










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.17 no.1 Ciudad de México ene./mar. 2013
Original research
Cephalometric description of facial patterns in skeletal open bite
Gloria Eréndira Acuña Dávalos,* Mauricio Ballesteros Lozano,§ Guillermo Oropeza SosaII
* Graduate, Orthodontics Specialty, Graduate School, National School of Dentistry, National University of Mexico.
§ Professor, Orthodontics Specialty, Graduate School, National School of Dentistry, National University of Mexico.
II Professor, Orthodontics Specialty, Graduate School, National School of Dentistry, National University of Mexico.
ABSTRACT
Different open bite indicators have been described in scientific literature. However, to attain proper and stable treatment it is important to be able to identify the etiology of the malocclusion. Facial patterns are directly related to growth direction, and therefore to the vertical behavior of bone bases. They embody a crucial factor for open bite expression. Description of facial pattern through cephalometric measurements supplies information of affected bone structures, providing thus an easier treatment. The aim of the present study was, using Bimler facial formula, to identify bone structures involved in open bite cases. Facial pattern was determined through upper basal angle, lower basal angle and suborbital facial index. The study encompassed 40 lateral skull x-rays taken from patients attending the Orthodontics clinic at the Graduate School, National School of Dentistry, National University of Mexico, within the 2004-2006 period. Patients had received diagnosis of skeletal open bite. This diagnosis was emitted with the help of open bite cephalometric indicators. Dominant facial pattern in skeletal open bite was leptoprosopic. Six different relationships were found among upper and lower basal angles. Maximum open bite relation was 27.5% with both jaws involved, followed by 40% (M/L) with less severity, 5% (L/L) with greater compensation, 5% (D/M) and m/ML with 2.5%.
Key words: Open bite, facial pattern, cephalometry, malocclusion.
INTRODUCTION
In open bite cases, dysfunction can be primary or secondary. According to dysfunction location, open bite can be anterior or posterior. In cases of primary dysfunction having as main etiologic factor abnormal muscle function, the growth pattern is generally towards a middle or horizontal direction. In open bite problems with vertical growth, dysfunction is mainly secondary or adaptative. In cases with primary dysfunction and at least medium growth functional devices have greater probability of success.
Problems related to anterior and posterior dentoalveolar open bite can generally be attributed to abnormal posture and functioning of the tongue. In cases of mixed dentition, these problems normally respond successfully to treatment with functional devices. In skeletal open bite cases, growth pattern is genetically determined and is frequently associated to a pronounced ante-gonial notch. This type of cases does not offer favorable prognosis for orthodontic treatment. Inclination of maxillary base must be taken into consideration in open bite problems. Maxillary base inclination can be due to functional factors as well as habits.1,2
In the case of a skeletal open bite, which progressively deteriorates because growth is clearly vertical, causal treatment is not possible. Since in these cases, lingual dysfunction is secondary to the primary morphogenetic base, therapeutic demands are more rigorous. The use of fixed devices, frequently with tooth extractions, offer a more efficient corrective approach. In extreme cases, orthognatic surgery is the only viable alternative after completion of growth period. In mixed dentition cases, partial improvement can be obtained through dysfunction elimination. Nevertheless, this does not mainly alter the growth pattern, which will at a later point require other therapeutic methods. Vertical growth can partly respond to firm orthopedic forces or to a specially designed activator. Fixed orthopedics with strong vertical traction can alter the direction of mandibular growth and at the same time restricting eruption of the posterior segment, while the activator has the potential to affect inclination of the maxillary base. Growth form analysis is necessary to determine which therapeutic approach is most likely to succeed. A proper cephalometric analysis allows classification of open bite malocclusions.
In skeletal open bite cases, anterior facial height is excessive, especially at the level of the lower third, while the posterior height (ramus height) is short. The mandibular base is usually short and frequently exhibits ante-gonial notch. The symphysis is long and narrow, and the ascending ramus is short. The gonial angle (especially its lower section) is large, and growth pattern is vertical. According to the inclination of the maxillary base, or palatal plane, the following variations can be observed:
1. A vertical growth pattern is frequent in cases showing upper inclination of the front end of the maxillary base. An anomaly can be produced in certain patients, in which a series of unfavorable sequels combine to produce a serious skeletal open bite problem.
2. A vertical growth pattern with lower inclination of the front end of the maxillary base can also be observed.
3. Another variant includes a pattern of horizontal growth with open bite produced by an anterior-superior inclination of the maxillary base.3
Bimler facial formula describes the facial pattern by relating three angles. The first one, sub-orbital facial index, identifies the general facial vertical behavior. Sub-orbital facial height is designed as the distance existing between the chin point and the horizontal FH. Facial depth is defined as the distance among FH projections from points A (A') and C (TM). This index is graphically determined by marking the sub-orbital height FH-Me and transferring this measurement with a compass centered in A' for FH (Figure 1). If these markings are found in front of TM the face will be considered as dolichoprosopic or brachyfacial. In cases where markings are found at the TM and the point where the plane is longitudinally cut, we will have a mesoprosopic or mesofacial face. In cases where the markings are found beyond the clivus plane it will be leptoprosopic or dolichofacial face. The second angle is the upper basal angle. This angle is formed by the clivus plane and the palatal plane. (Figure 2) The third angle is the lower basal angle formed by the mandibular plane and palatal plane (Figure 3).



Values for every angle are shown in table I.
It is important to take into account the growth pattern. This is due to the many reactions of growth patterns in every individual to the neuromuscular anomalies and vice-versa. Diagnosis is a crucial factor in open bite problems. Indications for possible treatment must be established as well as a specific cephalometric analysis.
METHODS
The present study is of a descriptive and transversal nature. It is based upon cephalometric diagnosis of patients with skeletal open bite treated from 2004 to 2006 at the Orthodontics Clinic of the Graduate School National School of Dentistry, National University of Mexico. The patients were diagnosed with the objective of determining variations in facial patterns. Points were traced, and after that, cephalometric planes were equally traced in the diagrams, on cephalometric tracing acetate with pencil number 5, Ricketts ruler and geometric squares.
One single operator performed the procedure so as to avoid technique discrepancies. With respect to the cephalometric analysis, skeletal open bite diagnosis was used with the following cephalometric measurements: palatine - FH, SN - mandibular (PM), upper (superior) gonial (Upp Go ) Lower gonial (Low Go), Ricketts facial height ( Rick height), anterior facial height (AFH) posterior facial height (PFH).
Pal-FH . Angle formed by palatal plane (ENA-ENP) and Frankfurt plane (Po-Or).
SN-PM . Angle formed by anterior cranial base (S-N) and mandibular plane (Go-Me)
Upp Go . Angle composed by the posterior cranial base (S-N) and the mandibular plane Go-N.
Lower Go . Angle formed by Go-N plane and mandibular plane (Go-Me)
Rick height : Angle formed by ENA-Xi plane and plane Xi-Pm.
ODI is the arithmetic sum of the A-B plane angle to the mandibular angle, and of the palatine plane angle to the Frankfort horizontal plane.
AFA . Distance from point N to point Me.
AFP . Distance from point S to point Go
Upper basal angle (UBA) . Angle formed by clivius plane and palatine plane.
Lower basal angle . Angle formed by palatal plane and mandibular plane.
Sub-orbital facial index (SFI) . Sub-orbital facial height is defined as the distance between the Menton point and the FH. Facial depth is the distance between FH projections of points A (A') and C' (capitulare). This index is graphically determined by marking sub-orbital height FH-Me and transferring this measurement with a compass with center at A' for FH (Figure 1).
Once the three variables of the Bimler facial formula were established for each sample, the formula was as follows:

RESULTS
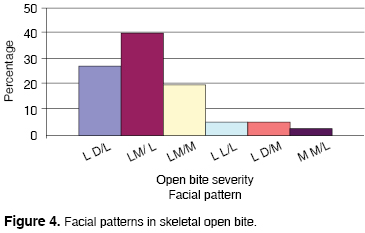
In cases of skeletal open bite, dominant facial patterns corresponded to the leptoprosope. Six different relationships were found between upper and lower basal angles. Open bite maximum relationship corresponded to 27.5% (D/L) with both jaws involved. With lesser severity, they were followed by 40% (M/L), 20% (M/M), 5% (L/L) reflecting greater compensation, 5% (D/M) and M M/L with 2.5% (Figure 4). Used statistical analysis was a one way T test. SPSS statistical program was used. Table II shows data on averages and standard deviation.
DISCUSSION
In 1974 Dr. Young H. Kim designed the Overbite Depth Indicator ODI, which was the arithmetic sum of A-B plane angle with the mandibular plane, and the palatal plane angle to the Frankfurt horizontal plane. Norm was 74.5 degrees with 6.07 standard deviation, a 68° or less value indicates skeletal open bite or tendency towards it.4
Zou et al (2001) researched the different cranio-facial types of anterior open bite. Patients afflicted with anterior open bite were divided into three types: dentoalveolar, rotation, CW mandibular, long face, CCW maxillary (upper) rotation as well as skeletal class III.5
Tsuchida et al, (1989) studied morphological characteristics of patients afflicted with open bite who suffered disharmonies in anterior-posterior relationships between upper and lower jaw. They found more dentoalveolar factors in the group where ANB was lesser than 4.5°. Skeletal factors predominated in the group where ANB was lesser than 1°.6
Beane et al conducted a cephalometric comparison among African American and Caucasian patients with and without anterior open bite. They found that anterior open bite incidence is three to four times higher in African Americans than in Causasians.7
Stefan et al found that an increase in lower facial height during treatment tended to decrease overbite depth. Excessive increase in symphysis height could almost ensure relapse.8
Haralabakis (1994) assessed cephalometric characteristics which contributed to the development of open bite in adults. The assessment was conducted under tri-dimensional perspective with posterior-anterior and lateral skull x- rays.9
Tanaka (1990) studied the morphological characteristics of Class I and Class II open bites.10
In the present study, in all measurements, lower goniac and mandibular angles were found to be most distant to their norms. In all cases, upper goniac angle was found to be decreased. This compensation explains the value, within the norm, of the total goniac angle. These findings proved to be contrary to those encountered in other studies where total goniac angles were found to be increased.7,10 Posterior facial height was found to be within the norm. Anterior facial height was found to be increased, therefore, in that case, no compensation was encountered since, in all cases, growth direction was found to be below norm, that is to say CW.
CONCLUSIONS
No history was found concerning research on open bite in relation with facial pattern, therefore, comparison of results attained in this study was not possible. Nevertheless, it is noteworthy to mention that as was the case in this project, the attempt to classify open bite based on different parameters plays an essential role when emitting diagnosis and making decisions pertaining to orthodontic or orthodontic-surgical treatment.
In the present study, it was generally found that there was a relationship between measurement of facial pattern and measurements commonly used to assess open bite severity. Nevertheless, it is suggested to expand the sample in future studies. Bimler facial formula could then be useful as an additional tool when emitting open bite diagnosis.
It is recommended to conduct further studies focused on facial patterns encountered in open bite cases, since this has a direct bearing on the vertical behavior of bony bases, and therefore could be considered the origin zone for this type of malocclusion.
REFERENCES
1. Houston WJB. A textbook of orthodontics . Gran Bretaña. Ed. Wright. Second edition. 1998. [ Links ]
2. Stockfisch H. The principles and practice of dentofacial orthopaedics . United Kingdom. Quintessence Books. 1998. [ Links ]
3. Graber T, Rakosi T, Petrovic A. Ortopedia dentofacial con aparatos funcionales. España. Harcourt. Segunda edición. 1998. [ Links ]
4. Silva R. Aplicación práctica de los indicadores de profundidad de sobre mordida vertical, displasia anteroposterior e índice de extracción . UNAM, FES Zaragoza 2004. [ Links ]
5. Zou B, Zeng X, Tseng JY. A classification of anterior open bite. Zhonghua Kou Qiang Yi Xue Za Zhi . China 2001; 36 (1): 61-63. [ Links ]
6. Tutshida T, Moniromoto. Open bite morphological study on open bite patients. Nippon Kyoser Shika 1989; 48 (5): 496-506. [ Links ]
7. Beane R, Reimann G. A cephalometric comparison of black open-bite subjects and black normals. The Angle Orthodontist 2002; 73 (3): 294-300. [ Links ]
8. Beckman S, Segner D. Changes in alveolar morphology during open bite treatment and prediction of treatment result. European Orthodontics Sociaty 2002; 24: 391-406. [ Links ]
9. Haralabakis NB, Yiagtzis SC, Toutountzakis NM. Cephalometric characteristics of open bite in adults: a three-dimensional cephalometric evaluation. Int J Adult Orthodon Orthognath Surg 1994; 9 (3): 223-231. [ Links ]
10. Tanaka S. Morphological study of open bite. Skeletal Class I and Class II open bite. Aichi Gakuin Daigaku Shigakkai Shi . Japón 1990; 28 (4): 1129-1150. [ Links ]
LECTURAS RECOMENDADAS
- Villavicencio J. Ortopedia dentofacial ''Una visión multidisciplinaria''. Colombia. Actualidades Médico Odontológicas Latinoamérica, C.A. 1997. [ Links ]
- Mc Namara JA, Brudon WL. Tratamiento ortodóntico y ortopédico en la dentición mixta . Estados Unidos. Needman Press. Quinta edición. 1995. [ Links ]
- Proffit W. Contemporary orthodontics . United States of America. Mosby Year Book. Second edition. 2006. [ Links ]
- Arat ZM, Iseri H, Arman A. Differential diagnosis of skeletal open bite based on sagittal components of the face. World Journal of Orthodontics 2005; 6 (1): 41-50. [ Links ]
- Klocke N. Anterior open bite in deciduous dentition. Longitudinal follow up and craniofacial growth considerations. Am J Orthod Dentofacial Orthop 2002; 122 (4): 353-358. [ Links ]
- Díaz JM, Velázquez R. Caracterización cefalométrica del síndrome de mordida abierta anterior. Revista Cubana de Ortodoncia 1996: 11 (2). [ Links ]
- Tsuchida T, Morimoto T, Inoue N, Hayashi S, Imai T, Takeuchi M, Nakamura S. Morphological study on open bite patients. Nippon Kyosei Shika Gakkai Zasshi 1989; 48 (5): 496-505. [ Links ]
- Cangialosi TJ. Skeletal morphologic features of anterior open bite. Am J Orthod 1984; 85 (1): 28-36. [ Links ]
- Dung D, Smith R. Cephalometric and clinical diagnoses of open bite tendency. Am J. Orthod Dentofac Otthop 1988; 94: 484-490. [ Links ]
- Argüelles A, Oropeza G, Guerrero J. Características radiográficas de la mordida abierta esquelética. Rev Odont Mex México 2007; 11 (1): 20-23. [ Links ]
Note This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam Mailing address:
Mailing address:
Mauricio Ballesteros Lozano
E-mail: maubalo29@hotmail.com

