











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
Intense biopsychosocial transformations occur in adolescence, expressed through significant mental and organic changes capable of eliciting responses peculiar to this age group, which may be associated with mental disorders or inappropriate behavioral manifestations (Santrock, 2014).
These biopsychosocial transformations in adolescence may be associated with certain losses that occur during human development, such as the child’s body, childhood, identity, and socio-familial role. These combine with the processes of affective choice, and autonomy (from their parents) inherent in becoming an adult, and the physiological transformations involved in this maturation process (Jatobá & Bastos, 2007).
The relationships established between adolescents and their families and communities constitute a historical, social, and cultural formation exerting an enormous influence on various aspects of their lives. They either encourage psychophysiological responses such as self-confidence and trust in oneself and others, or trigger stress, anxiety, and depression, negatively interfering with their quality of life (Patias et al., 2017).
Everyone is susceptible to unpleasant moments and emotions that can alter their behavior and cause mood swings that can lead to temporary depression, feelings of dissatisfaction, loneliness, lack of understanding, and rebellious attitudes. However, during adolescence, teenagers undergo an intense phase of emotional reorganization, making them vulnerable to the onset of depression and anxiety symptoms (Jatobá & Bastos, 2007; Grolli et al., 2017).
Although anxiety and depression disorders are increasingly common in adolescents, there are still few epidemiological studies on the subject, particularly of schoolchildren and the use of intervention strategies to reduce these symptoms (Rocha et al., 2013).
This study evaluated students at the Instituto Federal do Ceará, a Brazilian school of professional and technological education,. The school has a rigorous process for vetting students wishing to be admitted to high school. Once admitted, students follow a challenging curriculum, which is why many parents choose to enroll their offspring in the first year of high school.
Professional and technological education in Brazil has an intense curriculum and a weekly workload, often triggering anxiety symptoms in students. The time spent on classes and studies due to the new schedule and curricular organization particularly affects students in the first year of high school (Tabaquim et al., 2015).
First-year high school students must cope with several anxiogenic and stressful factors such as tests, a curriculum with a large number of disciplines, dense content, and full-time study. They also experience difficulties adapting to a new study routine, and parental pressure to excel academically, in addition to the physical, social, and psychological changes inherent in adolescence (Soares & Almeida, 2020).
The reorganization of their daily schedule and the use of strategies to support mental health, such as regularly engaging in meditation, can help reduce anxiety, stress, and/or depression symptoms, enhancing the quality of life of these students.
During this stage, meditation constitutes a possible instrument for physical, emotional, mental, social, and cognitive strengthening. It increases concentration, contributing to the perception of physical and emotional sensations and promoting self-discipline in health care. It fosters well-being, relaxation, the reduction of stress and anxiety, hyperactivity, and depression symptoms and can easily be incorporated into the school environment (Cossia & Andrade, 2020).
This study sought to evaluate the quality of life and anxiety, stress, and depression levels in high school adolescents regularly engaging in meditation.
METHOD
Participants
This is a quasi-experimental, mixed study with qualitative features, consisting of intentional non-probability sampling, with a population of approximately 600 students. The sample comprised 473 high school students of both sexes aged 13-17, (M = 15.35, SD = 1.22, 82% white) at the Federal Institute of Ceará (IFCE), Brazil. They were enrolled in physical education classes in the first semester of 2022, with over 75% attendance rates in classes. The sample excluded those who were absent from any evaluation stage or had engaged in some kind of contemplative practice (meditation, yoga, or Tai Chi) for at least three months. As stated in the introduction to this manuscript, this educational institution was chosen because of its curriculum and weekly workload, which tend to trigger anxiety symptoms in students.
Measures
This study was undertaken in 2022, with the implementation of meditation, followed by data collection between March and May 2022.
The quality of life assessment was performed using the WHOQOL-Bref Questionnaire, an abbreviated version of the 26-item WHOQOL-100. The first question refers to the quality of life in general and the second to personal satisfaction with health. The remaining twenty-four questions focus on four domains: physical, psychological, social relationships, and environment. Domain scores represent values of between zero and one hundred, with those closest to zero being the worst and those closest to one hundred being the best. An individual who scores fifty on a particular domain can therefore be considered average for that domain (Fleck et al., 2000; Kluthcovsky & Kluthcovsky, 2009).
Depression, anxiety, and stress levels were assessed using the Depression, Anxiety, and Stress Scale for Adolescents (DASS-21), adapted and validated for Brazilian adolescents. In this scale, participants indicate the degree to which they experience each of the symptoms described in the items during the previous week on a 4-point Likert-type scale. Item scores range from 0 (does not apply to me) to 3 (applies to me a lot, or most of the time). Depression, anxiety, and stress scores are determined by adding the scores for the twenty-one items (Patias et al., 2016).
During the intervention period, Participant Observation was undertaken based on a Field Diary, rating the feelings and informal attitudes in each session. Two meetings were held through the Focal Group in the 12th and 24th sessions, consisting of three guiding questions: 1. How are you feeling today? 2. How have you felt so far with the practice? 3. How do you feel about what brought you here? (Minayo, 2012).
After the 24th session, an individual interview was conducted with twenty-eight randomly selected students. This number was determined by the theoretical saturation criterion. This interview aimed to identify the feelings and possible transformations arising from meditation, with the following questions: “Why did you start doing meditation?” and “How do you identify these feelings today?” These interviews were recorded in full by a voice recorder. Observations and non-verbal expressions were noted in a report.
Procedure
This research project was undertaken for eight weeks, during which meditation was based on focused attention with breathing in three stages, lasting ten minutes, occurring three times a week, totaling twenty-four guided meditation sessions. In addition, students were instructed to practice meditation daily (Cardoso, 2011).
First of all, the sample characterization questionnaire, the ethical consent form (personal and responsible), and the diagnostic evaluation instruments (DASS-21; WHOQOL-Bref) were administered. The diagnostic evaluation was followed by meditation practices included in physical education classes. In the 12th and 24th sessions, meetings were held in the Focus Group. After eight weeks of meditation, the quantitative assessment instruments were re-administered and interviews conducted.
Meetings usually began with students sitting on a mat in a neutral spine posture. They were asked to close their eyes and try to notice their breathing without trying to direct or control it. After a few breaths, they began counting in three counts for both inhalation and exhalation. After taking a few breaths in three counts on the leader’s command, they counted in their heads, with personal guidance according to the individual needs/desires of each participant. They counted in their heads for three to four minutes, at which point they were asked to continue breathing calmly without a set time limit. They were then asked to breathe freely and observe themselves. After about two or three minutes, they opened their eyes and discussed the experience with the leader.
Data analysis
Quantitative data were analyzed using SPSS Statistics 20.0, expressed as mean and standard deviation. The significance level established was p < .05, following the Wilcoxon test.
Qualitative data were analyzed using IRAMUTEQ software (Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires) through classic lexicographical analyses to understand the statistical data and quantify the evocations and forms. Descending Hierarchical Classification was obtained to measure the dendrogram data according to the classes generated, considering words with x2 > 3.84 (p < .05). The software identified lexical patterns through similarity analyses, subsequently validated by two independent researchers to ensure consistency and accuracy.
These statements were transcribed from the characterization of the interviewees, the testimonials they provided, and the opinions given in the focus group meetings, constituting the text corpus. Each text had a command line that was arranged for the interviews, student_01 (S1) to student_28 (S28), and for the focus group, block_01 (B1) to block_03 (B3). All data were subsequently analyzed using the content analysis method (Minayo, 2012).
The general corpus of the interviews consisted of ten texts, separated into sixty-six text segments (TS), using fifty-seven TS (86.36%). Nine segments were excluded due to problems in the transcriptions or the thematic irrelevance with respect to the analysis categories. 1,723 occurrences emerged (words or forms), including 524 different words and 303 with a single occurrence. A class diagram was organized with examples of words from each class evaluated through the chi-square test (x2) to illustrate the words in the text corpus in their respective classes. They contain the evocations that present words that are similar to each other and different from the other classes.
The general corpus of statements collected in the focus group consisted of three texts, divided into thirty-one text segments (TS), with the use of thirty-one TS (100.0%). Four hundred and forty occurrences emerged (words or forms), with 190 different words and 124 with a single occurrence.
RESULTS
This study evaluated 473 students with a mean age of 15.35 (± 1.22), 316 (66.80%) female and 157 (33.20%) male, 82% of whom were white. They were mostly students in the first year of high school (336; 71.03%), 252 (53.27%) of whom declared that they had already failed at least one subject at some time.
The results showed a significant improvement in the perception of the quality of life of these students in the following domains: physical, psychological, personal satisfaction, and general quality of life after eight weeks of regular meditation practice (Table 1). Although there were significant improvements in anxiety and stress, effect sizes (Cohen’s d) ranged from .3 to .5, showing moderate effects.
Table 1 Statistical results of the WHOQOL-bref questionnaire
| Domains | Weeks | M (± SD) | p |
|---|---|---|---|
| Physical | 0 | 1.82 (± .47) | .022* |
| 8 | 2.20 (± .96) | ||
| Psychological | 0 | 2.23 (±.84) | .018* |
| 8 | 3.34 (±.79) | ||
| Socialrelationships | 0 | 1.97 (±.95) | .092 |
| 8 | 2.14 (± .47) | ||
| Environment | 0 | 1.97 (± .56) | .073 |
| 8 | 2.18 (± .75) | ||
| Personalsatisfaction | 0 | 1.78 (± .69) | .012* |
| 8 | 3.44 (± .64) | ||
| General quality of life | 0 | 2.04 (± .78) | .014* |
| 8 | 3.57 (± .87) |
Note:M: Mean; SD: Standard Deviation;
*Statistical significance according to Wilcoxon test.
Analysis of the Depression, Anxiety, and Stress Scale for Brazilian adolescents revealed a significant improvement across all domains: depression, anxiety and stress in the comparison between before and after meditation (Table 2).
Table 2 Statistical results of the depression, anxiety and stress scale for adolescents (DASS-21)
| Domains | Weeks | M (± SD) | p |
|---|---|---|---|
| Depression | 0 | 1.59 (± .77) | .014* |
| 8 | .29 (± .19) | ||
| Stress | 0 | 1.99 (± .62) | .007* |
| 8 | .29 (± .21) | ||
| Anxiety | 0 | .83 (± .59) | .002* |
| 8 | .06 (± .04) |
Note:M: Mean; SD: Standard Deviation;
*Statistical significance according to the Wilcoxon test.
Contents of the interviews were categorized into three classes: Class 1—“Meditation in the control of psychophysiological symptoms” with nineteen TS (33.33%); Class 2—“Breathing exercises as a strategy for changing behavior” with fourteen TS (24.56%), and Class 3— “Meditation in controlling physical symptoms and improving academic performance” with twenty-four TS (42 .11%).
Each of the classes found through the analysis of Descending Hierarchical Classification was operationalized and exemplified (Figure 1).
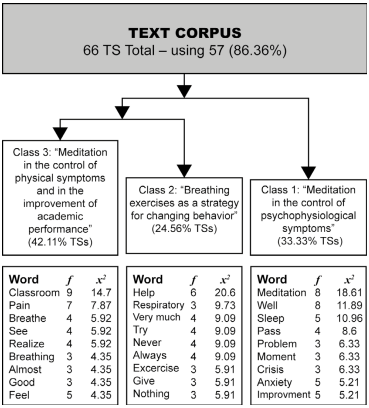
Class 1 refers to the perception of improvement in psychophysiological symptoms, such as a reduction in anxiety, chronotropic symptoms, and loss of appetite, as well as improved sleep and mood. A selection of respondents’ comments is given below:
When I’m about to do the meditation, I think, when I do it, all this will pass. I’ll feel better about the anxiety. Sometimes, when I have a problem, it will pass. It will subside. [...]. (S3)
[...] my eyes closed like this, my heart raced, I lost my appetite and had it in my head. Sometimes, I lose sleep, but today, I’m much better [...]. (S16)
[...] I was a little sleepy on the bus, as I leaned against the window. But when I got here, when I started to meditate, the sleepiness disappeared, and that’s something that I’m really impressed with. I don’t feel sleepy all day anymore, I don’t feel like staying in bed anymore, and I’ve been crying a lot less. (S5)
Class 2 points to breathing exercises as a strategy to change the behavior of the adolescent students evaluated. It shows that the pedagogical experience learned not only promotes the improvement of symptoms of depression and anxiety, but is also incorporated into the behavioral habits of these students. They provided the following testimonials:
[...] This thing of breathing counting the three counts helped me to ease my mind, you know? Defocus. Then, I no longer feel so much need for medication. (S24)
I’ve had depression for a long time, and my mother has been trying to help me for a while. Breathing exercises have made me feel so much better. I do them every day. (S4)
With you, I understood what breathing exercises were, and I said: I’ll try to do them every day whenever I feel anxious, and it really works. (S8)
Class 3 shows that regular meditation reduced physical symptoms, especially pain, common in people with anxiety, depression, and stress. It has also been cited as a practice that promotes improved grades in school subjects. Interviewee reports included the following comments:
I no longer wanted to leave the house and come to class, and I was feeling a lot of severe pain, really [...] only with breathing I noticed that these pains have diminished. I don’t know... I don’t know how to explain it. It hurts, but not so much. Nowadays, I almost don’t feel it. (S7)
[...] Whenever I get nervous during a test, I remember to breathe the way you taught me, and everything works out. (S1)
Even my grades have improved, I don’t have headaches so much, and I can sleep better. (S17)
The analyzed content of the focus group was categorized into two classes: Class 1— “Control of psychophysiological and behavioral symptoms” with 16 TS (51.61%), and Class 2— “Control of physical symptoms” with 15 TS (48.39%).
In the same way as the results presented in the interviews, a class diagram was organized with examples of words from each class evaluated through the chi-square test (x2). Each of the classes found through the analysis of Descending Hierarchical Classification was operationalized and exemplified (Figure 2).
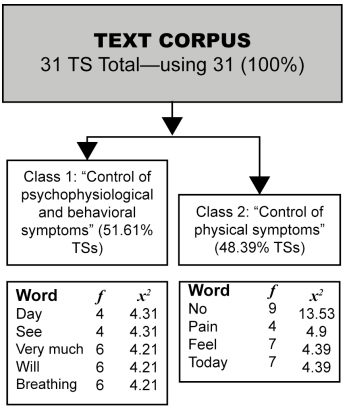
Class 1 of the focus group shows that regular meditation achieved increased willingness to perform daily activities, a sense of well-being, and improved sleep. These results corroborate those found in classes 1 and 2 of the interviews. Testimonials include the following remarks:
I wake up every day wanting to go to school. [...] feeling much more healthy and lively. I wake up early and sleep much better. (B3)
I’ve been feeling really good, you know? Getting better day by day. I don’t get so anxious anymore [...]. (B1)
I no longer feel my heart racing, and I even play with my friends more. (B2)
Class 2 of the focus group notes that regular meditation had a positive effect on physical symptoms, improved pain and fibromyalgia symptoms, improved concentration, and reduced medication use. These findings corroborate those revealed in class 3 of the interviews. Students observed the following:
[...] I no longer feel so much pain, nor do I feel so tired. I have fibromyalgia, yet despite that, my doctor said I’m doing much better. (B3)
I notice that I’m breathing better and don’t feel much pain anymore. (B2)
At first, it was hard to concentrate because of the thoughts and the pain, but today I don’t feel any difficulty. (B2)
DISCUSSION AND CONCLUSION
The assessment of the quality of life has been used for various purposes, not only by the scientific community but also in clinical practice, serving as a comparative foundation in therapies and different pedagogical strategies for mental health intervention (Patias et al., 2016).
This study showed that meditation practice helped improve the quality of life of the assessed students, more specifically in the physical and psychological domains. On the other hand, there were no statistically significant changes in the social relations and environment domains, suggesting aspects warranting further exploration in other studies.
Meditation proved to be efficient in statistically significantly reducing depression, anxiety, and stress symptoms in the students analyzed, using breathing as a technical-pedagogical foundation. However, the effects were moderate, suggesting the need for new studies to investigate the length of meditation per session, weekly frequency, and number of sessions performed, and evaluate new meditation techniques.
Psychophysiology has pointed out the close relationship between autonomic responses, such as respiratory and cardiovascular control, and the limbic system, demonstrating that breathing influences the control of emotions. In the case of the present study, they included stress, depression, and anxiety symptoms (Nemati, 2013; Brown et al., 2013; Novaes et al., 2020).
It is therefore suggested that the parasympathetic activation caused by meditation focused on breathing in three stages was able to promote the neuroplasticity of structures related to emotional regulation, alleviating anxiety and depression symptoms.
The Descending Hierarchical Classification analysis of the interviews and focus group meetings showed that meditation goes beyond the cognitive dimension, promoting significant physiological changes. The latter directly interfere with the mental flow, positively affecting the health-disease processes, quality of life and well-being, improving sleep, willingness to engage in daily activities and reducing pain and anxiety, stress, and depression symptoms.
These findings are reinforced by participant observation through the analysis of field diaries that initially described a silent, reluctant group of students. From the third meditation session onwards, they began to smile and engage in brief conversations with each other. By the sixth session, they spontaneously mentioned improvements in sleep, coupled with a reduction of chronotropic effects and lack of appetite, and greater overall well-being.
They gradually began to turn up at the meditation practice in a visibly better, livelier mood as if they had no more ailments. We observed a distinct change in their behavior, and they reported that they used the practice of focused breathing in three stages in their daily routine, particularly at times of stress, and shared it with family and friends.
González-Valero et al. (2019) point out that meditation, mindfulness programs, and cognitive-behavioral therapy can reduce stress, anxiety, and depression in schoolchildren. Ribeiro et al. (2019) mention improvements in the state of health and level of satisfaction after meditation, as well as in proprioception and the personal and collective behavior of adolescents. Pinto et al. (2023) observe that meditation practices in adolescents can be a valuable strategy for health promotion and educational training in the school environment.
School failure may be related to high levels of anxiety or emotional destabilization, especially when students regard school life as a decisive component in their lives, therefore making this environment a cause of psychological suffering (Rocha et al., 2022).
In addition, through participant observation, reports were obtained of parental pressure to excel academically and self-examination internalized by teenagers about the their future in the labor market. We also noticed the high level of discipline, the density of content coupled with less study and leisure time, as well as weaker teacher-student relationships.
Although academic performance was not directly assessed, some students reported improvements in their ability to concentrate, which warrants further exploration in future studies. In this context, the study by Yun et al. (2020)reports an improvement in self-reflection and academic attention in adolescents who meditate. Ribeiro et al. (2019)note that engaging in meditation at school can improve academic performance and positively affect the teacher-student relationship and collaborative work, in addition to reducing symptoms related to anxiety and stress.
Based on these results, we should regard school as being more than a place for knowledge acquisition and encourage this environment to help students overcome their difficulties and shortcomings in all areas of their lives. Meditation can be an accessible, low-cost instrument that promotes health and well-being for all educational actors, significantly enhancing school life.
Limitations of this study include the uncertainties of pedagogical intervention and acceptance during the period of implementing meditation practices; and prejudice regarding body-mind practices, especially in the school environment. Although this study was conducted with a large number of students, we cannot generalize findings to other school districts. This study only focused on the evaluation of students. Other school actors, such as teachers and administrators, were not evaluated. In addition, a randomized design with a control group would allow the effects of meditation to be isolated, while analyzing samples by sex could clarify specific differences.
We believe that allowing teenagers to engage in meditation at school not only enables students to cope with common difficulties in this challenging phase of human development. It also helps their teachers, classmates, friends, family members, and others who are part of their social groups, thereby enhancing the health of the school community. In addition, engaging in meditation helps promote the mental health of these students through effective, accessible, and autonomous pedagogical action.

