











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The care of persons with disabilities in Mexico is characterized by inequalities. A total of 23.1% of the Mexican population with disabilities >15 years of age lack access to formal education, and their participation in economic activities is 39.1%, compared with 64.7% of their counterparts without disabilities.1 Among indigenous population above the age of three years, the prevalence of disability is 7.1%, while in whole Mexican population, this is 6%. Furthermore, only 46.5% of the disabled population aged 3-29 years attends school, compared with 60.5% of the population without disabilities.1
Inequalities are influenced by systematized preconceptions from large descriptive representations denominated disability models (DM). The DM discussed in this work include the following: 1) charity; 2) medical/rehabilitation, and 3) the social model.2,3,4
In the charity DM, disabilities are identified with imperfections, impurities, faults, penalties, or damages that obey supernatural causes resulting from the irascibility of the gods, the expiation of sins, misfortune caused by spirits, ill omens, or sorcery.2 In this view, persons with disabilities are depicted as unproductive, useless, dangerous, or unnecessary to society.
Two variants of this model are recognized: 1) the eugenics submodel, with an emphasis on practices such as infanticide or forced sterilization, and 2) the marginalization submodel, which promotes the segregation, abandonment, or confinement of persons with disabilities.5
The medical/rehabilitation DM states that the etiology of disabilities is due to scientific reasons. Disability is defined as a deficiency, an alteration, a failure, or a need to be addressed: “as a ’personal’ problem caused by disease, trauma, or any other impairment of health requiring medical and rehabilitation assistance such as a individualized treatment provided by professionals”.6 To the extent possible, medical intervention seeks the social inclusion of people affected by the failure, loss, or injury of an organ, a sense, or a bodily function. To achieve this, medical facilities have developed services staffed by specialists, among which are rehabilitation medicine, orthopedics, ophthalmology, neurology, neumology, and rheumatology. In this DM, persons with disabilities are considered to be useful provided that they can be standardized through their habilitation or integral rehabilitation.
The social DM assumes that the causes of disability are not religious or medical, but that they result from a society designed to meet the needs of “normal” people; thus, diversities are not taken into account. It also presupposes that all human life is equally worthwhile and valuable; therefore, persons with disabilities can contribute to society, as does the remainder of persons without disabilities, always by means of inclusion, equity, and respect. This model is related with the defense of human rights. It attaches great importance to principles such as autonomy, allowing advocacy for the removal of barriers to equal opportunities. Even the right of persons with disabilities to live outside of health care institutions (as do persons without disabilities) is promoted, through deinstitutionalization policies.2
There is a mixture of medical/rehabilitation and social DM 7 that is known as the integrator or biopsychosocial DM. Driven by the World Health Organization (WHO), this DM is characterized by supporting principles such as personal autonomy, while maintaining the preponderance of certain deficiencies and medical conditions. This perspective attempts to balance the interaction of contextual, environmental, or social factors with the health status of individuals.8,9
Tacitly, some documents often argue that DM correspond to historical periods in chronological succession.2,3 This a priori view has permeated the main official documents on this subject in Mexico. To test whether this association is correct or not, in this paper we analyzed the three main DM described, by means of periodization with timelines, depicting the major milestones in disability in the country.
Materials and methods
Study selection. We designed a search strategy focused on documents published in English and Spanish from 1980 to 2015, conducted in the following specialized databases: Medline; ScienceDirect; EBSCO; Google Scholar, and Bibliounam, seeking studies on the three DM analyzed in the Mexican official discourse on disability.
Inclusion criteria were as follows: 1) articles analyzing DM in Mexico over time; 2) official documents where these models apply to particular historical periods, and 3) federal care programs in disability. Exclusion criteria were the following: 1) fragmentary studies in which DM have no direct application to historical periods or are incomplete, and 2) studies referring other classifications or typologies of DM. By not including patients, this study does not require the evaluation of an Ethics Committee.
After a first inclusion of 169 documents, five of them were considered to be representative of DM associated with historical periods within the Mexican official discourse, and were finally analyzed: three from the Instituto Nacional de Estadística y Geografía (INEGI) 1,10,11 and two federal programs.12,7
Timelines. Once the documents were selected, we employed timelines to plot visual structures in the corresponding historical periods within each DM. Situating events through this proposed method, in addition to being a valuable tool for thinking,13 can help locate patterns, non-numerical trends, gaps, and turning points.
Applied to the historical analysis of DM in Mexico, the resulting timelines provide the graphic representation of a chronological sequence of events,14,15,16 with an emphasis on the specific milestones outlined in each period.17 The timelines allowed us to examine the relevance of the association of DM with historical periods, as assumed in the official discourse on disability in Mexico.
Results
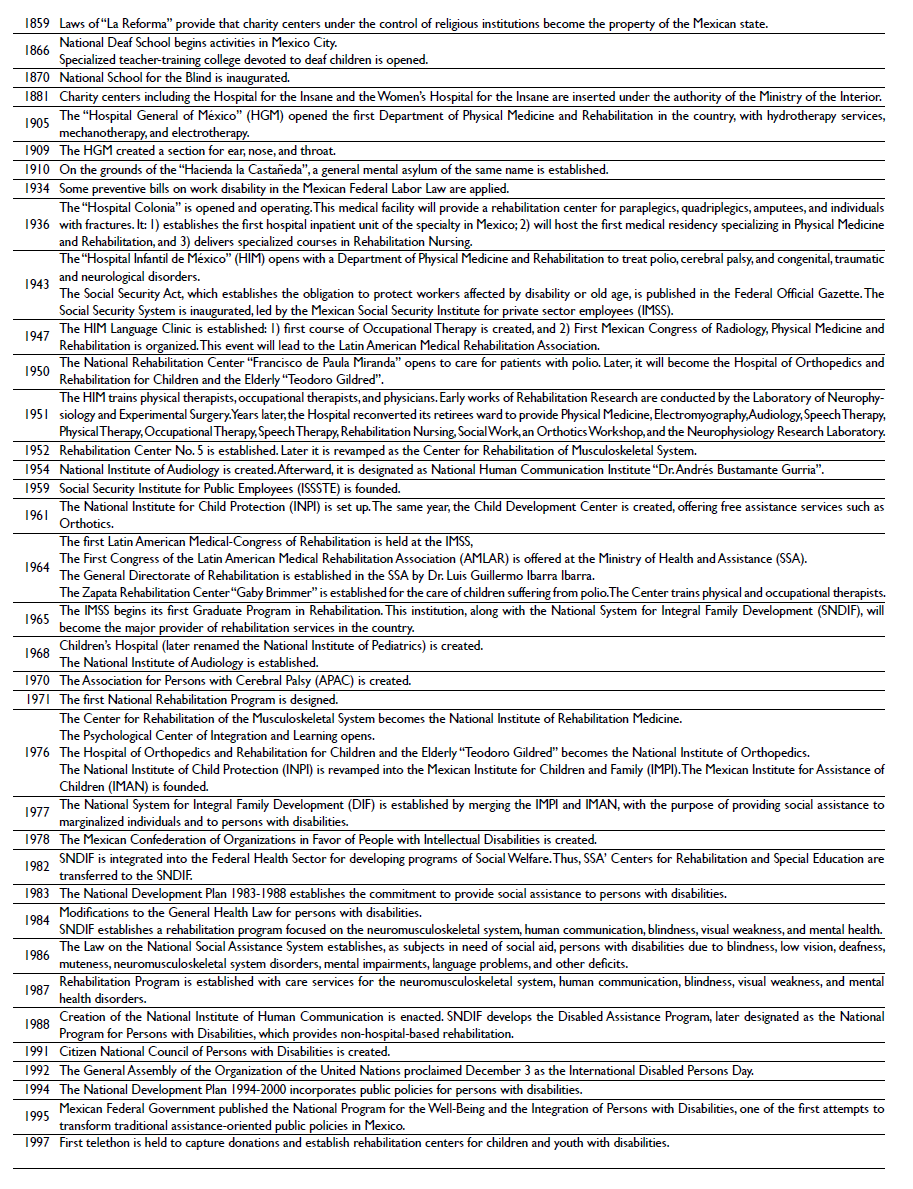
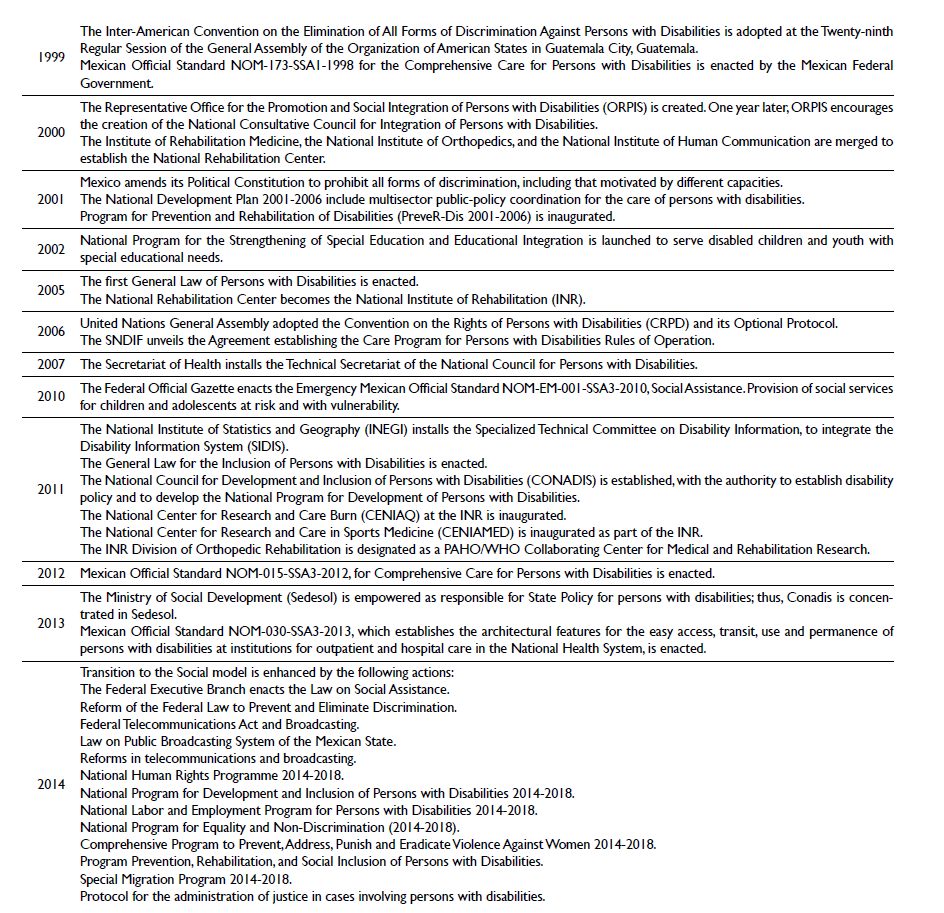
The use of timelines permits a graphic representation of the relative distribution of the major DM milestones for each period analyzed, as depicted in tables I, II, and III, in which the sequence of the items is highlighted by date, but the interval was omitted for simplicity. Time is represented from top to bottom, and from the past to the present.13
Discussion
Charity period
This period is the longest, but also the most difficult to document, given the scarcity of sources. Its antecedents comprise the pre-Hispanic Era, during which certain benign attitudes toward persons with disabilities deviate from the conventional characteristics of the charity DM, as documented by leading chroniclers of that time: Diego de Landa 18 and Juan de Torquemada.19 There are few references on eugenic practices, although it is possible to infer negative attitudes and exclusion towards persons with diversities11 and a sophisticated knowledge of the herbolary tradition.20
The charity model exhibits a better fit within the Colonial Era, with the emergence of welfare centers comprising a constellation of hospices, houses of mercy, orphanages, nursing homes, and hospitals,21 which represented the only chance of survival for the poorest individuals.22 The response to disability in this period is ambivalent: on the one hand, there was the discourse of compassion, applied through Christian charity, which considers that persons with diversities deserve compassion. On the other, there were exclusion and punishment practices, when disabilities were suspected to have a malefic origin, such as mental illness being attributed to witchcraft.23
The first timeline is mapped from the pre-Colombian Era to a year before the enactment of the Reform Laws, as depicted in table I. However, the prominent features of this DM have prevailed until the present, such as the following: 1) a range of stereotypes that identify persons with disabilities as objects of charity and compassion;24 2) practices of forced sterilization on girls, adolescents, and women with disabilities without their free and informed consent, and pressures to abort,24,25,26 and 3) strong social exclusion, now leading back to variables such as level of disposable income, age, gender, ethnicity, rurality, migratory status, educational level, employment characteristics, and disability type.24
Medical/rehabilitation period
Although it is difficult to establish the onset of this period accurately, its development is linked with the emergence of the Mexican secular state from the year 1859. Since that time, church property, including charity centers, became part of public property.27 Later, the term “charity” is replaced by the concept 28 of “public assistance”, provided to citizens by government institutions.
During this period, the religious causes of disability were left behind and a scientific etiology and medical treatments were imposed. As illustrated in table II, care for motor disabilities is stressed, deriving from a strong boost starting during the 1950s, 29 due to the need of caring for children affected by the polio epidemics at that time in the country 27,30 (table II).
By emphasizing their deficits and alterations during this period, persons with disabilities were often perceived as dependent and inferior from a biological perspective; thus, they were labeled as disabled or handicapped, notwithstanding the scientific progress achieved.31 Also, a link was established between disability and welfarism under a paternalistic concept. This perception was institutionalized through coercive policies 29 and legal practices such as substitution, where persons with severe disabilities were subject to procedures of interdiction.32
From this period, the following endure until the present: 1) a model of “special” education and barriers to accessibility in schools;24 2) the difficulty of eradicating the practice of substitution, and 3) legislation that continues to enforce the internment of persons with intellectual and psychosocial disabilities,24 without respecting their free and informed consent.
Social period
Again, there is no consensus on the exact date of onset of this period, which was characterized by greater legal recognition of inclusion and acceptance of diversity and the rights of persons with disabilities, starting from the signing of international treaties and amendments to the Mexican Political Constitution 33 (table III).
The transition that was underway formed part of the mainstreaming of human rights in public policy, which seeks to conceptualize disability as a collective subject. Within this context, society has a responsibility of not placing or allowing barriers to exist that discriminate or impede the full enjoyment of the rights of persons with disabilities.12
The social model faces the following difficulties to date:24 1) a legislative framework on accessibility that does not include all aspects established in the Convention on the Rights of Persons with Disabilities; 2) a lack of regulation, monitoring mechanisms, a national accessibility plan (and another for situations-of-risk and humanitarian emergencies), with an emphasis on persons with diversities; 3) the low employment rate of people with disabilities and noncompliance with the labor quota of 3% in the government; 4) lack of updated statistics on disability and information on these persons’ current situation,34 and 5) denial of the right to vote for persons with acute intellectual and psychosocial disabilities, in addition to the lack of accessibility alternatives to voting.24
Conclusion
The three DM analyzed should be used only as conceptual categories. The timeline method applied shows that DM are not historical periods, nor sequential chronologies, because of the following: 1) there is a prevalence of characteristic features of each DM in the current situation, and 2) some of their features overlap, thus frontiers between periods cannot be established precisely; therefore, start and end dates are unreliable.
DM should not be employed to presuppose evolutionary historical steps, assuming that a period represents an improvement or completion over the previous one, in terms of progression. This last approach leads to teleological interpretations of the history of disability 35 that minimize the serious complications present up to the present day, such as discrimination and substitution practices.
The timelines depicted suggest that the care of disabilities in Mexico requires a reconfiguration to a less unequal and more inclusive system, aligned with the principles and assumptions of social DM, which require strengthening. To date, disability healthcare comprises a constellation of four fragmented and heterogeneous disability healthcare subsystems,36,37 which continue to exhibit strain due to the inherited inertia of the charity and medical/rehabilitation DM:
Private providers. While not offering inclusive comprehensive care for disabilities, these provide personalized services to the population with economic solvency through a conglomerate of 28.6 privately owned hospitals per one million individuals, compared with 11.4 publicly owned hospitals.36
Social security system (SSS). Includes the Mexican Social Security Institute, for private sector employees (IMSS, by its Spanish acronym), the Social Security Institute for Public Employees (ISSSTE), the Institute of Social Security for the Armed Forces (ISSSFAM), the Ministry of Navy (Semar), Mexico’s national oil company (Petróleos Mexicanos, Pemex), and the healthcare services of the state governments (SESA).
The SSS provides full disability healthcare benefits for public and private employees (including pensioners) and their households (such as paid sick days, retirement plans, and so forth). Funded by both the Mexican Federal Government and by contributions from employees and their employers, SSS encompasses a heterogeneous array of independent healthcare institutions.
Public insurance subsector. A set of agencies financed by the Mexican Federal Government, state governments, and/or individuals. It covers non-salaried, informal workers, and unemployed and rural persons without affiliation with the SSS. Main Institutions in this group include the following: 1) Ministry of Health (through the National Institute of Rehabilitation Luis Guillermo Ibarra Ibarra, and certain rehabilitation services offered by other National Institutes of Health, High Specialty Hospitals, and programs such as “Health Caravans”); 2) National Commission of Social Protection for Health, also referred to as “Seguro Popular”. This agency protects the poorest persons with some disabilities through a restricted package of services with fewer benefits, and omits important treatments of secondary and tertiary care,36 not providing benefits against temporary or permanent disability; 3) “Different Community” Program and “Care Program for Persons with Disabilities” of the National System for Integral Family Development (SNDIF); 4) Special Basic Community Healthcare Programs for the Uninsured, such as the IMSS-Prospera Program and Seguro Médico Siglo XXI-IMSS, among others.
Non-profit organizations. Civil societies, civil associations and private assistance institutions (IAP) that offer rehabilitation and orthopedics.

