











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Kidney stone disease has been described since the time of Hippocrates. It affects 5-15% of the world population, with recurrence rates close to 50%.1 Percutaneous nephrolithotomy (PCNL) was developed in 1976 by Fernstrom and Johansson and established as a minimally invasive treatment option for the removal of kidney stones in the 1970s.2 Currently, the European Association of Urology (EAU) clinical guidelines panel recommends percutaneous nephrolithotomy as the first-line treatment for kidney stones measuring 2 cm, lower pole stones of 1.5 cm, and staghorn stones.3-5 It has almost completely replaced open surgery, because it is less invasive, safer, and more effective (stone-free rates of 78 to 95%).6 Traditionally, the prone position was exclusively considered for renal access. In 1987, Valdivia-Uria reported the first percutaneous access to the kidney with the patient in the supine position. Multiple position modifications emerged in an effort to simplify the procedure and improve its efficiency, marking the beginning of the era of combined intrarenal endoscopic surgery.7 Supine percutaneous nephrolithotomy achieves excellent results with a low rate of complications, and is equal in effectiveness and safety to the prone position. Adequate access to the renal collecting system, whether in the prone position, supine position, or any of the modified positions, is one of the most important aspects required for successful surgery.8 The ideal puncture should maximize the effectiveness of the procedure in terms of the stone-free rate and minimize the risk of complications.9 Stone removal depends on adequate puncture, with the preferred site being between the lower edge of the 12th rib and the upper border of the posterior iliac crest. Punctures above the 12th and 11th ribs have a 16- and 46-fold increased risk of intrathoracic complications, respectively, compared with subcostal access.10 The puncture should be medial to the posterior axillary line to avoid injury to the colon. In addition, the puncture should be sufficiently distant from the rib to avoid injury to the intercostal nerve or vessels. Puncture through the infundibulum of the upper, middle, and lower poles is associated with vascular lesions in 67.6, 38.4, and 68.2% of cases, respectively. Direct puncture of the renal pelvis can injure the retroperitoneal vessels. An important step is the dilation of the tract with the insertion of the access sheath.11 Effective renal puncture and dilatation are of paramount importance for surgical success.
CASE PRESENTATION
We present the case of a 36-year-old male patient that had a surgical history of laparoscopic cholecystectomy and an otherwise unremarkable personal medical history. He sought medical attention for bilateral, colicky, intermittent, and predominantly right-sided lumbar pain of 3-month progression, with no other accompanying symptoms. Complete laboratory work-up revealed abundant erythrocytes per field, as well as calcium oxalate crystals in the urinalysis. An abdominopelvic CT scan was performed that revealed bilateral hyperdense images. The right image was consistent with an incomplete staghorn calculus, with an attenuation index of up to 1410 Hounsfield units (HU). A right retrograde colon was also identified. Urine culture was negative and prophylactic antibiotic therapy was initiated. Left flexible nephrolithotripsy and the placement of an ipsilateral double catheter were indicated in a first surgery, followed by right percutaneous nephrolithotomy.
Surgical technique
The procedure was performed under general anesthesia with the patient in the modified Valdivia position (Figure 1). Cystoscopy with a 22-French (Fr) cystoscope was performed by inserting a 6-Fr ureteral catheter, followed by 16-Fr Foley transurethral catheter placement and a retrograde pyelogram. The distance between the last rib and the iliac crest was measured, achieving subcostal renal access through the posterior axillary line. An incision of approximately 1.5 cm and digital dissection of all layers of the anterolateral abdominal wall was made until the retroperitoneum was reached, forming a tunnel through which the renal unit was finally palpated (Figure 2). A puncture under fluoroscopic guidance (C-arm in a 90-degree fixed position) was made with a Chiba 22 G needle (Cook Medical Inc) at the level of the lower calyx, facilitated by distension with saline injection and contrast medium through the ureteral catheter with renal opacification (Figure 3). Urine was then assessed to confirm proper puncture, and a SensorTM guidewire (PTFE-Nitinol Guidewire with Hydrophilic Tip) was introduced into the ureter, with subsequent sequential dilation of the tract with Amplatz dilators up to 30-Fr in diameter (Figure 4). A 26-Fr nephroscope (KARL STORZ GmbH & Co. KG) was introduced, and pneumatic lithotripsy with LithoClast Master equipment was performed (Electro Medical Systems, Nyon, Switzerland). Flexible nephroscopy was carried out to assess the renal cavities. At the end of the procedure, an 18-Fr, 3-mL-volume nephrostomy catheter was inserted into the balloon, and nephrostography was performed. Total surgery duration was 100 minutes. The patient received standard postoperative care, his progression was satisfactory, and he was discharged from the hospital 48 h after the procedure. The nephrostomy was left in place for one week and removed when the stone-free status was corroborated. The patient is currently under multidisciplinary management by the endocrinology and urology services and is considered at high-risk for stone formation due to hypercalciuria. He is presently being treated with potassium citrate.


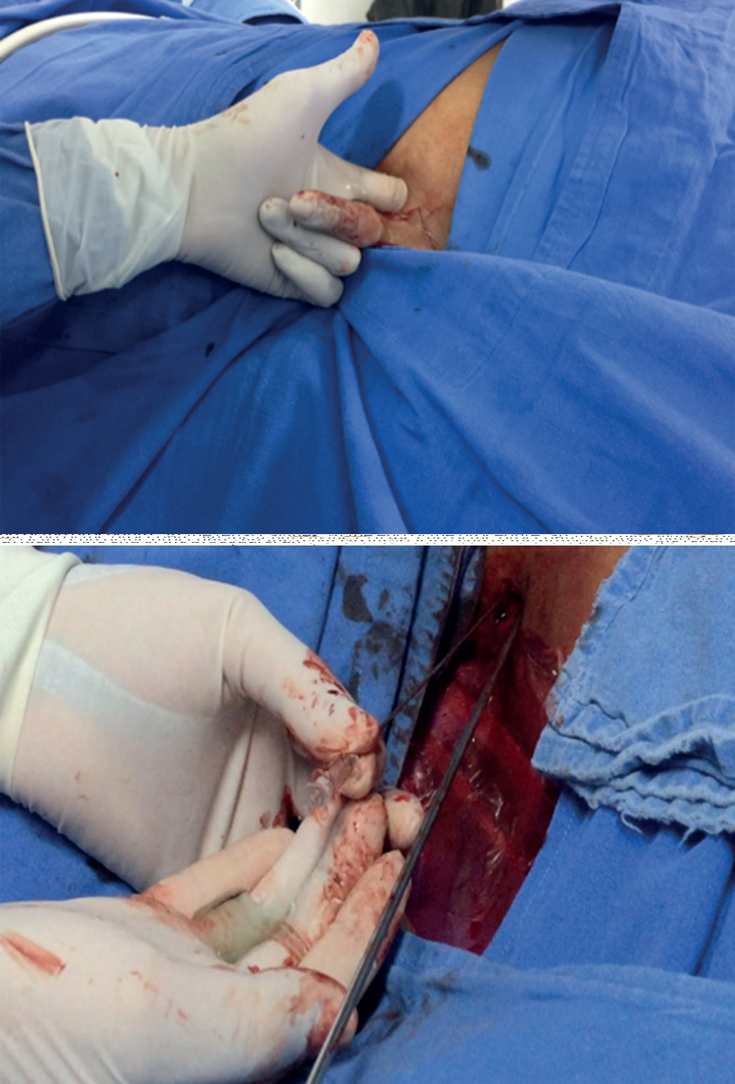
Figure 3 Renal puncture under fluoroscopic guidance through the digital tract with urine collection.

DISCUSSION
The complications of percutaneous nephrolithotomy can be divided into those related to access and those related to stone retrieval. The rate of complications reported during percutaneous nephrolithotomy ranges from 3 to 18%. Complications related to initial percutaneous access and dilatation of the tract include renal or parenchymal bleeding (perinephric hematomas), failed access, chest complications (pneumothorax or pleural effusion) and injury of the main renal vessels (<0.5% cases). There is inherent danger to adjacent organs when accessing the renal collecting system, especially to the colon, liver, and spleen. A retrorenal position places those organs at even greater risk. The risk factors for colon injury are distention of the colon, decreased perirenal fat, a left-side procedure, advanced age, female sex, horseshoe kidney, and previous renal surgery.12-13 In the supine position, the risk of perforation of the colon (0.5%) is lower because the intestine floats freely in the abdomen away from the kidney.14 Compared with single access, multiple access entails an increased risk of bleeding and complications, including a detrimental effect on renal function.15 The digital insertion and dissection technique does not cause problems for the movement of the access sheath or leakage of saline solution with its instillation during the procedure, nor is bleeding modified. The results are comparable to the conventional technique with the advantage of preventing potential complications.
CONCLUSIONS
Obtaining optimal renal access and dilation are crucial in percutaneous nephrolithotomy and are difficult tasks for many urologists. Careful patient selection and accurate positioning are essential. We believe that the technique described above offers more secure access to the renal unit and is highly useful in patients with risk factors for potential complications. The experience at our hospital center has been favorable. However, further study is needed to confirm the benefits of this technique over those of the standard procedure.

