










Serviços Personalizados
Journal
Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de investigación clínica
versão On-line ISSN 2564-8896versão impressa ISSN 0034-8376
Rev. invest. clín. vol.58 no.1 Ciudad de México Jan./Fev. 2006
Carta al editor
Use of non–absorbable polypropylene mesh for the treatment of spontaneous renal graft rupture
Uso de una malla no absorbible de polipropileno para el tratamiento de la ruptura espontánea de injerto renal
Luis Jorge Vales–Albertos,* Alfonso M. Cueto–Manzano,** Carlos Valdespino*** Benjamín Gómez*
* Department of Nephrology.
** Medical Research Unit in Clinical Epidemiology.
*** Transplantation Unit. UMAE Hospital de Especialidades, CMNO, de Guadalajara.
Correspondence and reprint request:
Luis Jorge Vales–Albertos
Department of Nephrology,
UMAE Hospital de Especialidades
Belisario Domínguez No. 1000 Col. Independencia Guadalajara, Jal.
Fax: (33) 3133–5090 Tel: (33) 1024–5622
E–mail: vales74@hotmail.com
Recibido el 7 de septiembre de 2005.
Aceptado el 25 de noviembre de 2005.
ABSTRACT
Renal graft rupture (RGR) is a life–threatening complication of kidney transplantation (KT), frequently associated with rejection and acute tubular necrosis. RGR repair with the use of suture, and corsetage with various materials (including synthetic glue, polyglactin absorbable hemostatic mesh, and lyophilized human dura), is indicated in non–severe cases. However, the employment of non–absorbable synthetic mesh had not been previously reported. Here, a case of a KT from cadaveric donor with RGR associated with acute rejection is reported. The graft was salvaged with the employment of a non–absorbable polypropylene mesh. Six months after KT, the patient remains asymptomatic with normal renal function. To the best of our knowledge, this is the first report of the use of a non–absorbable polypropylene mesh to repair a RGR. In a setting in which economical restrictions are important, the use of non–absorbable synthetic mesh may represent a good option of treatment.
Key words. Kidney transplant. Renal graft rupture. Polypropylene mesh.
RESUMEN
La ruptura del injerto renal (RIR) es una complicación del trasplante renal (TR) que amenaza la vida, y frecuentemente está asociada a rechazo y necrosis tubular aguda. La reparación de la RIR con el uso de sutura y ferulización con varios materiales (incluyendo pegamento sintético, mallas hemostáticas absorbibles de poliglactina y duramadre liofilizada humana) está indicada en los casos no graves. Sin embargo, el empleo de mallas no absorbibles no había sido informado previamente. Aquí se informa el caso de un TR proveniente de donador cadavérico con RIR asociada a rechazo agudo. El injerto fue rescatado con el empleo de una malla no absorbible de polipropileno. Seis meses después del TR el paciente se encuentra asintomático con función renal normal. Hasta donde tenemos conocimiento, éste es el primer informe del uso de una malla no absorbible de polipropileno para reparar una RIR. En un medio con importantes restricciones económicas, el uso de mallas sintéticas no absorbibles puede representar una buena opción de tratamiento.
Palabras clave. Trasplante renal. Ruptura del injerto renal. Malla de polipropileno.
CASE REPORT
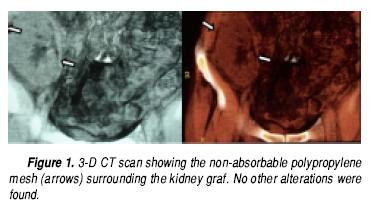
A 42–year–old male with end–stage renal disease of unknown origin received a kidney transplant (KT) from cadaveric donor in September/2004. No HLA compatibility test was performed, but negative cross–match was determined. He received induction with anti–CD25 (25 mg at days 0 and 4) and metilprednisolone (500 mg at day 0). Cold ischemia time was 15 hours. The graft was perfused with Eurocollins preservation solution. Eleven hours post–surgery, he presented abdominal pain, hypotension, hemoglobin decrease (5.7 g/dL) and oliguria. A perirenal hematoma (500 mL), found by ultrasonography and CT, was surgically evacuated; no vascular anastomosis alteration nor graft rupture were observed, and five red blood cell units were transfused. No biopsy was performed at this time. Four days after transplantation, increased resistance indexes were documented by Doppler ultrasound, and a control CT was normal. Hemodialysis was initiated because of delayed graft function. Patient was mobilized at the 5th day, and a 2–L spontaneous bleeding through the surgical drain tube required an emergency surgery, documenting a renal graft rupture (RGR) 5 cm length in the inferior pole, and a subcapsular hematoma (100 mL) in the convex border. Because the recipient was hemodynamically stable, RGR was filled with absorbable gelatin hemostatic gausses (S–99, Beijing Textile Research Institute, China); graft was subsequently wrapped with a polypropylene mesh (Polimesh–WL, World Lab, Guadalajara, Mexico), and externally compressed with gausses which were removed three days later (a direct biopsy was taken at this time). Daily methylprednisolone 250 mg were given empirically for three days. After the biopsy report of acute rejection Banff Ha, anti–thymocyte globulin 100 mg/ day was administered for three doses, leading to SCr of 2.2 mg/dL. Subsequently, anti–CD3 antibodies 2.5 mg/day were administered for four days, after which SCr was 1.2 mg/dL. The patient received mofetil mycophenolate, tacrolimus and prednisone as maintenance immunosuppression, and was discharged twenty–six days after KT. Six months after KT, he remains asymptomatic with SCr 0.9, creatinine clearance 90 mL/min/1.73 m2, and normal urinary sediment (Figure 1).
DISCUSSION
Spontaneous RGR is a life–threatening complication. Clinical presentation of the present case, as well as its association with acute rejection, are similar to others reported in literature.1–4 In concordance with others, the current case had a cadaveric donor and delayed graft function as additional risk factors.1–4
Nephrectomy is performed in presence of severe rejection, wound infection or hemorrhagic shock. In less severe cases, RGR repair is indicated with use of suture, and corsetage with various materials including synthetic glue, polyglactin absorbable hemostatic mesh, lyophilized human dura, and free graft of peritoneum.2
Non–absorbable synthetic meshes, especially those of polypropylene are mostly employed in the repair of incisional hernia.5 However, such non–absorbable polypropylene mesh had not been previously reported in the successful treatment of RGR. In a setting in which economical restrictions are important (as ours), the use of this kind of synthetic mesh may represent a good option of treatment (USD 627.00 absorbable us 290.00 non–absorbable).
REFERENCES
1. Hochleitner BW, Kafka R, Spechtenhauser B, Bosmäller C, Steurer W, Konigsrainer A, Margreiter R. Renal allograft rupture is associated with rejection or acute tubular necrosis, but not with renal thrombosis. Nephrol Dial Transplant 2001; 16: 124–7. [ Links ]
2. Chan YH, Wong KM, Lee KC, Li CS. Spontaneous renal allograft rupture attributed to acute tubular necrosis. Am J Kidney Dis 1999; 34: 355–8. [ Links ]
3. Finley DS, Roberts JP. Frequent salvage of ruptured renal allografts: a large single center experience. Clin Transplant 2003; 17: 126–9. [ Links ]
4. He B, Rao MM, Han X, Li X, Guan D, Gao J. Surgical repair of spontaneous renal allograft rupture: a new procedure. ANZ J Surg 2003; 73: 381–3. [ Links ]
5. Burger J, Luijendijk R, Hop W, Halm J, Verdaasdonk G, Jeekel J. Long–term follow–up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 2004; 240: 578–85. [ Links ]

