











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
In cor triatriatum dexter (CTD), the right valve of the sinus venosus fails to regress, thus separating the right atrium (RA) into two chambers. It represents 0.4% of congenital heart diseases (CHD) in autopsy series and < 0.1% of clinically diagnosed CHD1.
The clinical presentation depends on the degree of chamber separation and flow obstruction. In neonates, the presence of an atrial septal defect (ASD) may lead to cyanosis due to a right-to-left shunt2-4.
This case is significant because it highlights an exceptionally rare diagnosis during the neonatal period. In this scenario, desaturation serves as the primary clinical concern despite the absence of respiratory distress or hemodynamic repercussions. Notably, only a limited number of cases have been documented in the medical literature.
Clinical case
A 7-day-old full-term male newborn was referred to our clinic because of cyanosis and tachypnea associated with feeding and crying, with SpO2 falling as low as 70% during crises. The baby was born by cesarean delivery at 39 weeks of gestation, with good respiratory effort but persistent desaturation of 79% associated with feeding. A cardiology specialist’s opinion was not required, and the baby was discharged home with oxygen.
During the 1st week of life, he presented with tachypnea and desaturation associated with feeding but no fever or hemodynamic instability; therefore, he was referred to our department. We received him in the clinic on day 7 of life, with mild central cyanosis, normal pulse, liver to the right, no heart murmurs, tachypnea during breastfeeding, and no clinical signs of cardiac failure; weight 3.3 kg, height 51.5 cm, blood pressure 90/60 mmHg, heart rate (HR) 125 bpm, SpO2 78%, which increased to 89% after supplemental oxygen (FiO2: 25%).
There was no relevant medical family or psycho-social history.
An electrocardiogram showed a normal sinus rhythm, HR 125 bpm, and no arrhythmia.
Chest X-ray was normal, with no cardiomegaly or abnormal pulmonary overflow.
An echocardiogram showed normal drainage of pulmonary veins, with a membrane in the roof separating the RA into two cavities, the small upper cavity connecting to the left atrium through the patent foramen ovale (Fig. 1). This explained the right-to-left shunt and cyanosis. A diagnosis of ASD and complete CTD was made.
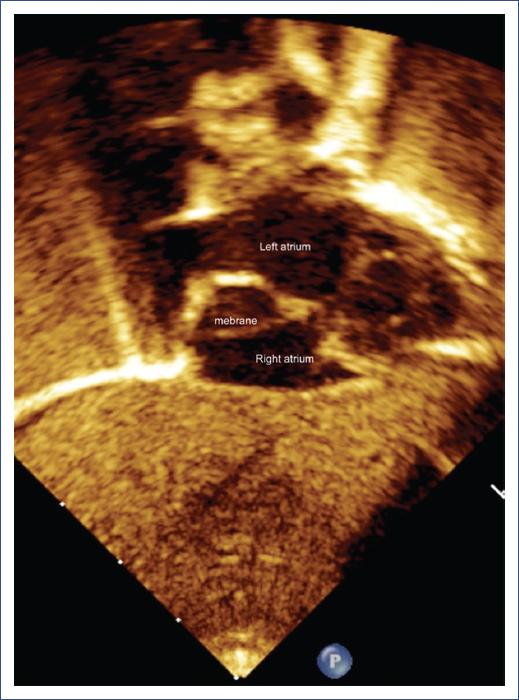
Figure 1 Echocardiography, subcostal view. The arrow shows the membrane (Cor triatriatum dexter) inside the right atrium.
Cardiac magnetic resonance imaging (MRI) revealed a complete CTD with an ASD and concordant atrioventricular and ventriculoarterial connections (Fig. 2).

Figure 2 Cardiac magnetic resonance imaging, sagittal plane, showing a membrane (white arrow) in the right atrium.
Cardiac surgery confirmed the pre-operative diagnosis of complete CTD by the presence of a membrane that separated the RA into two cavities. The membrane was removed, and the patent foramen ovale was closed.
Discussion
CTD is a rare CHD characterized by the presence of a membrane that separates the RA into two cavities. This membrane represents the persistence of the venous sinus, causing alterations in venous flow as it passes through the RA, potentially causing a shunt from right to left through defects in the interatrial septum and manifesting clinically with desaturation and cyanosis3,5.
CTD has varying clinical manifestations, depending on the degree of septation of the RA. The symptoms could range from desaturation with mild cyanosis, as in our case, to arrhythmias (supraventricular tachycardias), right-sided heart failure, or obstruction of the tricuspid valve or the right ventricle outflow tract. It is important to alert the pediatrician to immediately request a cardiology evaluation to rule out other severe structural heart diseases such as transposition of the great arteries, pulmonary atresia, or anomalous connection of pulmonary veins2,6,7.
The presence of cyanosis was explained by the ASD, which allowed a right-to-left shunt. As part of the pre-surgical approach, we decided to perform a cardiac MRI to assess the membrane and pulmonary vein anatomy, as recommended in some medical literature8,9.
During the surgical procedure, the membrane was identified, resected, and the foramen ovale closed. The patient’s post-operative course was very good, with a complete resolution of symptoms.
Conclusion
The importance of our case lies in the early identification of rare heart disease as a cause of cyanosis and desaturation in a neonate in the first days of life who did not present signs of heart failure. We recommend that all primary care physicians and pediatricians request a cardiology consultation when detecting any clinical signs of CHD, such as cyanosis, desaturation, tachypnea, increased respiratory effort, murmurs, or hepatomegaly. A simple test, like an echocardiogram, allows for timely diagnosis and treatment of CHD, preventing future complications and increased mortality.

