











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
The COVID-19 pandemic is one of the most important challenges for emergency medicine in this century. The initial lack of knowledge of this disease and its expression as a pandemic has led to the need for structural and management resources which were previously unknown in the emergency department (ED)1-6. A health alarm was generated by this new infection due to the elevated number of patients presenting pneumonia with acute respiratory distress syndrome (ARDS) requiring admission to intensive care units (ICUs) with invasive or non-invasive ventilatory support and carrying an elevated mortality. This context has made the presence of pneumonia by COVID-19 an area of uncertainty in the evaluation of risk in the ED and, consequently, has led to a high percentage of hospital admissions and never-before practiced situations in the ED7,8. Therefore, critical decisions in the ED must be made to ensure that patients with pneumonia can be safely discharged to avoid hospital overcrowding and collapse of the system. These decisions must be supported by scientific evidence to safeguard against inadequate discharges that result in bad clinical results. The data of large series collected in studies of patients with COVID-19 have reported some variables related to bad prognoses such as age, the presence of chronic comorbidities, an elevation of inflammatory parameters and D-dimer, and the presence of acute respiratory failure or lymphopenia, among others9-11. There are currently models for predicting severe manifestations and mortality from COVID-1912. However, at the time of the first wave of the pandemic, there was little clinical experience related to COVID-19 pneumonia that would allow emergency physicians to safely discharge patients without requiring hospital admission, and ED return visits were poorly studied13,14. Therefore, our objective was to study the variables associated with direct discharge of patients with COVID-19 from the ED and the safety of this decision in terms of mortality and ED revisits.
METHODS
Data from the UMC-19 project (Unusual Manifestations of COVID-19) were analyzed to conduct the present study. The UMC-19 project is a multicenter, observational study within a prospectively studied cohort carried out by the Spanish Investigators in Emergency Situations TeAm (SIESTA) research network15. This project has created a randomly selected control group of patients with COVID-19 recruited from 61 Spanish EDs participating in the project, which included from 10 to 30 patients each according to the reference population of the ED. The SIESTA cohort includes 1198 patients. The patient inclusion period was from March 1, 2020, to April 30, 2020. COVID-19 cases were defined as patients with a positive result in the reverse transcription-polymerase chain reaction test obtained from a nasopharyngeal swab at admission to the ED or from a second confirmation sample during hospitalization in the case of clinical suspicion.
A total of 43 variables were collected: two demographic (age and gender); 11 comorbidities (hypertension, dyslipidemia, diabetes mellitus, chronic obstructive pulmonary disease, coronary artery disease, clinically estimated obesity, cerebrovascular disease, chronic kidney disease, chronic heart failure, dementia, and active cancer); 16 symptoms and signs at ED arrival (lasting symptoms, fever, rhinorrhea, cough, expectoration, dyspnea, vomiting, diarrhea, anosmia, dysgeusia, temperature, systolic blood pressure, heart rate, respiratory rate, oxygen saturation by pulse oximetry, and fraction of inspired oxygen); 10 laboratory findings (C-reactive protein, creatinine, aspartate amino transferase, alanine amino transferase, ferritin, lactate dehydrogenase, leukocytes, lymphocytes, platelets, and D-dimer); and four chest X-rays data (interstitial infiltrates, opacities, pleural effusion, and cardiomegaly). For the study, only data of patients presenting with pneumonia in the chest X-rays defined by the presence of opacity or interstitial infiltrates were analyzed. In all cases, the review and description of the chest X-rays were carried out by the emergency physician responsible for the patient. The scores of the quick Sequential Organ Failure Assessment (qSOFA) and CRB-65 scales were calculated using the data collected. The patients were divided into two groups based on whether hospital admission or discharge directly from the ED was required, and associations between the two groups were studied. Afterward, we studied the variables associated with revisit to the ED related to COVID-19 within 30 days after discharge (EDR30d). The principal investigators (PIs) of each participating center reviewed the clinical histories of the EDs and hospitalization wards to obtain the study data. The final diagnosis of COVID-19 and the adverse events was collected locally by the PI of each center. Follow-up at 30 days was made by review of the electronic clinical histories of the patients.
The study was approved by the Ethics Committee in Clinical Research of the Hospital Clínic de Barcelona, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) (protocol HCB/2020/0534). In view of the urgent need of data collection, waiver of written informed consent was granted by the ethics committee. Patient information included in the database was encoded to ensure anonymity and patient confidentiality.
Statistical analysis
Categorical variables are expressed as absolute and relative frequencies, and continuous data are presented as means with standard deviation (SD) or, if not normally distributed, as median, and interquartile range. For comparisons, the Chi-square test was used for the qualitative variables (or the Fisher’s exact test in 2 × 2 tables when the expected values were <5), and Student’s t-test for independent measures was used for the quantitative variables, if the distribution did not affect the principle of normality (analyzed using Kolmogorov–Smirnov test) or using the non-parametric Mann–Whitney U-test if affected. The magnitude of association was expressed as a crude odds ratio (OR) with a 95% confidence interval (CI). A first analysis was performed to investigate the variables related to discharge directly from the ED. To investigate independent associations, adjusted ORs (aOR) were calculated; for this, variables that were statistically significant in the univariate analysis were introduced in the multivariate analysis. Taking into account, the large number of variables analyzed in the study and that many would foreseeably present statistically significant differences, the investigative team decided to perform multivariate analysis in two blocks (baseline related and acute episode related) to make a stable logistic regression model. We then performed a second analysis of the variables associated with EDR30d in the group discharged from the ED. For all analyses, differences were considered statistically significant when the p value was less than 0.05 or when the 95%CI of the OR excluded the value 1. The IBM SPSS Statistics V26 statistical program was used for the statistical analyses.
RESULTS
Of the 1168 patients recruited in the SIESTA cohort, at the time of analysis of the data, chest X-rays had not been performed in 25 cases (Fig. 1). Of the remaining 1143 patients, 859 (75.2%) presented with pneumonia and were included in the final study cohort. Of these, 84 patients (9.8%) were discharged directly from the ED. Table 1 shows the characteristics of the whole cohort and the variables associated with discharge from the ED. When comparing the basal characteristics of these patients with those requiring hospital admission, those discharged from the ED were younger, there was a greater proportion of women, and they presented fewer comorbidities. In relation to the characteristics of the acute episode, there was a lower presence of dyspnea, a higher presence of respiratory rate < 24 bpm, and O2 saturation > 92%. In regard to the analytical data of the group discharged from the ED, a greater proportion of patients presented C-reactive protein values of < 10 mg/L, creatinine < 1.2 mg/dL, ferritin < 300 ng/mL, lactate dehydrogenase < 240 IU/L, lymphocyte count > 1200 per mm3, and D-dimer < 1000 ng/mL. Chest X-rays showed a greater proportion of unilateral opacities. Figure 2 shows the estimation of the adjusted effect (ordered by the aOR value) of the different baseline and acute episode characteristics of the patients included in the multivariate model of the probability of hospital admission or discharge from the ED in patients with COVID-19 pneumonia. Discharge from the ED was associated with being a woman (aOR of 1.890; 95% CI 1.176-3.037), age < 60 years (aOR of 2.324; 95% CI 1.353-3.990), and lymphocyte count > 1200/mm3 (aOR of 4.667; 95% CI 1.045-20.839). A score ≥ 1 point in the qSOFA and CRB-65 scales was related to greater hospital admission.
Table 1. Characteristics of the study patients, according to hospital admission or ED discharge. Odds ratio calculated for ED discharge
| Total COVID-19 pneumonia (n = 859) | Hospital admission (n = 775) | ED discharge (n = 84) | p-value | OR (95%CI) | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age (years) (mean [SD]) | 64.4 (16.7) |
65.5 (16.5) |
54.8 (15.4) |
<0.001 | 1.039 (1.025-1.054) |
| Age < 60 years | 332 (38.6) |
277 (35.7) |
55 (65.5) |
<0.001 | 3.410 (2.124-5.473) |
| Female gender | 353 (41.1) |
306 (39.5) |
47 (56.0) |
0.004 | 1.947 (1.236-3.066) |
| Comorbidities (n [%]) | |||||
| Hypertension | 398 (46.3) |
377 (48.6) |
21 (25.0) |
<0.001 | 0.352 (0.211-0.588) |
| Dyslipidemia | 312 (36.3) |
290 (37.4) |
22 (26.2) |
0.042 | 0.593 (0.357-0.986) |
| Diabetes mellitus | 173 (20.1) |
165 (21.3) |
8 (9.5) |
0.011 | 0.389 (0.184-0.823) |
| Chronic obstructive pulmonary disease | 86 (10.0) |
84 (10.8) |
2 (2.4) |
0.014 | 0.201 (0.048-0.831) |
| Coronary artery disease | 70 (8.1) |
68 (8.8) |
2 (2.4) |
0.042 | 0.254 (0.061-0.999) |
| Obesity (clinically estimated) | 127 (14.8) |
121 (15.6) |
6 (7.1) |
0.038 | 0.416 (0.177-0.975) |
| Cerebrovascular disease | 54 (6.3) |
51 (6.6) |
3 (3.6) |
0.280 | |
| Chronic kidney disease | 65 (7.6) |
64 (8.3) |
1 (1.2) |
0.020 | 0.134 (0.018-0.977) |
| Chronic heart failure | 68 (7.9) |
68 (8.8) |
0 (0.0) |
0.005 | 0.894 (0.873-0.916) |
| Dementia | 69 (8.0) |
64 (8.3) |
5 (6.0) |
0.460 | |
| Active cancer | 86 (10.0) |
84 (10.8) |
2 (2.4) |
0.014 | 0.201 (0.048-0.831) |
| Symptoms at ED arrival [n (%)] | |||||
| Symptom onset (days) (mean [SD]) | 7.8 (5.6) |
7.7 (5.5) |
8.5 (6.5) |
0.302 | |
| Fever | 592 (68.9) |
541 (69.8) |
51 (60.7) |
0.087 | |
| Rhinorrhea | 90 (10.5) |
81 (10.5) |
9 (10.7) |
0.940 | |
| Cough | 511 (59.5) |
456 (58.8) |
55 (65.5) |
0.239 | |
| Expectoration | 139 (16.2) |
127 (16.4) |
12 (14.3) |
0.619 | |
| Dyspnea | 506 (58.9) |
466 (60.1) |
40 (47.6) |
0.027 | 0.603 (0.384-0.947) |
| Vomiting or diarrhea | 220 (25.6) |
196 (25.3) |
24 (28.6) |
0.513 | |
| Symptoms at ED arrival [n (%)] | |||||
| Anosmia | 59 (6.9) |
51 (6.6) |
8 (9.5) |
0.311 | |
| Dysgeusia | 62 (7.2) |
52 (6.7) |
10 (11.9) |
0.081 | |
| Signs at ED arrival (n [%]) | |||||
| Temperature (°C) (mean [SD]) | 36.9 (0.9) |
36.9 (1.0) |
36.7 (0.9) |
0.059 | |
| SBP (mmHg) (mean [SD]) | 128.8 (21.2) |
128.8 (21.7) |
129.5 (16.7) |
0.701 | |
| Heart rate (bpm) (mean [SD]) | 89.5 (17.1) |
89.2 (16.9) |
92.0 (19.7) |
0.159 | |
| Respiratory rate < 24 bpm | 621 (73.9) |
546 (72.0) |
75 (91.5) |
<0.001 | 4.160 (1.887-9.173) |
| Basal saturation O2 > 92% | 677 (78.8) |
600 (77.4) |
77 (91.7) |
0.002 | 3.208 (1.453-7.082) |
| Laboratory findings (n [%]) | |||||
| C-reactive protein < 10 mg/L | 549 (68.3) |
490 (66.8) |
59 (83.1) |
0.005 | 2.438 (1.286-4.622) |
| Creatinine < 1.2 mg/dL | 756 (90.3) |
681 (89.4) |
75 (100) |
0.003 | 1.110 (1.084-1.137) |
| AST < 40 IU/L | 395 (64.2) |
359 (63.8) |
36 (69.2) |
0.431 | |
| ALT < 40 IU/L | 516 (71.4) |
468 (71.0) |
48 (75.0) |
0.501 | |
| Ferritin < 300 ng/mL | 104 (27.7) |
93 (26.4) |
11 (47.8) |
0.026 | 2.553 (1.089-5.983) |
| LDH < 250 IU/L | 238 (34.9) |
206 (33.2) |
32 (52.5) |
0.003 | 2.218 (1.306-3.766) |
| Leukocyte count > 4000 per mm3 | 114 (13.5) |
108 (14.0) |
6 (8.0) |
0.145 | |
| Lymphocyte count > 1200 per mm3 | 301 (36.7) |
252 (33.6) |
49 (69.0) |
<0.001 | 4.402 (2.603-7.443) |
| Platelets > 150,000 per mm3 | 654 (77.7) |
590 (76.9) |
64 (85.3) |
0.095 | |
| D-dimer < 1000 ng/mL | 479 (67.9) |
422 (66.4) |
57 (82.6) |
0.006 | 2.409 (1.265-4.586) |
| Chest X-rays findings (n [%]) | |||||
| Interstitial lung infiltrates | 486 (56.6) |
445 (57.4) |
41 (48.8) |
0.130 | |
| Ground-glass lung opacities | 696 (81.0) |
630 (81.3) |
66 (78.6) |
0.546 | |
| Central | 93 (13.7) |
86 (14.0) |
7 (10.6) |
0.448 | |
| Chest X-rays findings (n [%]) | |||||
| Unilateral | 236 (33.9) |
197 (31.3) |
39 (59.1) |
<0.001 | 3.175 (1.890-5.334) |
| Pleural effusion | 34 (4.2) |
33 (4.5) |
1 (1.2) |
0.241 | |
| Cardiomegaly | 64 (7.9) |
60 (8.2) |
4 (4.9) |
0.301 | |
| Risk score (n [%]) | |||||
| qSOFA≥ 1 points | 309 (36.8) |
296 (39.1) |
13 (15.9) |
<0.001 | 0.294 (0.160-0.541) |
| CRB65 ≥ 1 points | 465 (55.4) |
440 (58.0) |
25 (30.5) |
<0.001 | 0.317 (0.194-0.518) |

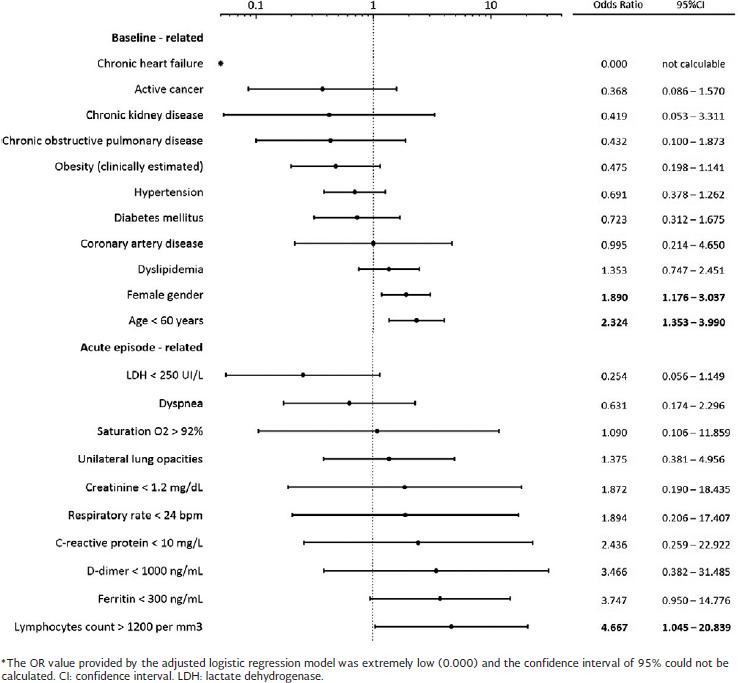
Figure 2. Estimation of the adjusted effect of the different baseline patient characteristics included in the multivariate model on the probability of admission or discharge from the ED in patients with COVID-19 pneumonia
Among the whole cohort, 132 patients died (15.4%), 130 from the hospitalized group (16.8%), and two in the group discharged from the ED (2.4%), with a crude OR of 0.121 (95%CI 0.029-0.498). In the latter group, a total of 30 patients (40.0%) revisited the ED, but only 6 (8.0%) required hospitalization. Table 2 shows the comparative analysis based on EDR30d. The only variable significantly associated with a lower EDR30d was being a woman, with an OR of 0.368 (95%CI 0.142-0.953).
Table 2. Characteristics of patients with pneumonia COVID-19 depending on revisit to the emergency department at 30 days (EDR30d) related to COVID-19
| Total COVID-19 pneumonia (n = 75) | COVID-19 pneumonia with EDR30d (n = 30) | COVID-19 pneumonia without EDR30d (n = 45) | p-value | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) (mean [SD]) | 54.8 (15.4) | 54.7 (13.7) | 54.1 (15.6) | 0.862 |
| Age < 60 years | 51 (68.0) | 22 (73.3) | 29 (64.4) | 0.419 |
| Female gender | 41 (54.7) | 12 (40.0) | 29 (64.4) | 0.037 |
| Other comorbidities | ||||
| Hypertension | 18 (24.0) | 7 (23.3) | 11 (24.4) | 0.912 |
| Dyslipidemia | 20 (26.7) | 6 (20.0) | 14 (31.1) | 0.286 |
| Diabetes mellitus | 8 (10.7) | 4 (13.3) | 4 (8.9) | 0.706 |
| Chronic obstructive pulmonary disease | 2 (2.7) | 1 (3.3) | 1 (2.2) | 1.000 |
| Coronary artery disease | 2 (2.7) | 1 (3.3) | 1 (2.2) | 1.000 |
| Obesity (clinically estimated) | 6 (8.0) | 2 (6.7) | 4 (8.9) | 1.000 |
| Cerebrovascular disease | 2 (2.7) | 1 (3.3) | 1 (2.2) | 1.000 |
| Chronic kidney disease | 1 (1.3) | 1 (3.3) | 0 (0.0) | 0.400 |
| Chronic heart failure | 0 (0.0) | - | - | - |
| Dementia | 4 (5.3) | 1 (3.3) | 3 (6.7) | 0.646 |
| Active cancer | 2 (2.7) | 2 (6.7) | 0 (0.0) | 0.157 |
| Symptoms at ED arrival | ||||
| Symptom duration (days) (mean [SD]) | 8.5 (6.5) | 9.1 (7,3) | 7.6 (5.7) | 0.327 |
| Fever | 45 (60.0) | 18 (60.0) | 27 (60.0) | 1.000 |
| Rhinorrhea | 9 (12.0) | 4 (13.3) | 5 (11.1) | 1.000 |
| Cough | 49 (65.3) | 22 (73.3) | 27 (60.0) | 0.235 |
| Expectoration | 12 (16.0) | 5 (16.7) | 7 (15.6) | 1.000 |
| Dyspnea | 37 (49.3) | 15 (50.0) | 22 (48.9) | 0.925 |
| Vomiting or diarrhea | 22 (29.3) | 10 (33.3) | 12 (26.7) | 0.534 |
| Anosmia | 8 (10.7) | 2 (6.7) | 6 (13.3) | 0.464 |
| Dysgeusia | 9 (12.0) | 2 (6.7) | 7 (15.6) | 0.301 |
| Signs at ED arrival | ||||
| Temperature (°C) (mean [SD]) | 36.7 (0.9) | 36.6 (0.9) | 36.7 (1.0) | 0.680 |
| SBP (mmHg) (mean [SD]) | 129.5 (16.7) | 129.5 (17.5) | 129.1 (16.6) | 0.917 |
| Signs at ED arrival | ||||
| Heart rate (bpm) (mean [SD]) | 92.0 (19.7) | 90.1 (16.5) | 94.8 (21.7) | 0.319 |
| Respiratory rate < 24 bpm | 66 (90.4) | 28 (93.3) | 38 (88.4) | 0.692 |
| Basal saturation O2 > 92% | 66 (88.0) | 27 (90.0) | 39 (86.7) | 0.733 |
| Laboratory findings [mean (SD)] | ||||
| C-reactive protein < 10 mg/L | 52 (81.3) | 23 (85.2) | 29 (78.4) | 0.491 |
| Creatinine < 1.2 mg/dL | 65 (95.6) | 25 (92.6) | 40 (97.6) | 0.558 |
| AST< 40 IU/L | 30 (66.7) | 13 (72.2) | 17 (63.0) | 0.519 |
| ALT< 40 IU/L | 43 (75.4) | 16 (66.7) | 27 (81.8) | 0.189 |
| Ferritin < 300 ng/mL | 11 (47.8) | 4 (36.4) | 7 (58.3) | 0.292 |
| LDH < 250 IU/L | 27 (49.1) | 12 (44.4) | 15 (53.6) | 0.498 |
| Leukocyte count > 4000 per mm3 | 65 (94.2) | 26 (92.9) | 39 (95.1) | 1.000 |
| Lymphocyte count > 1200 per mm3 | 45 (68.2) | 19 (67.9) | 26 (68.4) | 0.961 |
| Platelets > 150,000 per mm3 | 59 (86.8) | 24 (85.7) | 35 (87.5) | 1.000 |
| D-dimer < 1000 ng/mL | 52 (82.5) | 19 (76.0) | 33 (86.8) | 0.320 |
| Chest X-rays | ||||
| Interstitial lung infiltrates | 38 (50.7) | 19 (63.3) | 19 (42.2) | 0.073 |
| Ground-glass lung opacities | 57 (76.0) | 23 (76.7) | 34 (75.6) | 0.912 |
| Central | 5 (8.8) | 2 (8.7) | 3 (8.8) | 1.000 |
| Unilateral | 32 (56.1) | 11 (47.8) | 21 (61.8) | 0.298 |
| Pleural effusion | 1 (1.4) | 0 (0.0) | 1 (2.3) | 1.000 |
| Cardiomegaly | 4 (5.5) | 0 (0.0) | 4 (9.1) | 0.147 |
Ed: emergency department; OR: odds ratio; CI: confidence interval; SD: standard deviation; SBP: systolic blood pressure; AST: aspartate amino transferase; ALT: alanine amino transferase; LDH: lactate dehydrogenase; Hb: hemoglobin.
DISCUSSION
In our series, a significant proportion of patients with COVID-19 attending the ED presented with pneumonia and required hospital admission. Those discharged from the ED were more often women under the age of 60 with mild or no lymphopenia. However, the EDR30d was high but few patients needed hospitalization and mortality was low, and therefore, these discharges may be considered as safe. The COVID-19 pandemic is one of the greatest challenges that EDs have faced to date. In a situation in which the health-care system has bordered on the collapse, and health-care personnel have been exposed to a high risk of contagion and an unprecedented workload, emergency medicine physicians have been up against an unforeseeable situation. All of these circumstances have occurred within the context of a new, previously unknown infectious disease linked with an elevated need for hospital admission due to the presentation of severe, heterogeneous complications such as multiorgan dysfunction, ARDS, septic shock, disseminated intravascular coagulation, and thromboembolic events requiring ICU admission and with a high mortality8-12,16. For all these reasons, it is logical that our results reflect the high number of hospital admissions in patients with COVID-19 with pneumonia, even in patients who did not present criteria of severe pneumonia. Indeed, being a woman, being young, and the absence of lymphopenia were the only variables significantly associated with ED discharge. There are multiple tools for the evaluation of risk for bacterial pneumonia, including the Pneumonia Severity Index, CURB-65, and CRB-6517-19. These scales are very commonly used since they assess the risk of mortality of the episode and help in decision-making. However, differences between community-acquired pneumonia and COVID-19 pneumonia have been observed and may imply a different evolution of the disease. Based on indirect data, if it is taken into account that the mortality in our series was 15.4%, it can be said that mortality by COVID-19 pneumonia could be up to 50% higher than that of community-acquired pneumonia20,21. At present, different predictive models have been proposed for COVID-19 infection. However, many of these scales have limitations: highly variable clinical scoring performance, undetermined or high risk of bias, retrospective design, or performed early in the pandemic12.
The variables that emergency physicians have considered to be well related to safe decision-making have been few, but based on clinical judgment. Age is a variable widely related to worse outcomes in patients with SARS-CoV-2 infection. With an increase in age, the proportion of patients who evolve to more severe forms of infection and require ICU admission increases. A recent meta-analysis with 611,583 subjects shows that all age groups had significantly higher mortality compared to the immediately younger age group. The greatest increase in the risk of mortality was seen in patients aged 60-69 years compared with those aged 50-59. Advanced age is, therefore, one of the variables most clearly related to the need for hospitalization, and probably, the age of 60 is the optimal cut point in this decision together with the remaining clinical, analytical, and radiological criteria22. Males present more severe COVID-19 infection, with a greater need for hospital admission, admission to an ICU, and intubation23. The reason why men present more severe clinical forms is not clear, and in fact, this circumstance was also observed in infection by MERS-CoV and SARS-CoV24. It is likely that the clinical presentation in men is more severe and more often leads to the decision for hospital admission. The presence of lymphopenia is a common characteristic of this infection and has been related to more severe clinical forms with worse outcomes8-12,25. The reduction of total lymphocytes is also reflected by a reduction in its subsets, and therefore, CD4+ T cells, CD8+ T cells, B cells, and natural killer cells are reduced in patients with COVID-19. These lymphocytes and their subsets play an important role in the maintenance and function of the immune system, and their involvement indicates a deterioration of the immune system during the course of SARS-CoV-2 infection, which is common to other coronavirus infections such as MERS-CoV and SARS-CoV and indicates greater compromise and severity26,27. In our study, the absence of lymphopenia was a predictive variable in the decision-making for discharge from the ED. While physicians are not especially confident that this biological marker or indeed, any other analytical parameter or inflammatory marker is related to patient discharge from the ED, the absence of marked lymphopenia could certainly be associated with a less severe clinical presentation, and as such, is considered in the final decision. It is to be expected that unilateral radiological involvement would be associated with the decision for discharge from the ED. Although this association was important in the crude analysis, it was not confirmed in the adjusted analysis. Chest X-ray is one of the principal complementary studies of evaluation in COVID-19, although its sensitivity is variable based on the days of disease evolution28. Unilateral radiological involvement is more related to early phases of the disease and mild clinical pictures29. We found no significant differences in the duration of the symptoms, although there was a trend to fewer days of evolution among patients discharged from the ED.
An under-researched area is ED return visits in these patients. There are currently no prediction models for ED revisits in patients with COVID-19 infection. In our study, few patients were discharged and many presented EDR30d, although the need for hospital admission after EDR30d was low. One positive finding was that the decision for discharge from the ED was safe, considering the low mortality in this group. It is likely that the elevated EDR30d was due to the uncertainty and alarm generated by this infection among the population in general, together with a clinical picture which produces greater involvement in the general state of health, myalgias, and different symptomatology hard to control. It is difficult to predict the EDR30d in patients discharged from the ED, making further studies in this scenario necessary, along with the implementation of follow-up resources at ED discharge to reduce ED revisits30.
The main limitation of this study is that it was multicenter, with the inherent heterogeneity this represents in the availability of health-care resources not only at the level of the hospital itself but also in relation to alternatives to hospitalization. Nonetheless, this reflects the usual clinical practice in Spain, one of the countries with greater impact of the pandemic in relation to mortality in Europe. The use of chest X-rays for the diagnosis of COVID-19 pneumonia may have limited the number of patients with pulmonary involvement because of the limited sensitivity of the test, with chest computer tomography (CT) being much more effective in this sense. However, not all hospitals could perform CT in all the patients suspected of having pneumonia, and neither could it be performed in all the patients due to work overload during the peak of the pandemic. Therefore, we believe that our results closely approach the real-life health-care setting of the ED in our country. Likewise, the use of ultrasound might have helped improve the diagnosis of pneumonia, but similar to CT, not all EDs are able to perform lung ultrasound in all the patients attended. There may also be a limitation on the results in relation to the number of independent variables collected and the number of events. To minimize this possibility, the variables were grouped into blocks according to their characteristics.
Patients with COVID-19 pneumonia had an elevated rate of hospital admission. However, when the decision to discharge a patient from the ED was made, it was safe in terms of mortality but not for EDR30d.
SUPPLEMENTARY DATA
The complete members list of the SIESTA Research Group is available as supplementary material. Supplementary data are available at Revista de Investigación Clínica online (10.24875/RIC.22000021). These data are provided by the corresponding author and published online for the benefit of the reader. The contents of supplementary data are the sole responsibility of the authors.

