











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 65-year-old man with a history of recent non-reperfused myocardial infarction presented to the emergency department due to 3-day progressive dyspnea during mild physical activity (functional class III) and chest pain, which later required myocardial revascularization. Transthoracic echocardiogram revealed a left ventricular ejection fraction (LVEF) of 38%.
Perfusion study exhibited a transmural infarction of the apex and apical third of the left ventricular anterior wall that extended as non-transmural to the other segments of the anterior and septal walls, and no ischemia was found; the FDG metabolism study showed moderate uptake in the anterior wall suggestive of hibernating myocardium (Fig. 1).
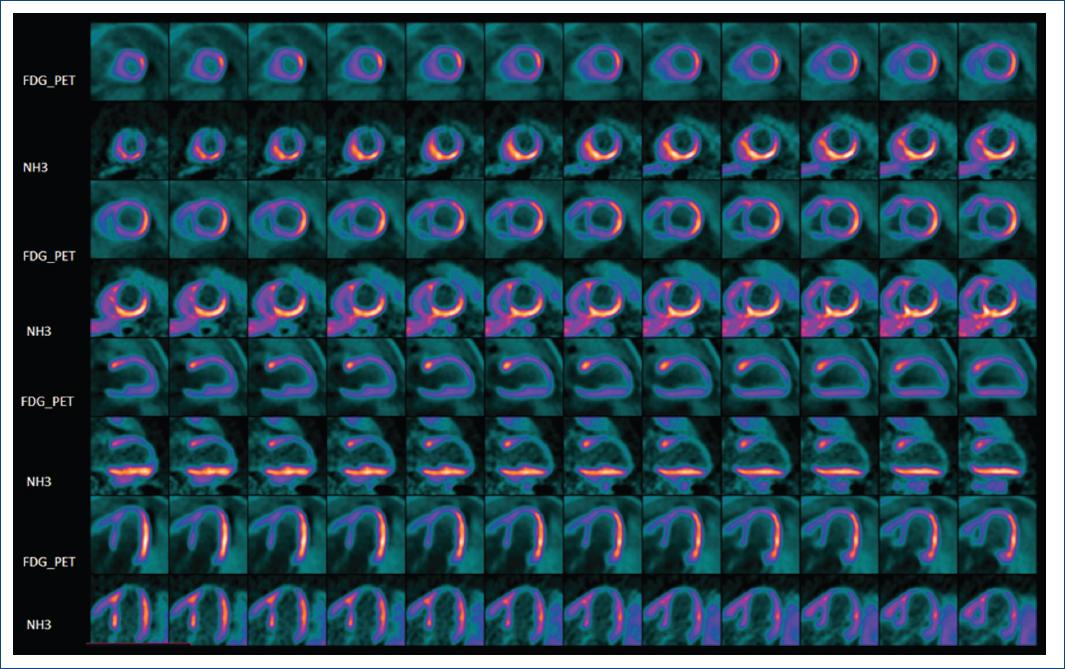
Figure 1 Positron emission tomography-fluorodeoxyglucose (FDG) viability. A moderate FDG uptake in the basal and middle thirds, with reduced uptake toward the more apical segments and the apex is visualized.
Calculated mismatch was approximately 10%. A significant reduction in coronary flow capacity (CFC: On the basis of a scatter plot of CFR vs. absolute stress flow) is observed in the apex, with an area with decreased FDG uptake, and a moderately reduced CFC in the rest of the anterior wall (Fig. 2). Absolute myocardial blood flow (MBF) analysis showed a positive result with a value of 110.21 ml/100 ml/min, while relative MBF analysis showed a negative result with a ratio of 0.71.
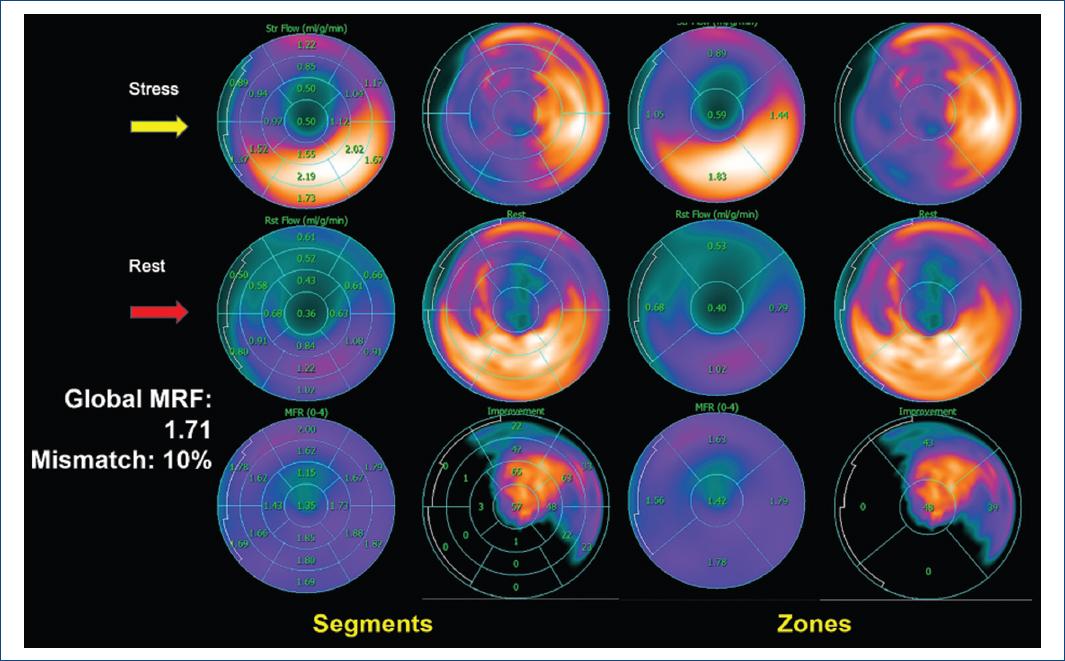
Figure 2 Dynamic polar maps of positron emission tomography NH3/fluorodeoxyglucose (FDG) flows and viability. Note the correlation between higher uptake and mismatch in segments with moderately reduced coronary flow capacity (CFCs) and less FDG uptake in zones with lower CFCs. Global MFR: 1.71; mismatch: 10%.
Myocardial perfusion quantified by regional pixel distribution of CFC is the final common expression of coronary artery disease severity for which revascularization reduces mortality. Decreased coronary flow reserve (CFR) is associated with an increased risk of cardiovascular events1.
CFC represents a novel diagnostic and prognostic parameter measured by positron emission tomography [PET], with a CFR > 3.37 and stress MBF (SMBf) > 2.39 cc/min/g considered as normal. Revascularization of patients with reduced CFC (within 90 days of PET) is associated with decreased mortality in approximately 54%2.
Mismatch between perfusion and metabolism ≥ 7% can predict LVEF recovery; but the use of CFC to predict hibernating myocardium requires further investigations. Our patient had a severe reduction of CFC defined as CFR < 1.23 and SMBf < 0.83 in the segments with the lowest FDG uptake2,3. CFC represents a highly underused parameter, compared with CFR and SMBf, yet it may have future prognostic and therapeutic implications.

