricle ejection fraction; LAVI: left atrial volume index; LVMI: left ventricle mass index; Ace inh/ARBs: angiotensinogen-converting enzyme/angiotensinogen receptor blockers.
Table 2 displays all participants’ laboratory results and angiographic findings. NOAF patients had higher white blood cell (WBC) counts, red cell distribution width, UA, C-reactive protein (CRP), and UAR levels than non-NOAF patients. Serum albumin and estimated glomerular filtration rate (eGFR) values were similarly lower in NOAF individuals. In terms of door-to-balloon time, infarct-related artery, Syntax score, and in-hospital mortality, there were significant differences between in NOAF and non-NOAF patients.
Table 2. Laboratory and angiographic results according to the development of new-onset AF
| New-onset AF (−), (n = 1365) | New-onset AF (+), (n = 119) | p value | |
|---|---|---|---|
| WBC count, ×103/µL | 8.90 (7.36-10.7) |
9.40 (8.00-11.2) |
0.004 |
| Hemoglobin, g/dL | 14.7 (13.6-15.6) |
14.8 (13.4-15.4) |
0.423 |
| Platelets, ×103/µL | 219 (182-253) |
222 (203-274) |
0.067 |
| Red cell distribution width, % | 43.7 (42.2-46.4) |
44.7 (44.0-46.4) |
0.007 |
| Mean platelet volume, fL | 10.0 (9.30-10.7) |
10.2 (9.50-10.5) |
0.087 |
| eGFR, mL/min/1.73 m2 | 88.8 (20.0) |
81.5 (18.0) |
< 0.001 |
| Triglyceride, mg/dL | 112 (98.0-168) |
124 (100-152) |
0.179 |
| LDL cholesterol, mg/dL | 110 (84.0-134) |
103 (84.0-154) |
0.322 |
| HDL cholesterol, mg/dL | 39.0 (33.0-43.0) |
40.0 (36.0-41.0) |
0.116 |
| Baseline troponin I | 12.0 (11.1-15.5) |
16.0 (10.3-18.0) |
0.213 |
| Serum uric acid, mg/dL | 4.60 (4.40-5.30) |
5.30 (4.50-5.50) |
< 0.001 |
| Albumin, g/dL | 3.88 (0.42) |
3.67 (0.48) |
< 0.001 |
| CRP, mg/dL | 4.32 (2.2) |
6.01 (2.23) |
< 0.001 |
| UAR | 1.23 (1.11-1.39) |
1.37 (1.27-1.61) |
< 0.001 |
| Infarct-related artery, n (%) | |||
| LAD | 655 (48.0) |
62 (52.1) |
|
| Cx | 333 (24.4) |
30 (25.2) |
0.677 |
| RCA | 364 (26.7) |
26 (21.8) |
|
| Others | 13 (0.95) |
1 (0.84) |
|
| Door-to-balloon time, min | 45.0 (35.0-60.0) |
55.0 (40.0-55.0) |
0.005 |
| Procedure, n (%) | |||
| Direct stenting | 244 (17.9) |
17 (14.3) |
|
| PTCA+stenting | 1109 (81.2) |
99 (83.2) |
0.133 |
| Only PTCA | 12 (0.88) |
3 (2.52) |
|
| IRA lesion length, mm | 25.0 (20.0-36.0) |
38.0 (30.0-40.0) |
< 0.001 |
| Syntax score | 15.8 (5.26) |
18.8 (4.91) |
< 0.001 |
| In-hospital mortality, n (%) | 55 (4.1) |
11 (9.3) |
0.016 |
Continuous variables are presented as median (interquartile range) or mean (SD), nominal variables presented as frequency (%).
AF: atrial fibrillation; WBC: white blood cell; eGFR: estimated glomerular filtration rate; LDL-C: low-density cholesterol; HDL-C: high-density cholesterol; CRP: C-reactive protein; UAR: uric acid/albumin ratio; Cx: circumflex coronary artery; LAD: left anterior descending artery; RCA: right coronary artery; IRA: infarct-related artery: PTCA: percutaneous transluminal coronary angioplasty.
Table 3 represents the findings of univariable and multivariable logistic regression analyses for predictors of NOAF. Using a univariable logistic regression model, age, diabetes, hypertension, LV ejection fraction, LAVI, ACE inh/ARBs, Killip Class >II, WBC, eGFR, CRP, door-to-balloon time, Syntax score, and UAR were identified as contributing factors for NOAF in STEMI patients. After incorporating these covariates into a multivariable logistic regression model, we noted that the UAR (OR: 6.951, 95% CI: 2.978-16.28, p < 0.001) remained an independent variable for NOAF in STEMI patients.
Table 3. Logistic regression analysis of variables for detecting new-onset AF
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p value | OR | 95% CI | p value | |
| Age | 1.030 | 1.012–1.049 | 0.001 | 1.021 | 1.001–1.042 | 0.041 |
| Diabetes mellitus | 1.802 | 1.188–2.689 | 0.005 | 2.149 | 1.320–3.474 | 0.002 |
| Hypertension | 2.174 | 1.490–3.192 | < 0.001 | 2.273 | 1.453–3.588 | < 0.001 |
| LVEF | 0.907 | 0.884–0.929 | < 0.001 | 0.902 | 0.874–0.929 | < 0.001 |
| LAVI | 1.118 | 1.049–1.194 | 0.001 | 1.073 | 0.99–1.158 | 0.071 |
| ACE inh/ARBs | 1.927 | 1.323–2.815 | 0.001 | 1.620 | 1.040–2.529 | 0.033 |
| Killip status >II | 2.303 | 1.514–3.449 | < 0.001 | 2.392 | 1.449–3.909 | 0.001 |
| WBC | 1.086 | 1.027–1.145 | 0.003 | 1.078 | 1.009–1.149 | 0.023 |
| eGFR | 0.981 | 0.972–0.993 | < 0.001 | 0.983 | 0.970–0.996 | 0.001 |
| UAR | 12.58 | 6.376–25.01 | < 0.001 | 6.951 | 2.978–16.28 | < 0.001 |
| CRP | 1.421 | 1.300–1.557 | < 0.001 | 1.460 | 1.317–1.626 | < 0.001 |
| Door-to-balloon time | 1.019 | 1.009–1.028 | < 0.001 | 1.014 | 1.003–1.025 | 0.013 |
| Syntax score | 1.112 | 1.073–1.153 | < 0.001 | 1.121 | 1.073–1.172 | < 0.001 |
OR: odds ratio; CI: confidence interval, AF: atrial fibrillation; LVEF: left ventricle ejection fraction; LAVI: left atrial volume index; Ace inh/ARBs: angiotensinogen-converting enzyme/angiotensinogen receptor blockers; WBC: white blood cell; eGFR: estimated glomerular filtration rate; UAR: uric acid/albumin ratio; CRP: C-reactive protein.
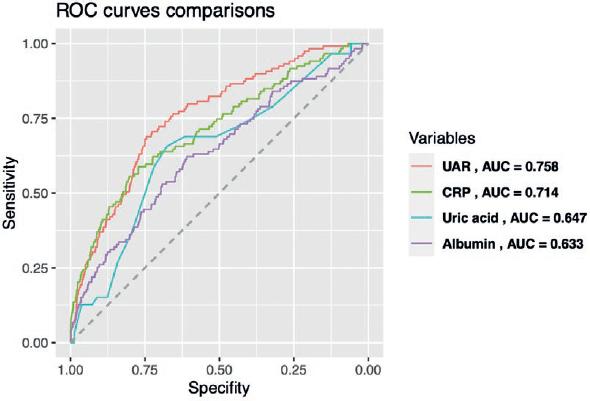
The area under curve (AUC) value of the UAR in a ROC assessment was 0.758 (Fig. 1). Remarkably, the AUC value of the UAR was greater than that of its constituents (albumin [AUC: 0.633] and UA [AUC: 0.647]) and CRP (AUC: 0.714). The recommended UAR value for predicting NOAF in STEMI patients was more than 1.39, with a sensitivity of 69% and a specificity of 74.5%.
DISCUSSION
This study indicated that after incorporating all possible covariates, the UAR was independently related with NOAF in STEMI patients. Despite major advancements in treatment modalities and PCI procedures, significant cardiovascular complications, such as NOAF, can develop during STEMI hospitalization. It is worth mentioning that the development of NOAF is related with a higher risk of in-hospital death in post-STEMI patients3,17,18. Similarly, in our analysis, we noticed that NOAF patients had higher in-hospital death rates than those who did not have NOAF. The etiology of NOAF in STEMI patients is complex, with particular mechanisms being unclear. According to the previous data, inflammation may have an influence on the development of AF. Notably, inflammatory changes have been discovered in atrial tissues collected from people with isolated/permanent AF19. In addition, serum CRP levels in individuals with paroxysmal and chronic AF were shown to be considerably higher than in controls20. Furthermore, elevated CRP levels have been known to increase the risk of NOAF in STEMI patients21,22. CRP was a predictor of NOAF in STEMI patients in our investigation, which was consistent with the literature. We did notice, however, that the AUC value of CRP was substantially lower than the AUC value of UAR.
The previous research attributed low albumin levels to the development of CAD and the risk of mortality from any cause23. There is further evidence that lower serum albumin values may be connected to the onset and progression of AF24. Hypoalbuminemia negative effects on anti-inflammatory and antioxidant activities may play a part in the pathophysiological process of AF7. On the other hand, in epidemiological studies, close connections between hyperuricemia and cardiovascular disease have been documented25. In individuals with cardiovascular disease, elevated UA levels are a major predictor of mortality26. According to a latest study, serum UA levels were connected to the severity of CAD, and it was a significant determinant of a high SYNTAX score27. An experimental investigation found that UA precipitated and generated monosodium urate crystals, causing local inflammatory responses. UA might also induce oxidative stress, inflammation, and endothelial dysfunction, all of which would have a role in the development and progression of AF28.
The UAR is an innovative biomarker that incorporates UA and albumin measurements to reflect the body’s overall inflammatory and oxidative status. This index has been proved to predict short-term mortality in individuals suffering from acute renal damage12. Furthermore, UAR predicted the severity of CAD better than the CRP-to-albumin ratio (CAR) in patients with non-ST-elevated myocardial infarction11. UAR has also been shown to be a predictor of death in STEMI patients, as well as a potential biomarker for identifying high-risk STEMI patients10. However, there is a lack of evidence in the literature on the potential role of UAR in predicting the development of NOAF following a STEMI event. In our analysis, the UAR was independently associated with NOAF development in STEMI patients after pPCI. It was also worth noting that the UAR’s AUC value was higher than that of UA or albumin alone.
We assume that our conclusions would be helpful in clinical practice. Because NOAF complications can be catastrophic, anticipating this adverse event is one of the top priorities in the care of STEMI patients. Because the UAR can be simply calculated with two commonly available laboratory parameters, it can be used at the bedside to identify efficiently STEMI patients who are at high risk for NOAF and to assist the implementation of prevention methods in such patients.
Our investigation has few limitations. First, the study’s retrospective methodology limits its capacity to establish exact causality between UAR and NOAF. Second, because the study is restricted to a single geographic location and only STEMI patients, extrapolating the findings to all ACS patients may be inappropriate. Thus, more research on other ACS presentations is required. Third, although multivariate analyses were carried out, residual covariates may still present. Fourth, the laboratory measures were derived only from blood samples collected within 24 h, which may have further decreased the precision of determining causality. Fifth, we did not have data regarding long-term outcome and prognosis of NOAF and non-NOAF STEMI patients. Finally, more prospective studies should be conducted in the future to confirm the findings of our analysis.
In conclusion, the present study indicated that the UAR was an independent predictor of NOAF development in STEMI patients. As an easily calculable laboratory index, the UAR can be utilized to predict NOAF in STEMI patients treated through pPCI.

