











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkFemale 23-year-old patient with heart murmur diagnosed in the first year of life. She attended to our institute with progressive dyspnea and palpitations of 7-month evolution. Physical examination showed perioral and distal cyanosis with digital clubbing, oxygen saturation of 79%, jugular plethora, arrhythmic heart sounds of upper limbs, fixed second heart sound, systolic tricuspid murmur, and edema. Electrocardiogram and 24 hour Holter monitoring showed atrial fibrillation and right bundle branch block. Transthoracic echocardiogram revealed Ebstein anomaly with moderate displacement of tricuspid septal leaflet (46%), atrialized right ventricle of 37%, functional ventricle of 63% (A), double tricuspid lesion with severe regurgitation, tricuspid area of 2.26 cm2 (B, C), ostium secundum-atrial septal defect (diameter – 19 mm) with right-to-left shunt (D), infundibular dilation (E), non-obstructive cor triatriatum dexter (F, G), and decreased left ventricular ejection fraction (LVEF – 30%). Cardiac magnetic resonance showed biventricular systolic dysfunction (LVEF: 26%, right ventricular ejection fraction: 19%) and fibrosis of the right atrium, interventricular septum and in the sites of septal and posterior leaflets adherence to the right ventricle, (H, I) (Fig.1).
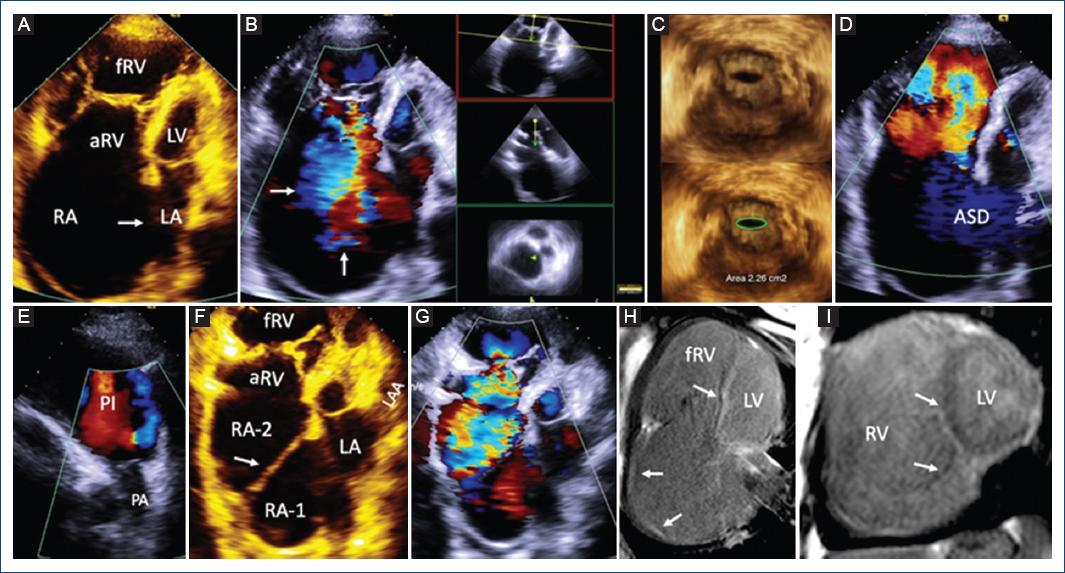
Figure 1 Transthoracic 2-D and 3-D echocardiography and cardiac magnetic resonance. A: Four-chamber view showing moderate Ebstein’s anomaly with atrial septal defect (arrow). B: Severe tricuspid regurgitation (arrows). C: 3D echocardiogram showing tricuspid stenosis area of 2.26 cm2. D: Atrial septal defect with right to left shunt. E: Infundibular dilation and normal pulmonary valve. F: Modified four chamber view showing the membrane (arrow) dividing the right atrium in two chambers: RA1 and RA2. G: Color Dopplerrevealed severe tricuspid regurgitation and non-obstructive membrane. H: Four-chamber view and I: short axis of both ventricles with the right atrial and septal fibrosis, also fibrosis in the sites of septal and posterior leaflets adherence to the right ventricle, (arrows). RA: right atrium; aRV: atrialized right ventricle; fRV: functional right ventricle; LA: left atrium; LV: left ventricle; ASD: atrial septal defect; PI: pulmonary infundibulum; PA: pulmonary artery; RA-1: right atrium 1; RA-2: right atrium 2; LAA: left atrial appendage.
The patient received medical treatment and oxygen with improvement on clinical symptoms and oxygen saturation – 94%. She was not considered a candidate for surgical treatment. Actually, she continues her follow-up in the outpatient clinic, and she is in functional NYHA Class II.
Cor triatriatum dexter is an extremely rare congenital heart disease with a prevalence of 0.01%1. In this abnormality, the right atrium is divided into two parts by a membrane, resulting on the lack of regression of the right valve of sinus venosus and it is usually associated with other congenital anomalies2.
The multimodality imaging allowed us to establish the precise diagnosis and make therapeutic decisions.

