











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
In 1937, Meigs JV and Cass JW described seven patients with the typical triad of Meigs’ syndrome (MS) - a benign ovarian fibroma with ascites and hydrothorax.1-6 Worthy of note, pleural effusions and ascites should resolve after the tumor removal.1-6 Differential diagnosis of MS includes pseudo-MS and pseudo-pseudo MS.2,3,6 Pseudo-MS is characterized by pleural effusions and ascites associated with other benign or malignant pelvic tumors;2,6 whereas in pseudo-pseudo MS the cavitary effusions with high levels of CA 125 are related to systemic lupus erythematosus.3 Elevated levels of CA 125 are reported in cases of MS, pseudo-MS and pseudo-pseudo MS;2,3 however, this tumor marker is indicative of malignant ovarian cancer.7,8 Serous ovarian cancer is a main cause of cancer-related death in USA,7 and the pretreatment levels of CA 125 are related to survival in high grade serous ovarian cancer (HGSOC).8 A case of pseudo-MS associated with HGSOC is herein described; and the role of CA 125 levels and mechanisms of ascites and pleural effusions are commented.
Case report
A 64-year-old Brazilian woman was admitted on January 24th 2016 because of abdominal distension causing progressive breathlessness with two months of duration. She had noticed changes in her bowel function, with alternate constipation and diarrhea. Before admission, a chest radiography showed bilateral pleural effusion; and abdominal computed tomography revealed an extensive hypogastric mass with central areas of necrosis and involving adjacent small and large intestinal bowels. In addition, there was massive ascites, and infra diaphragmatic bilateral lymph node enlargement (Figure 1). On admission, she claimed abdominal pain and presented with tachycardia and dyspnea. Physical examination revealed BMI: 29 kg/m2, normal heart function, pleural effusion and ascites, absence of visceromegaly and of lymph node changes, or peripheral edema. Diagnostic thoracentesis and paracentesis were done with suspicion of Meigs’ syndrome. Pleural fluid was a transudate and malignant cells were not observed in pleural specimens, whereas ascites was clearly carcinomatous. Routine tests showed: hemoglobin 13.7 g/L, hematocrit 42.1%, leukocytes 5.18 × 109/L, platelets 476 × 109/L, urea 12.7 mg/dL, creatinine 0.6 mg/dL, AST 55.4 U/mL, ALT 37.5 U/mL, ESR 61/1ah, C-reactive protein 5 mg/dL; the rest of biochemistry was normal. Worthy of note was the elevated level of CA 125: 6,973.0 U/mL (reference: < 35 U/mL). Pulmonary computed tomography angiography ruled out lung thromboembolism, and showed bilateral pleural effusion. PET-CT scan detected hypermetabolic foci indicative of neoplastic involvement in the hypogastric mass, in abdominal and thoracic lymph nodes, and in the first left rib; in addition to smooth and nodular inspissation in some peritoneal and pleural locations. Exploratory laparotomy revealed a large hypogastric tumor (9.9 cm x 9.7 cm x 7.4 cm) without plans of cleavage, and omental caking that indicated peritoneal carcinomatosis. Histopathology findings from samples obtained of the peritoneum as well as of the tumor were consistent with the diagnosis of HGSOC (Figure 2). Immunohistochemistry: cytokeratins 40, 48, 50 and 50.6 kDa (AE1/AE3) positive; estrogen receptor (SP1) positive; PAX8, transcription factor of the family of gene-paired box [PAX] (MRQ50) positive; and product of oncogene Wilms Tumor 1 [WT-1] (6F-H2) positive. Additionally, the CDX2, intestinal transcription factor (EPR2764Y) and TTF-1, thyroid and lung transcription factor (clone 8G7G3/1) were all negative. The possibility of surgical approach was discarded. Therefore, patient was referred to outpatient Oncology care, and underwent chemotherapy with paclitaxel and carboplatin. It is worth noting that the patient’s general condition as well as ascites and hydrothorax had progressively improved on the course of chemotherapy. Therefore, the patient did not undergo further thoracentesis since her hospital discharge. Currently, approximately 10 months after beginning of specialized follow-up, no recurrence of ascites or significant pleural effusion was revealed by routine radiographic control (Figure 3).
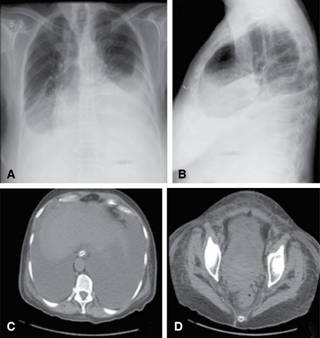
Figure 1: A and B: Chest radiograph showing accentuated bilateral pleural effusion; and abdominal CT revealing massive ascites (C); and voluminous hypogastric mass with areas of necrosis, bilaterally involving adjacent organs and local lymph nodes (D).
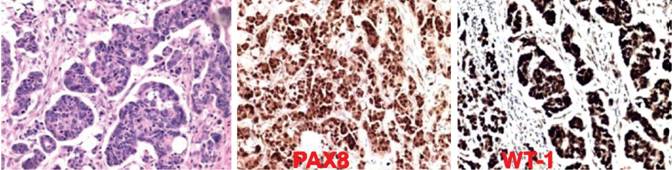
Figure 2: Immunohistochemistry evaluation strongly consistent with diagnosis of high-grade ovarian serous carcinoma, revealing the expressions of PAX8 and WT-1; the cytokeratins 40, 48, 50 and 50.6 kDa (AE1/AE3) and the estrogen receptor (SP1) were also found positive.

Discussion
Initially, the patient of the present case study had the diagnostic hypothesis of MS, but the diagnosis of pseudo-MS was confirmed with base on histopathology findings.1-6 The classical triad of MS specifically refers to a benign ovarian tumor associated with hydrothorax and ascites.1-6 Moreover, these cavity effusions should resolve after tumor removal;1-6 phenomenon not found in people with carcinomatous ascites.9 Although the ovarian tumors represent the fifth cause of death by cancer in women, they are the most lethal gynecologic malignancies in the US.10 The morphological and phenotypic patterns of this tumor include HGSOC and low-grade serous cancer, endometrioid, clear cell and mucinous carcinoma.10 Furthermore, the HGSOC may be genetically classified in the following molecular groups: immunoreactive, proliferative, differentiated, and mesenchymal.10 Useful protein markers are PAX8 and WT1.10 The main ovarian tumors related to MS are fibroma, thecoma, Brenner’s tumor, granulose cell tumor, and teratoma.4-6 Pseudo-MS is associated with other benign or malignant pelvic tumors, and pseudo pseudo-MS is due to systemic lupus erythematosus.2,3,6 The mechanisms of the elevated levels of CA 125 in patients with active systemic lupus are related to serositis, inflammatory phenomena involving proinflammatory cytokines, and the expression of this tumor marker by cells of the omentum and mesovarium.3 Histopathology data of biopsy samples showed peritoneal carcinomatosis in our patient. A major concern in the present case was the possibility of pseudo-MS due to metastases of digestive tract cancers with high levels of CA 125, as reported in two women with colon cancer (1,150.0 U/L)3 and omental caking by pancreatic cancer (465.0 U/L).9 Concerns about the origin of the pelvic mass were ruled out by immunohistochemistry confirmatory findings of pseudo-MS secondary to a HGSOC. Cytokeratins 40, 48, 50 and 50.6 kDa (AE1/AE3) and estrogen receptor (SP1) positive, and the expression of PAX8, and of WT-1 were consistent with ovarian etiology.10 Pretreatment levels of CA 125 higher than 500 U/ml in patients with HGSOC of FIGO stage III were found in association with enhanced survival rate.5 The woman herein reported presented with exceeding high blood level of CA 125 (6,973.0 U/mL); the presence of ascites and omental caking discarded possibilities of surgical approach. The antigen CA-125 is a glycoprotein that origins in the epithelium of fallopian tubes, endometrium, mesothelium of the pleura, peritoneum, and pericardium.6,7 High levels of this protein marker may be found in menstruation period, pregnancy, endometriosis, peritonitis, or liver cirrhosis.7 Finally, etiopathogeny of cavitary effusions both of MS and of pseudo-MS merit comments. The mechanisms of ascites and pleural effusion in Meigs’ syndrome are controversial.6-8 Hypotheses include passage of ascites through diaphragmatic foramens or lymphatics, and increased capillary permeability by VEGF or inflammatory cytokines.6-8 Whereas pleural transudates may be due to local changes in hydrostatic or oncotic pressures; exudative effusions often occur in MS, and are found in the vast majority of the pseudo-MS cases.6-8 Worthy of note, novel HGSOC cell models can reliably generate tumors and ascites,10 findings that may contribute to better understanding about these syndromes.
Conclusion
Ovarian cancers are among the major causes of death from malignant genital tract tumors, and the association with hydrothorax and ascites constitutes pseudo-Meigs’ syndrome. High levels of CA 125 do not discriminate benign from malignant abdominal conditions. Finding of PAX8 and WT1 increases the specificity and sensitivity of the ovarian cancer diagnosis. Classical MS is a benign condition that regresses after tumor removal, but the outcome of the pseudo-MS depends on the benign or malignant nature of the causes. Diagnostic criteria of both MS and pseudo-MS include the disappearance of effusions after the removal of the tumors. The option for surgery was discarded in the present case, but successful chemotherapy yielded similar result as an invasive extraction of the tumor bulk.

