











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkEtiology
The rabies virus belongs to the genus Lyssavirus, family Rhabdoviridae, and is bullet-shaped1.
Mr. Editor:
We present the case of a 13-year-old boy living in a rural area with poor hygiene and overcrowding. His illness began on April 3, while he was working in the field. He experienced paresthesias in both lower extremities, which progressed to the upper extremities, and urinary retention. He was evaluated on April 5; family members reported that last February. He had suffered injuries consistent with bat bites on his right toes.
Post-exposure rabies prophylaxis was initiated due to the severe risk of a bat bite with suspicious symptoms. Human rabies immunoglobulin (HRIG) and the first dose of human rabies vaccine were administered. The corresponding epidemiological study was carried out, and the health jurisdiction was notified.
The case was referred to the Eva Samano de Lopez Mateos Children’s Hospital in Morelia, Michoacan, on April 7, where his condition worsened with sialorrhea, confusion, vomiting, fever, photophobia, and respiratory distress with oxygen desaturation of 83%.
On April 8, 2024, at 11:35 a.m., the patient presented with cardiorespiratory failure, and resuscitation efforts were initiated. Death was declared at 11:50 a.m. On the same day, an autopsy was requested from the pathology service of the “Dr. Miguel Silva” Civil Hospital, where the brain was removed.
According to the epidemiological protocol, the Institute of Diagnosis and Epidemiological Reference requested a cerebral hemisphere to perform immunofluorescence tests. The right cerebral hemisphere and the left cerebellar hemisphere were analyzed in the pathology department of the “Dr. Miguel Silva” Civil Hospital (Fig. 1).
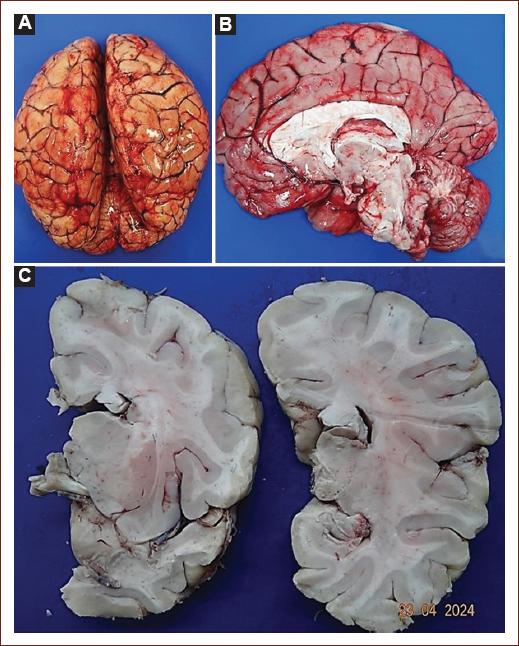
Figure 1 A: dorsal view of the brain. B: sagittal view of the brain; both show severe edema and congestion of the leptomeninges. C: coronal sections showed cortical congestion.
Eosinophilic inclusions were found in the cytoplasm of neuronal cell bodies in the midbrain, hippocampus, and cerebellum, as well as neuronal cell bodies with loss of nuclei (degenerated neurons), Virchow-Robbin spaces with perivascular lymphocytic infiltrate, known as “perivascular cuffs,” and neuropil edema (Fig. 2).
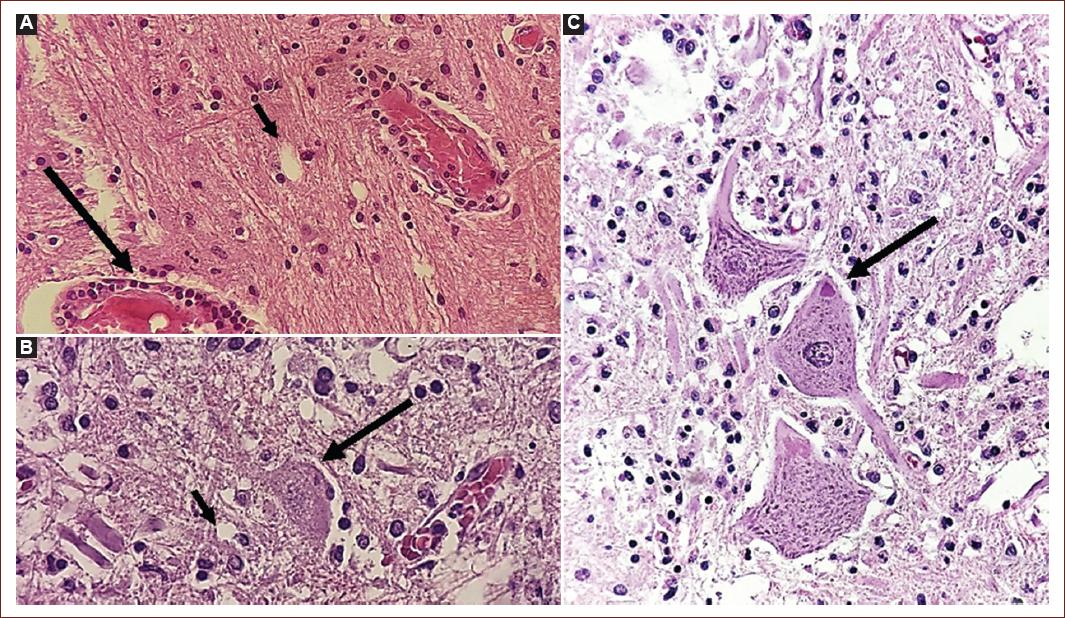
Figure 2 A: brain parenchyma with perivascular lymphocytic infiltrate (cuffs) (long arrow), and neuropil vacuolation (short arrow) in relation to edema. H&E, ×400. B: hippocampus section, degenerated neuron (long arrow), and intense neuropil vacuolation (short arrows). H&E, ×400. C: cerebellum, three Purkinje cells with different degrees of degeneration; the central neuron showed an eosinophilic cytoplasmic inclusion, Negri body (arrow).
These histological findings confirmed the diagnosis of rabies meningoencephalitis.
Discussion
In 2019, the World Health Organization awarded Mexico the certificate of the first country free of human rabies, transmitted by dog bites; However, this has created confusion, creating a false sense of rabies “eradication,” while ignoring the consequences of infection through other vectors, such as bat bites.
Rabies virus is the most important virus in the genus Lyssavirus because, from a global perspective, its distribution, human cases (> 55,000 deaths/year), wide range of potential reservoirs, and veterinary and economic cost implications make it the most important viral zoonosis. Rabies is thought to have occurred in tropical America since pre-Hispanic times, being transmitted predominantly by hematophagous vampire bats, although recent phylogenetic reconstructions suggest that the rabies virus in the Americas is unlikely to have originated from vampire bats1.
The vampire bat (Desmodus rotundus) is both host and vector of the rabies virus. In contrast, the other two hematophagous species (Diphylla ecaudata and Diaemus youngii) are not considered important transmitters of the virus. It is important to mention that cases of rabies in non-hematophagous bat species in Mexico are very rare, and do not represent a risk of transmission to humans1.
Diagnostic
To confirm the diagnosis of human rabies meningoencephalitis, premortem (in life) or postmortem can be performed2.
Corneal
A slide is firmly pressed against the central part of the cornea and repeated twice in each eye. The slides are fixed in acetone. This test is insensitive and sometimes traumatic2.
Saliva
Collect saliva from the floor of the mouth using a dropper or syringe and place it into a screw-capped test tube containing 2 mL of saline solution. Send the sample immediately to the laboratory and store it at a temperature of 4-8 °C. Saliva inducers should not be used, as they may interfere with viral replication2.
Skin biopsy
A skin sample measuring 10 mm in diameter is taken from the nape of the neck, at the level of the hairline, including the dermis (hair follicles). It is placed in a test tube (with a screw cap) containing 2 mL of saline or 50% glycerol in saline. It is identified, packaged, and kept refrigerated2.
Serum and cerebrospinal fluid (CSF)
They are obtained 10 days after the onset of neurological symptoms. Detection of antibodies in serum is only useful in unvaccinated patients; this limitation does not apply to CSF. The required amount for each sample is 2 mL. This test is less sensitive than others, as in a minority of cases it may show the typical changes of viral meningoencephalitis2.
Postmortem diagnosis
It is performed by extracting the brain and taking a sample to look for Negri bodies, lymphocytic infiltration in Virchow-Robin spaces, eosinophilic degeneration of the cytoplasm, and nuclear effacement2.
Immunofluorescence
It is based on the detection of antigens for the rabies virus, and is the gold standard2.
Differerntial diagnosis
The diagnosis of human rabies is usually suggested by epidemiologic and clinical findings and confirmed in the laboratory. The diagnosis is not difficult if there is a history of animal bite exposure and if a full spectrum of symptoms and signs has appeared. Otherwise, careful but rapid assessment of the epidemiologic and clinical features of less typical cases is essential before special laboratory tests are performed. Every patient with neurologic signs or symptoms or unexplained encephalitis should be questioned about the possibility of animal exposure in a rabies-endemic area inside or outside the country of residence3.
Early in the course of illness, rabies can mimic numerous infectious and non-infectious diseases. Many other encephalitides, such as those caused by herpesviruses and arboviruses, resemble rabies. Other infectious diseases also may resemble rabies, such as tetanus, cerebral malaria, rickettsial diseases, and typhoid. Paralytic infectious illnesses that may be confused with rabies include poliomyelitis, botulism, and simian herpes type B encephalitis3.
Non-infectious diseases that may be confused with rabies encompass a number of neurologic syndromes, especially acute inflammatory polyneuropathy (Guillain-Barré syndrome), as well as allergic post-vaccinal encephalomyelitis secondary to vaccination with nervous-tissue rabies vaccines, intoxication with poisons or drugs, withdrawal from alcohol, acute porphyria, and rabies hysteria. Guillain-Barré syndrome may be mistaken for the paralytic form of rabies, and vice versa3.
Post-exposure prophylaxis
All persons exposed to rabies should start by thoroughly washing and cleaning out the wound with soap and water or a virucidal agent. This should be followed immediately by passive rabies immunization with rabies immune globulin (RIG) in unvaccinated patients and vaccination with a cell culture rabies vaccine4.
Equine rabies immunoglobulin may also be used as an alternative if HRIG is not available4.
Unvaccinated individuals should receive four 1-mL dose vaccines and RIG promptly after being exposed to the rabies virus4.
The first dose of the vaccine should be administered as soon as possible after the exposure, on what is considered day 0. It can also be started weeks to months after exposure within the incubation period if signs and symptoms of rabies have not yet appeared. The next three doses should then be administered on days 3, 7, and 14 after the first vaccination4.
In our case, the consequences of the bat bite were not known, so medical attention was sought only when the patient already presented irreversible clinical symptoms. Due to the late complexity of the symptoms, no prior premortem diagnosis was performed.
The diagnosis was confirmed postmortem by immunofluorescence in the brain and histologically with brain sections.
Conclusion
The case of a 13-year-old boy who developed rapid encephalomyelitis of approximately 6 weeks duration is presented. He was not treated in time because he did not receive medical attention; therefore, the diagnosis was not timely. In this case, the prolonged progression is notable, as the fatality rate of the disease is typically within the 1st week after the bite.
In 2019, Mexico was certified as the first country in the world to eliminate human rabies transmitted by dog bites. However, the cases reported in recent years have been caused by bat bites.
The population should be advised on how to act when there is certain or suspected evidence of a bite from a rabies carrier, and how to take the necessary health measures, because the window of opportunity is very short and is essential for a good prognosis, as the outcome is often fatal.

