











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Long bone diaphyseal fractures are responsible for prolonged periods of incapacity, work absenteeism and economical losses that may reach the millions due to their extended recovery period1. To reduce its socioeconomic impact, it is important to investigate methods that accelerate the bone consolidation process. The use of some biophysical methods, such as pulsed electromagnetic fields and low-intensity pulsed ultrasound (LIPU), has become a common therapeutic aid in Europe, Japan, and the United States in the past 20 years2-5. The LIPU is the only method approved by the Food and Drug Administration (FDA) to enhance the recovery process in distal radius fractures, type 1 exposed tibial diaphyseal fractures non-surgically treated as well as for non-union fractures (Approval Number P900009)6. However, the LIPU has not been applied for the bone healing process of tibial shaft fractures treated with an intramedullary nail as it has the drawbacks of implant overheating and high cost7.
Tanaka et al., 2003, accelerated 3.9 times the bone formation by simultaneously adding of noise (0.3 N, 1-50 Hz) to an axial load applied to the ulna which simulated the movement of walking in rats8. Besides, the increase in bone formation was not just the expected result of adding the effects of load and vibration; it was actually potentiated. However, these results were not replicated when noise was used without applying weight load. For this reason, these authors proposed the existence of the stochastic resonance (SR) phenomenon in the bone when applying load and noise simultaneously8. Based on this background, we generate the following hypothesis: the phenomenon of SR can be replicated in humans if we apply a noise stimulus coupled with the weight-bearing that the patient performs during walking to potentiate the osteogenic response.
Materials and methods
Ethical considerations
The present study was approved by the Bioethics and Investigation committees of the Centro Universitario de Ciencias de la Salud of the Universidad de Guadalajara and the Civil Hospital "Fray Antonio Alcalde." All patients signed the written informed consent form before admission to the study, between January 2010 and December 2011.
Study description
In this randomized clinical trial, 12 adult patients (two women and ten men) with recent tibial shaft fractures (< 30 days of evolution) were enrolled during a 24-month period. Participants were treated with closed and blocked intramedullary nails and randomized to two groups using sealed and consecutively numbered opaque envelopes: an experimental group (n = 6, weight-bearing plus noise stimulus) and a control group (n = 6, weight-bearing only). After removal of stitches, the patients underwent a rehabilitation program (RP) in two daily sessions of 20 min each. The RP was an outpatient period in which the participants walked using crutches or a walker and partial weight-bearing (15% of its own weight the 1st month) for 20 min (10 min of walking, followed by 5 min of rest and other 10 min of walking). The weight-bearing was duplicated in the 2nd month, and full weight-bearing was recommended in the 3rd month after the removal of the stitches. Simultaneously to the RP, the experimental group received a noise stimulus on the cutaneous surface of the fracture site with random intensities of 0.1-0.6 N and random frequencies of 0.1-50 Hz. The actors were placed directly on the surface of the skin just over the fracture site and turned it on during ambulation of the patient. Radiographic consolidation was evaluated by Radiographic Unión Scale of Tibia9. Patients with a diagnosis of diabetes mellitus, malnutrition, intestinal malabsorption, hepatic and/or renal insufficiency, nephrotic syndrome or any immunodeficiency, as well as patients who were receiving pharmacological therapy that could alter bone metabolism such as thiazolidinediones, bisphosphonates, calcium, and among other drugs, were excluded. In addition, patients with dementia or any disability that rendered them incapable of following orders, pregnant women or polyfractured patients were also excluded.
Devices description
Our working team designed the device used for the stimulus application which consists of two parts: a controller and a actor. The controller defines the vibratory wave's amplitude and force and the actor consists of two magnetic motors coupled permanently to an electric current to convert the energy into a mechanical signal. The device's intensity range and frequency were 0.1 a 0.6 N and 0.1-50 Hz, respectively. The device was programmed for randomly changing the intensity and frequency each 100 ms within the previously mentioned range.
Statistical analysis
The statistical analysis was carried out with IBM SPSS Statistics v. 17 (Armonk, NY, USA). All data were expressed as means ± standard deviations. The categorical variables were compared using Fisher's exact test. The numerical variables were assessed with Mann-Whitney U-test. The level of statistical significance was set at p < 0.05.
Results
Demographic variables
Demographic and surgical characteristics were similar for both experimental and control groups. Any variables showed no statistical difference (Table 1; p > 0.05).
Table 1 Demographic and surgical variables.
| Variable | Experimental group | Control group | p value |
|---|---|---|---|
| Age (mean±SD) | 23.2 ± 5.0 | 26.5 ± 8.5 | 1 |
| Gender (male:female) | 5:1 | 5:1 | 1 |
| Weight (mean±SD) | 61.8 ± 9.6 | 65.9 ± 13.6 | 0.63 |
| Injury mechanism (direct/indirect) | 3:3 | 4:2 | 1 |
| Affected leg (right to left) | 5:1 | 4:2 | 0.87 |
| Concomitant ipsilateral fibula fracture | 5 | 6 | 0.60 |
| Tibial fractures (Open: closed) | 3:3 | 2:4 | 0.89 |
| Closed and blocked intramedullary nailing | 6 | 6 | 1 |
Radiographical consolidation
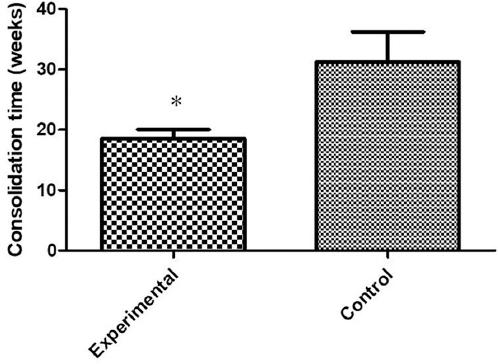
The required time for reach radiographical consolidation was better in the experimental group when compared to control group (p = 0.02). The progress of radiographical consolidation is shown in figure 1.
Functional recovery
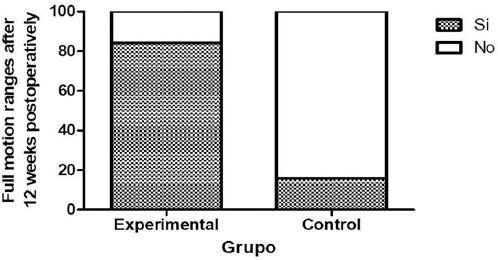
The recovery of mobility ranges in both knee and ankle was faster in the experimental group than in the control group after 12 post-operative weeks (Fig. 2).
Complications
There was no need to suspend the use of the experimental device due to discomfort in any of the patients. Few complications were presented among the subjects, which were satisfactorily resolved at the treatment's end. These happened in the experimental group and control group, respectively, as follows: gastrocnemius atrophy, 1 versus 0 patients (p = 0.29); wound dehiscence, 1 versus 0 patients (p = 0.29); hypoesthesia of the affected leg's 5th toe, 0 versus 1 patient (p = 0.29); hallux neurapraxia 0 versus 1 patient (p = 0.29), and delayed consolidation 0 versus 2 patients (p = 0.12). Consolidation delay was considered when recovery did not occur before the 26th week after surgery10.
Discussion
The present work assessed for 1st time the effect of applying simultaneous axial weight-bearing and noise vibration to accelerate the consolidation of tibial shaft fractures. Both groups were similar in demographic and anthropometric variables as well as in the trauma basic characteristics: lesion mechanism, affected leg, concomitant fibula fracture, and open fracture percentage.
The usual reported time for the clinical consolidation of tibial shaft fracture treated with closed and blocked intramedullary nail ranges from 16 to 30 weeks (112-210 days)11-14, and it depends on several factors such as age, severity of injury, fixation rigidity, and nutritional status15-17.
In the current study, the consolidation process in the control group lasted approximately 27 weeks (190 days), and two patients showed consolidation delay. This consolidation time is within the time range reported by other studies11-14. However, the frequency of consolidation delay in our study is higher than the one reported by Chalidis et al. 200913. The experimental group achieved consolidation almost 9 weeks earlier (60 days in total) and no patient was delayed in consolidation. Taking this into account, we can suggest that applying simultaneous noise vibration and weight-bearing accelerated the bone recovery process in adults with tibial shaft fracture managed with closed and blocked intramedullary nail. Although direct precedent of similar human therapies such as the one herein presented does not exist, Tanaka et al., 2003, demonstrated an important increase in bone formation in vivo when in healthy mice without ulna fracture, simultaneous axial load and noise vibration were applied. The increase in bone formation obtained was 4-fold as expected for the sole adding of load and vibration, suggesting that a SR phenomenon could occur when noise and load were applied at the same time8.
Previous studies using any physical method have demonstrated positive effects on bone consolidation6,18,19. Rubin et al., 2001, reported the use of LIPU to accelerate the healing of fractures which one was approved for the FDA in October 1994. Likewise, this method was approved for the FDA for treatment of established non-unions in February 20006. However, such results have been controversial20,21 and the need to research therapeutic alternatives to accelerate the consolidation of fractures persists.
This work represents an approximation to a new method to accelerate the bone consolidation process of lower extremity fractures. Furthermore, this method is promising for improving joint mobility, decreasing the frequency of delay in consolidation and does not produce any discomfort that obligates its discontinuation.

