











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroductión
The aim of this paper is to present the results of a case study carried out in health care centers of Pachuca and Zimapan in the state of Hidalgo, México. With this purpose, a review of the framework of organizational culture, health care services, and organizational culture in health care services is included. The method used was a case study under a qualitative approach with the techniques of interview and focus group, whose results were processed under a discurse analysis using the software Atlas Ti.
The outcome that arised after the results were processed was a systemic model of analysis of organizational culture in health care services.
This model could be taken as a reference in order to study health care service organizations and help them to understand their inner and outer dynamics. A long term purpose is to offer some tools for designing and implementing strategies for managers and practitioners to raise the quality of service, to enhance the level of satisfaction of patients, to reduce costs, to create a better corporate identity and to improve the organizational environment. It is important to highlight that the outcomes of this research focus only on the health care units under analysis. Therefore, the resultant model tends to explain the situation identified in the state of Hidalgo.
Organizational culture and its background
The concept of culture initially served to refer to the idea of cultivation and its subsequent derivatives such as aquaculture: fish farming; agriculture, cultivation of animals, plants and life forms; floriculture, flower farming among some others (Schwanitz, 2004, 341). Nowadays this is a multi conceptualized term due to the different disciplines that have studied it and the interaction of the globalization process that generates cultural interchanges, affecting the ideas and principles of the people, which change according to the culture of each country (Townsley, 2004, 34).
The role that culture plays in organizational environments comes to be the cultivation of organizations. Therefore, organizational culture becomes the culture of organizations which amalgamates core beliefs, habits, practices, myths, rituals, norms, clashes and expectations of the members of an organism (Hellriegel, 2004, 378).
Schein (2010, 14) defines organizational culture as "the pattern of shared basic assumptions learned by a group as it solved its problems of external adaptation and internal integration which has worked well enough to be considered valid and, therefore, to be taught to new members as the correct way to perceive, think and feel in relation to those problems”. Here, organizational culture can be analyzed in three levels: artifacts, values and assumptions. Artifacts are the visible parts of the organization like furniture, colors, symbols or even office jokes. Values are norms conceived by the high direction that rule organizational behavior and most of the time are established as written statements. Assumptions are the core beliefs that guide actions and decisions defining the organizational behavior of the entity.
Robbins (2004, 50) states organizational culture as “a common perception held by the organization’s members; a system of shared meaning”. Here stands the idea of a dominant culture that holds subcultures which share values that bring stability to the system, identity to their members and control to managers. In order to focus the elements of organizational culture in health care services, some concepts are included in the following paragraphs.
Health care services
The World Health Organization (2013) defines health as “the state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity”. Under this definition health is understood from a holistic view, integrating the physical perspective, as well as the psychological and sociological aspects of well being.
Pam Pohly´s Net Guide (1997) uses the previous definition of health and adds “It is recognized; however, that health has many dimensions (anatomical, physiological, and mental) and is largely culturally defined”. Within this definition the cultural factor is implied throughout the surrounding culture, which becomes the way to understand health according to the generally accepted values of the society where it is defined.
The Mosby’s Medical Dictionary (2009) establishes that health is “a relative state in which one is able to function well physically, mentally, socially, and spiritually in order to express the full range of one's unique potentialities within the environment in which one is living”. So, the impact of health is not only focused on the patient, but in the different environments where he/she interacts, which in health care institutions may affect the service atmosphere and, in some cases, when tension grows, the effectiveness of treatments, the quality of attention and health procedures.
About health organizations, according to Carrada (2002, 203-211), they are “a group or a professional and interdisciplinary team that works structurally to produce intangible goods -the health services- and achieve certain goals and, to get them, the agreement and participation of users is required”. So, inner factors like health services and their elements, and external factors such as patients and users are appreciated, because here there is evidently a reciprocal relationship in which health, as the result of this dynamic, does not rely only on one of the actors, but in the interaction between them.
Thus, under a systemic perspective, open issues, such as clean facilities, medical attention and clinical treatments are strongly linked to enclosed aspects, such as the physicians’ ethics, and their performance among multidisciplinary teams; as well as the patient’s fears, anger, rumors and idiosyncrasies. The result of this mixture does not only set the type of organizational culture of health care services, but actually impacts on the prescriptions and effectiveness of treatments, considering the patient as an active part of this setting.
According to the Mosby’s Medical Dictionary (2009), health care services are considered as “an organized plan of health services”. Health services include facilities, equipment and trained personnel; public health policies about water, food and drugs regulations; patients, and the surrounding culture of health of the population in general.
Health services can be provided either by public or private institutions, with operative and quality differences. Essentially, they offer the same services and search for the same goal: health. The public sector includes hospitals, specialized national institutes, health care management public offices, communitarian health centers and health houses (Blaauw et. al., 2003). In the private sector, there are doctor’s offices, laboratories, sanatoriums and specialized hospitals that offer, sometimes, health services similar to those provided by the public sector. Health services are regulated by the government. In Mexico the General Law of Health (2014) refers to health services as those provided either by public institutions, private corporations or social organizations. There is also a Comisión Nacional de Arbitraje Médico (National Comission of Medical Arbitrage) (2014), which establishes and defends the patients’ rights. These elements design an organizational behavior which derives into organizational culture.
Organizational culture in health care services
According to Bennett & Lynne (1999) “organizational culture will vary considerably between different organizational units (such as different hospitals and health centers)”. Nevárez et al. (2010, 1071-1090), note that the level of education and income level of the patient are associated with the organizational culture and efficiency of health care services. As a consequence, it is common to find that the performance of one particular health care unit is considerably better and, staff motivation considerably higher than another health care unit, which operates with similar structures and levels of resources. So, the level of performance of a health unit is determined by the interaction of its elements.
Organizational culture is also a vehicle for communication (Novato, 2009, 75-82). Hence, health organizations are both transmitters and receptors of codes, symbols, medical slang and paradigms that keep and define the effectiveness and results of health practices.
Hernández et al. (2008) report: “there are additional components of the organizational culture in the health sector relating to atmosphere, the commitment of workers of the sector and a warm and human treatment”. Therefore, the proper use of the clinical method and diagnostic means, are relevant aspects in the process of creating a health care culture, as well as the adequacy of the medical language to the patient.
About medical consultations, Montero (1998,82 -86) stated that organizational culture may have negative connotations, especially with a slow appointment system, slow delivery of drugs, the speed of medical care and the lack of an adequate service process according to the patient needs. As a consequence, they refer that the good management of interpersonal relationships among doctors and with their superiors, seem to be related to the level of satisfaction between doctor-patient interaction which should be based on communication and confidence.
Organizational culture of health units also reflects the general aspects of the surrounding culture, which influences and is influenced by society in terms of economical, legal, technological, political, religious and moral issues. So, organizational culture of health care services could be understood as a system of inner and outer elements that includes specific subsystems like skilled personnel focused on health restoration, technology and specialized equipments for diagnostics, treatments and surgeries as well as supportive care facilities and services framed in an economical, legal, social and idiosyncratic environment. Under the same perspective, Donabedian (in Coronado-Zarco, et. al., 2013, 25(1):28) considers three components for health care services: technical care, interpersonal relationships and the environment (amenities) in which the process of health care is performed. This will be reviewed from the concrete perspective selected for this paper, task of the following section.
Method
Materials and methods
The state of Hidalgo is divided into 13 health zones from where the most important health centers were selected. Information was requested from all managers, but only two zones accepted to participate in the research. The zones were Pachuca and Zimapan which include 17 health centers from where doctors' offices and private clinics -which fit into the category of first level organizations in the zones - were studied as shown in Table 1.

Additionaly, two second level organizations belonging to the Public Health System were studied throuhg interviews and observation guides: the General Hospital of Pachuca and the Mexican Institute of Social Security (IMSS) of the state of Hidalgo. These hospitals are located in the Zone of Pachuca and they are the only ones in their kind in the zones selected.
The research was focused through a case study analysis, as an empirical instrumental inquiry that investigates health care services within its context (Harvard Business School, 1997, & Stake, 2006) and a single case design with embedded units (Yin, 2009). Guides for observation, interview and focus group were used as well as semistructured interviews with randomized samples of managers and patients of the referred units.The information was processed through the technique of discurse analysis using the software Atlas Ti to create hermeneutical units established under the systemic approach according to Schein´s levels of organizational culture.
Then ontosemiotic networks were designed to understanding the system of codes and their relationships (Bencomo, Godino & Wilhelmi, 2004). The objects of the networks with two digits: one concerning the amount of witness phrases related to each code and, the second, regarding the number of relationships with other codes. Codes are listed on Table 2 shown at the end. Therefore the purpose of this research was to understand the organizational culture in these particular cases without the intention to generalize the results. For this reason, the sample size and the selection of hospitals were suitable solely for the health care units under study.

Results
Elements of organizational culture involved in health care services
It is possible to classify organizational culture of health care services in four subsystems: human, technical-technological, functional-structural, and environmental macrosystem as shown in Figure I below.

a. Human subsystem
The human aspects of organizational culture in health care services can be stated in two subcategories: patients-relatives and physicians-medical staff. According to the Medline Plus (2011), patients are “individuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures” so, the relation with the different stages and processes of health services is stated, since they become the center and reason of their efforts, as well as the receivers and evaluators of their actions and interactions.
Thus, relatives become the social net that accompanies patients in their healing process. Both of them, patients and relatives, bear a socioeconomic background that includes social stratum, fears, anger, pain, believes, idiosyncrasy and a particular perspective of illnesses, health, health care services and health culture. Table 2 shows the main witness phrases for each code of this subsystem; health expectations, professional knowledge and unhealthy habits were the most repetitive.
There is also another binomial in the human subsystem: physician-medical staff. Physicians are “individuals licensed to practice medicine” (Medline Plus, 2011), therefore the different specialties performed by them, offer the possibility to restore health. Depending on the type of disease, physicians demand professional aid provided by medical staff that “care to patients in an organized facility, institution or agency” (Idem). Here, operative personnel such as nurses, stretcher-bearers, medical office assistants, medical technicians, medical receptionists, janitors and cooks work together with specialists and physicians lead by managers, bosses and hospital directors, who also have their own point of view and frame of references about health care and health culture (Walshe & Rundall, 2001 op. cit.). These also involve social stratum, skills, language, relationship and discipline, which can be perceived by patients, relatives and users of health care services.
b. Technical and technological subsystem
Technical aspects of the technological subsystem include techniques, technology, materials and procedures. Techniques are the group of professional human practices made with specialized tools that contribute in the healing process or from which it depends. Technological equipments are those specialized devices intended to significantly help in diagnostics, treatments and surgeries. Materials are the necessary incomes for an illness treatment; and, procedures the specific patterns required to professionally managing an emergency, infirmity or administrative activity (Panamerican Health Organization, 2001).
Therefore materials, equipments and techniques complement the actions started by physicians and medical staff in order to accomplish the patient’s health expectation through aspects of security, hygiene, availability, disposals management and administrative information equipments. Transaction, quality service and technological equipment were the most repetitive codes of this subsystem (Table 2).
c. Functional structural subsystem
Depending on the type of capacities of a health unit, there are several tangible and intangible aspects (Ramírez, 1995, 456-462) that define its functional-structural subsystem. Leadership for instance, is an organizational strength where authority should be exercised properly, ensuring the right integration of teams, a timely supply of inputs, medicines, instruments and materials, as well as creating an atmosphere of respect and collaboration. Vogus et al. (2010, 60-77) point that for safer practices in health care organizations, these organizations need a coherent organizational culture that sustains the salience and further development of relevant practices.
Communication, therefore, should be clear, accurate and timely but, in health environments, should especially be agile and understandable. The medical slang should not become an obstacle for the interaction with patients, but a mean to increase efficiency among interdisciplinary teams. It is true that there are components of the working environment which are difficult to control -especially making a distinction between public and private organizations since their operation is usually different- nevertheless, a friendly atmosphere, a sense of belonging and an appropriate high level of integration can be perceived by the users of health care services, patients and their relatives.
It is possible to define values that should characterize a health care provider, having in mind that in the physician-patient relationship, aspects of warmth, courtesy, kindness, dignity, humanism and solidarity are factors that impact not only on the organizational culture (Scott, et. al., 2003, 923-945), but even in treatments, convalescences, recoveries and mind settings of patients and relatives. In other words, service should be understood not simply as giving appointments or prescriptions but as the prompt, kind, and efficient action in diagnostics, treatments and surgeries, which lead patients to restore their health with less work, and lower economical, psychological, physical and familiar costs. Values, ethical behavior, corporate image and communication were the most repetitive codes of this subsystem (Table 2).
d. Environmental macrosystem
The environmental macrosystem refers to the aspects surrounding health care services; where rules, regulations, norms and laws (Muslin, et al. 2010) constitute the legal framework of health care organizations. The macro and micro economical aspects of the environment are also included in this system, together with beliefs and practices of society reflected in its health culture included in this category. Regulatory framework, reputation and practices of self-medication were the most mentioned codes of this subsystem (Table 2).
Systemic model for the analysis of organizational culture in health care services
Resultant from the ontosemiotc nets carried out in this study, the following model shows a systemic perspective of organizational culture in health care services according to the subsystems explained above.
Source: authors´ elaboration.
Figure 2 Systemic model of analysis of organizational culture in health care services
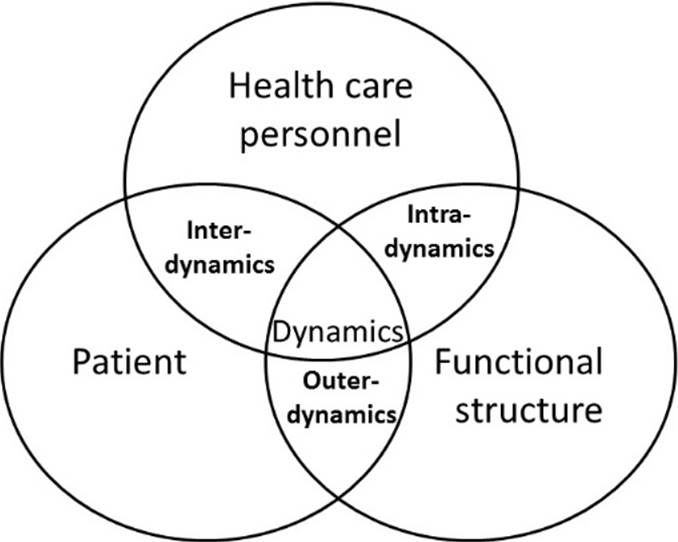
The model shows three Holons that display the interaction among the constitutive elements of organizational culture in health care services. The first Holon refers to the inherent aspects of the patient such as fears due to health disorders or infirmity, healthy or unhealthy habits, personal background reflected in idiosyncrasy, the economical situation and possibilities from the patient’s social stratum and circumstances. The second Holon represents the structural aspect of health care services, including financial and material resources, technical and technological practices and equipment, in addition to the conditions of facilities and materials. The third Holon corresponds to the health care personnel, whose medical slang, ethical behavior, clinical work to treat specific diseases and patients, proper interaction with colleagues and authorities, professional knowledge and expertise, as well as his/her social stratum, determine the interaction with patients and the quality of the services.
Explanation of the model
In order to define a relationship among the three Holons of health care services a dynamic is identified where all the elements and subsystems interact. This is based on a transaction of information, attention, resources, services, commands and interventions, as shown in Figure 3.
Source: authors´own elaboration.
Figure 3 Transactional dynamic of organizational culture in health care services
The transactions from this dynamic can be stated in three levels: outerdynamic, intradynamic and interdynamic. Each level presents a range of interchanges of elements that define the points of intersection in every Holon. The following lines explain each transaction with its corresponding reference in the ontosemiotic networks. It is important to point out that the numbers in parenthesis refer to the source and mentions of each code.
a. Outer dynamic
The external level and first aspect of the dynamics of health care services is where patients make contact with health care providers such as doctor’s offices, hospitals, sanatoriums and laboratories (Romo, 2003). Here the patient works as a double agent: like the income for health care services and the transmitter of the surrounding health culture, which reflects the importance given to infirmity, the practices of self medication, hygienic conditions and the use of alternative medicines (Figure 4).

The outer dynamic starts with the accessibility to health care services, where micro economy is an important criterion to consider the sort of services at hand. When it is defined, the type of illness (code: Health basic needs, 33-10) becomes another criterion to select the health care provider (27-9). In this transaction there is an interchange of health expectations (107-5), needs and fears, which interact with the opportunity, effectiveness, quality, resources and accessibility of health services (code: Quality service, 80-11), strengthening the faith and reliability (29-7) of the provider or weakening it, due to a perception of bad service (24-4) expressed in a distant, cold, slow, expensive or unfair attention (Figure 5).

In this level, technical and technological equipments (16-2) are not a defining criterion for the selection of health care providers; they are just complements and tools in the search for health, which is commonly accepted by a patient. It normally gets importance when the provider cannot offer the service and then the issues of costs, distance and possibilities of use of the equipments become criteria to select the health care provider.
In the outer dynamic is basic to create a good relationship with patients, taking into consideration kindness, promptness, accuracy and availability of personnel, equipment, drugs and spaces in facilities for a good and efficient attention (code: faith and reliability 29-7).
b. Intra dynamic
In this level, the contact is among the members of the organization: doctors, nurses or administrative staff (Figure 6). Here, the transaction is given in multiple ways such as treatments, diagnoses, commands, reports, information, financial interchanges, medical or surgical materials and coordination for the use of spaces. Multidisciplinary work is part of this dynamic interrelation, and the ethical aspects of medical practices are common in this stage, where the professional knowledge is an important element and, together with the value of discipline, become sensible aspects that impact on the organizational climate of the entity.

At this level there is certain risk of developing higher levels of occupational strain and stress, provoked by the performance of health care services (Flores et al., 2010:1-15). Also, it is necessary to point out the existing menace of injury and disease in the mean (Chowdhury and Endres, 2010, 182-198), so as part of the organizational culture, transactions (175-9) on this dynamic comprehend security measures and practices (Figure 7). Therefore an opportunity arises for managers to introduce politics with the personnel, in order to help them to find satisfaction in their work (codes: policies of quality 16-6 and Policies of organization 15-6). In this way it will be possible to avoid stress as well as some other diseases from the environment using leadership and communication as strategies (code: organizational climate 5-6). All of these, jointly with management facilities, spaces and equipments will lead to the whole system good performance.

Additionally the timely supply of inputs, materials and equipments represents the opportunity to offer an agile service, taking into consideration low costs and promptness for the organizations as well as for patients (code: quality service 80-11).
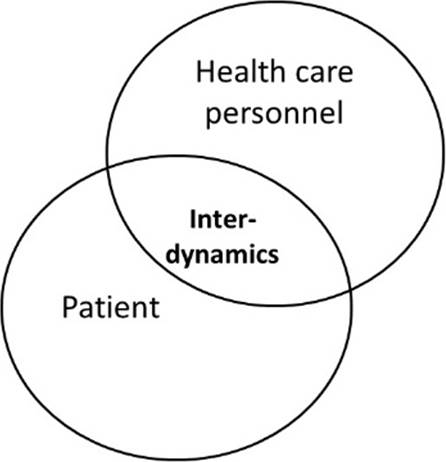
c. Interdynamic
During this stage comes a “moment of truth” when patients meet the health care (Figure 8). The organizational culture of the entity faces the culture surrounding the patient and the transactions (175-9) tend to be more “client-provider styled” (Figure 9).
Source: authors´own elaboration.
Figure 8 Interdynamic of organizational culture in health care services model

At this stage the personal aspects of patients such as fear (6-2), anger, anxiety, desperation, pain expectation, awe or social stratum, make contact with the personal aspects of the health care staff, like ethics, professionalism, responsibility, medical slang, collegiate work and also social stratum (code: health expectations 107-5). This will be important in order to establish a perception of the services altogether with the cleaning of facilities, availability of equipments and materials and with healthy or unhealthy habits (codes: healthy habits 21-4 and unhealthy habits 64-4), to define a way to interact and also affect the service and work atmosphere.
Therefore, the effectiveness of treatments and prescriptions is also embedded in the idiosyncrasy of the patient, who might have good or bad health habits that, simultaneously with the expectations of health and confidence to the institution and doctor, become determinant to reach a complete state of well being. This will bring feedback to the interdynamic in the level of patients and relatives satisfaction (code: user satisfaction 17-3), which is important because they evaluate the service and take their opinions to the outer environment, where these are transformed into reputation and corporate image (codes: social perception 22-7, quality service 80-11 and reputation 62-5).
Conclusions
According to the models presented in this paper, it is possible to conclude that in health care services in the State of Hidalgo managers are the main responsible for the adequate performance of the dynamic of organizational culture, since their position becomes the link between the three Holons and the environmental macro system, acting as performers of the system and regulators of its actions. Managers also implement policies of quality and organization, and use leadership and communication, as determinant factors to handle the entity and all its elements, working as well as the mesh that articulates the different dynamics also exposed.
In the same way the systemic model shows that patients play a triple role in this dynamics, because according to their stage become the client, the income or the product of the activities of health care services, providing the model of a cybernetic view when making contact with the environment. This is due to the feedback received by the health culture, the regulatory framework and society in general, producing effects on corporate image and reputation, as well as in quality and satisfaction of patients, relatives and users.
Even more, patients should realize about the improvement, or not, of the service since, directly or indirectly they pay for it. But patients are not certain about what helps them to get better, even though, they know that the entire organization contributes to their health improvement as was shown in the systemic model presented above.
Values are the key elements to gather subsystems of the systemic model to the environment, since they appear in every Holon and can be used as tools to comprehend and be comprehended. This could be, either as a member of the medical staff, a manager in health care services, a doctor or a patient, understanding the reasons, needs and circumstances of the dynamics of every participant, emphasizing communication as the way to interact with all the actors.
Finally, further research should focus on what the customer thinks about those issues that led him to health, and then to identify those elements which really helped him to improve, extending the range of influence of these studies to national units and to the different dynamics established.

