











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Depression and generalized anxiety disorder (GAD) are comorbid conditions frequently found in patients with rheumatic diseases. A recent study found a prevalence of 21.8% for depression and 37% for anxiety, in 514 Greek patients with rheumatic conditions1. Notably, depression and anxiety had not been previously diagnosed in most of these patients; therefore, they were not under medical treatment. Recognition of a mental health disorder is essential to receive adequate therapy, and it is estimated that only 50% of patients with depression are diagnosed2. In this regard, several factors may be responsible for the high frequency of undiagnosed depression and anxiety in patients with rheumatic diseases including a persistent social stigma surrounding mental illness (both among physicians and patients), poor communication between patients and physicians, and the limited time available in outpatient clinics to explore properly the existence of mental health disorders3. This has important implications in rheumatic patients since depression and anxiety have been associated with a poorer quality of life, higher disease activity, more pain, greater fatigue, worse outcomes, longer time to achieve remission, a decrease in response to treatment and in the likelihood of remission, increased costs, and increased mortality1,4,5.
Recently, the European League Against Rheumatism proposed several elements aimed to evaluate comorbidities in patients with rheumatic diseases, specifically considering depression as a comorbidity that should be examined using a simple question, without referring to any specific screening tool6. To improve the detection of mental health disorders, there are some self-administered tools that are quick and easy to complete, saving valuable consultation time. These instruments may also minimize social stigma and have been extensively validated to detect patients with clinical depression and anxiety. However, most of these tools have been developed in English-speaking countries, which create problems when used in regions with other languages and cultures. Spanish is the most widely spoken language in the world after Mandarin Chinese, and the number of speakers is rising; therefore, there is a need to apply these instruments in patients who speak a language other than English to evaluate whether transcultural adaptation certainly ensures that these instruments mean the same as in their original version7,8.
In this study, we sought to investigate the frequency of the symptoms of depression and anxiety in Mexican patients with rheumatic diseases, using self-administered questionnaires already adapted to the Spanish language, as well as to evaluate their usefulness in a real-world setting.
METHODS
Adult patients who attended our outpatient rheumatology clinic (a public tertiary care practice in a university setting) from March to June 2016 were invited to participate in this cross-sectional survey. Patients were asked to participate if they had an established diagnosis of a rheumatic disease. We excluded individuals who, in the investigators judgment, were unable to understand or answer the questions included in the questionnaires due to their educational level or lack of knowledge of the Spanish language. Each diagnosis was verified by attending physicians and only patients who met the current classification criteria for their respective rheumatic disease were included. A medical history was obtained, including demographic and clinical data with a special focus on the previous establishment of a psychiatric diagnosis. Socioeconomic status was obtained from the medical record; in our hospital, this represents a composite of the degree of education, family income, and occupation, and is routinely evaluated by a professional social worker. The family status was also obtained from the medical record and classified in a dichotomous way as married/living with a partner or not. In the understanding of the heterogeneity of rheumatic diseases included in the study and considering the wide diversity of therapeutic schemes and drugs used for each one, information related to treatment, functional ability, and disease activity was not collected. All participants were Mexican Mestizo (mixed European and Amerindian ancestry).
The study protocol and data collection were approved by the local ethics committee. All patients consented to provide their data for research purposes. All procedures were performed in accordance with the Declaration of Helsinki and local regulations.
Depression was assessed with the Spanish language version of the patient health questionnaire-9 (PHQ-9) test, which contains 9 items scored from 0 to 279. It also includes a question to assess whether depression symptoms are affecting functioning, a key criterion for establishing a diagnosis based on the Diagnostic and Statistical Manual of Mental Disorders (DSM)-5. This instrument is considered more accurate than other screening tools, with 88% sensitivity and 88% specificity10. Anxiety was evaluated with the 7-item GAD-7 scale, a questionnaire based on 7 items, which has also been validated in the Spanish language11. It is a useful tool with strong criterion validity to identify individuals with a possible GAD. In addition, the instrument is an excellent measure of disease severity, as demonstrated by the fact that increasing scores in GAD-7 scale are strongly associated with multiple domains of functional impairment and the number of disability days12. In this study, we used the Spanish language versions of PHQ-9 and GAD-7 originally translated in Spain, without making any cross-cultural adaptation9,11. It should be noted that these versions have already been used and validated in Latin American individuals13,14. All participants self-completed the PHQ-9 and GAD-7 formats in the waiting room of our rheumatology clinic.
PHQ-9 scores were classified as not elevated (score 0-4), mildly elevated (5-9), moderately elevated (10-14), or severely elevated (≥15), and these should be interpreted as representing no depression, mild, moderate, and severe levels of depression, respectively. The same cutoff points were used to measure the levels of GAD for GAD-7 test.
Statistical analysis
Continuous variables were expressed as means ± standard deviations or medians with interquartile range, while frequencies were used to describe discrete variables. Differences were assessed using the Students t-test or the Pearson Chi-square test with Yates correction, as corresponded. p < 0.05 value was set for statistical significance. Analyses were performed using GraphPad Prism version 7.00 for Windows, GraphPad Software, La Jolla, California, USA.
RESULTS
A total of 413 study subjects (341 women; 82.5%) were recruited. Table 1 shows a summary of the main clinical data. On average, patients included in this analysis were 50 years old, married or living with a partner, and had a low-to-medium socioeconomic level. The main rheumatic conditions were rheumatoid arthritis, systemic lupus erythematosus, fibromyalgia, and osteoarthritis.
Table 1 Main demographic and clinical characteristics of the study population.
| Study participants (n=413) | |
|---|---|
| Age in years, mean ± SD | 50.8 ± 16.2 |
| Female gender, n (%) | 341 (82.5) |
| Socioeconomic statusa | 396 |
| Low-income, n (%) | 352/396 (88.9) |
| Middle-income, n (%) | 38/396 (9.6) |
| High-income, n (%) | 6/396 (1.5) |
| Married or living with a partner, n (%)a | 279/371 (75.2) |
| Previous depression diagnosis, n (%) | 27 (6.5) |
| PHQ-9 scale, median score with IQR | 4 (2-8) |
| No depression, n (%) | 220 (53.2) |
| Mild depression symptoms, n (%) | 105 (25.4) |
| Moderate depression symptoms, n (%) | 56 (13.5) |
| Severe depression symptoms, n (%) | 32 (7.7) |
| Previous anxiety diagnosis, n (%) | 12 (2.9) |
| GAD-7 scale, median score with IQR | 3 (1-7) |
| No anxiety, n (%) | 245 (59.3) |
| Mild anxiety symptoms, n (%) | 100 (24.2) |
| Moderate anxiety symptoms, n (%) | 43 (10.4) |
| Severe anxiety symptoms, n (%) | 25 (6) |
SD: standard deviation, IQR: interquartile range.
aDue to missing data in medical records, participants may not add up to 413.
Overall, 57 (13.8%) patients did not score any point in any of the items of PHQ-9 questionnaire (PHQ-9 score = 0). In 193 (46.7%) patients, PHQ-9 scores were ≥ 5. We found PHQ-9 scores ≥ 10 (considered to be moderately to severely elevated) more frequently in women than in men (23% vs. 13%; p = 0.038). Interestingly, from a total of 88 (21.3%) subjects showing moderate and severe elevations of PHQ-9 scores (≥10 points), 27 (30.6%) had been previously diagnosed as having depression and only 4 (4.5%) were under therapy with antidepressants. Figure 1 shows a summary of the distribution and severity of depression symptoms according to PHQ-9 scale, by rheumatic condition. As noted, the highest frequencies of the severe elevations of PHQ-9 scale were observed in patients with osteoarthritis (20.2%), fibromyalgia (19.3%), Sjögrens syndrome (12%), and osteoporosis (10.2%).
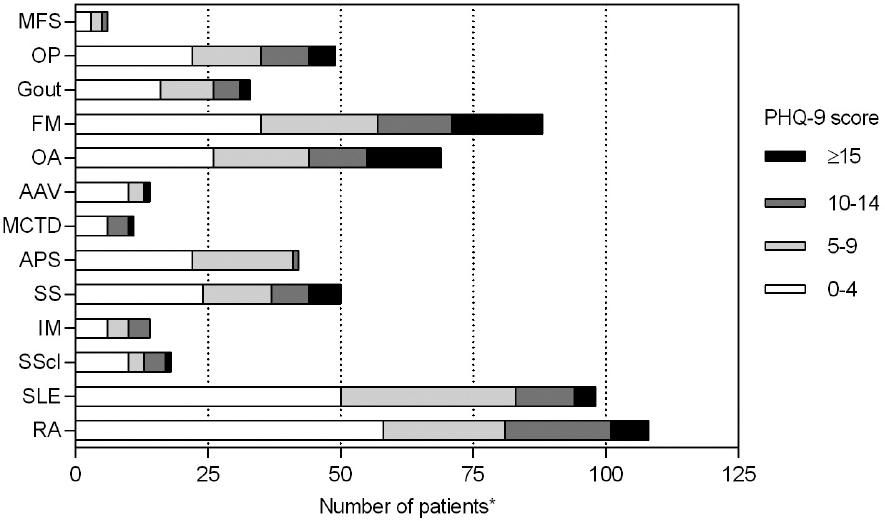
Figure 1 Frequency and severity of depression symptoms in 413 rheumatic patients according to the patient health questionnaire-9 scale. The bars represent the number of participants suffering from each rheumatic disease.
91 patients (22%) did not score any point in any of the items of GAD-7 questionnaire (GAD-7 score = 0). Generalized anxiety symptoms (GAD-7 score ≥ 5) were found in 168 (40.6%) subjects, 68 of them showing moderate-to-severe elevations of GAD-7 scores (≥ 10 points). Of these patients classified as having moderate or severe symptoms of anxiety, 12 (17.6%) were previously diagnosed as having GAD and only 4 (5.8%) were under medical treatment. Figure 2 shows a summary of the distribution and severity of anxiety symptoms according to GAD-7 scale, by rheumatic condition. As noted, the highest frequency of patients having severe elevations of GAD-7 score was found in patients with fibromyalgia (12.5%) and osteoarthritis (11.5%).
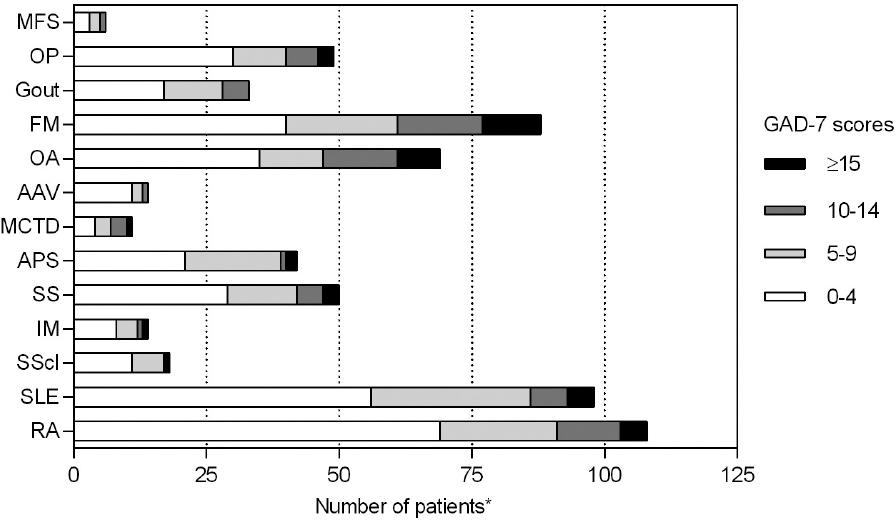
Figure 2 Frequency and severity of generalized anxiety symptoms in 413 rheumatic patients according to the generalized anxiety disorder-7 scale. The bars represent the number of participants suffering from each rheumatic disease.
An overlap of symptoms compatible with depression and generalized anxiety was observed in 90 patients with rheumatic conditions, which represents 21.7% of the study participants.
DISCUSSION
The findings of this cross-sectional survey suggest that self-administered screening tools are very useful and may help clinicians to suspect undiagnosed depression and/or GAD in patients suffering from rheumatic diseases. In addition, there was an unusually high rate of rheumatic patients with depression (46.7%) and anxiety (40.6%) symptoms; surprisingly, most patients had not been previously diagnosed with a mental illness despite receiving medical care regularly.
Depression is a major cause of ill health and disability worldwide, and, at worst, may lead to suicide. According to the latest estimates from the World Health Organization (WHO), more than 300 million people are now living with depression, which represents an increase of over 18% between 2005 and 201515. Moreover, an adequate recognition and diagnosis of depression and anxiety represent a major clinical challenge for physicians taking care of rheumatic patients, and previous studies have suggested that Latin American populations tend to have worse clinical outcomes regarding mental health disorders16. Results of the present survey are in line with studies already describing a high prevalence of depression and anxiety in rheumatic patients from other ethnicities; moreover, our findings were more than twice those found by Anyfanti et al. for depression (21.8%) and similar to those found by them for anxiety (37%) in Greek patients with various rheumatic diseases1. Previously, a study performed in 35 Mexican patients with rheumatoid arthritis found a 37% frequency of depression-related disorders, mainly major depression and dysthymia, using the beck depression inventory17. Recently, Matcham et al. conducted a systematic review and meta-analysis of 72 studies evaluating the prevalence of depression in rheumatoid arthritis12. They found a variation from 0.04% to 66.3%, and the meta-analytical pooled prevalence according to PHQ-9 scale was 38.8%, which is close to 46.2% prevalence found in our patients with rheumatoid arthritis, although they used a threshold of 10 points, indicating moderate-severe depression symptoms. In our patients with rheumatoid arthritis, the prevalence of moderate-to-severe symptoms of depression (PHQ-9 ≥ 10 points) was 25%.
Of interest, the results of a study including 43,845 Mexican female teachers who responded to PHQ-9 instrument have just been released18. This study revealed that 16% of participants had PHQ-9 score suggestive of severe depression; of them, < 5% had a formal diagnosis of depression and only 17% received antidepressants. Comparatively, of 341 female patients included in our study, 23% had PHQ-9 score compatible with severe depression (6.5% with a previous diagnosis of depression), and only 4.5% of them were in antidepressant treatment. Despite this, we should consider the possibility of an overestimation of depression symptoms in the subjects of our study since several of the questions included in the PHQ-9 questionnaire assess sleep and appetite disturbances, fatigue, psychomotor disorders, and concentration problems (see below), all of which are important issues in rheumatic patients.
Recently, the WHO launched a yearlong campaign Depression: lets talk on the understanding that overcoming the stigma frequently associated with depression will lead to more people getting help15. Following the WHOs campaign goals, our commitment as rheumatologists, often in the care of patients with undiagnosed depression or anxiety, should be to participate in this yearlong campaign and help to accomplish its main goal that patients with depression both seek and get help. In this regard, scales used in our study have been validated in several languages and have shown to correlate with the clinical diagnosis of depression and anxiety as well as to correlate with disease severity. On the one hand, PHQ-9 test assesses depression symptoms including anhedonia, depressed mood, insomnia or hypersomnia, fatigue, appetite and concentration disturbances, guilt, psychomotor alterations, and suicidal ideation. This instrument has been validated by classical test theory and item response theory models, and the Spanish version of PHQ-9 was shown to measure one underlying construct (i.e., depression) when used among Peruvian women13. The Spanish version of PHQ-9 has also been demonstrated to have good internal consistency in a large sample of Mexican women19. Notably, the ability of each item of PHQ-9 to capture one unique feature of depression has been shown to be independent of age, education attainment, and employment status13. On the other hand, GAD-7 questionnaire is a one-dimensional scale aimed at assessing the presence of anxiety symptoms referred in DSM-IV, and the Spanish language version has good reliability and cross-cultural validity to be used as a screening tool in Latin American individuals14. Finally, both PHQ-9 and GAD-7 instruments require a short time to be completed and may be applied by medical personnel free of charge. For instance, some studies have used the Zung Self-Rating Depression Scale for depression and the Hamilton anxiety scale for anxiety, both with more items to be answered by the patient, thus requiring more time to be completed (10-15 min, as compared to only 5-10 min for PHQ-9 and GAD-7 scales)1. Consequently, PHQ-9 and GAD-7 appear to be self-applied instruments useful for increasing the ability to detect depression and anxiety symptoms in clinically and culturally diverse settings.
The findings must be interpreted against the background of the limitations of this study. First, the cross-sectional nature of the survey does not allow us to evaluate the prognostic relevance of undiagnosed mental illnesses nor the sensitivity to change of self-administered screening tools. In the second place, there is a lack of confirmation of a diagnosis of depression or GAD by a mental health professional. Third, there is the absence of non-rheumatic patients as a control group; however, the overall prevalence of depression in Mexico has been estimated in 8%, 10.4% in women, and 5.4% in men20. Therefore, we can assume that our rheumatic patients have a higher frequency of depression symptoms than the general population. Finally, all participants were recruited from a single, tertiary care center, and results may not be extrapolated to a primary care setting.
Undiagnosed depression and GAD are very common in Mexican patients suffering from rheumatic diseases. Self-administered screening tools are very useful and may help clinicians to suspect depression and anxiety in rheumatology clinics for Spanish-speaking patients. The results of this study may help to change the misperception that depression and anxiety are inevitable and normal conditions in rheumatic patients. Patients and their caregivers, however, may have difficulties to deal with the increased burden of a newly diagnosed condition which will require the reconfiguration of existing service delivery models.

